Microbial Preseptal and Orbital Cellulitis
Michael T. Yen
Seongmu Lee
Preseptal cellulitis is the term used to describe eyelid infections anterior to the orbital septum. Orbital cellulitis is the term used to describe infections involving the soft tissues posterior to the orbital septum. In contrast to the more common preseptal cellulitis, orbital cellulitis may be associated with severe vision- and life-threatening complications, including optic neuropathy, cavernous sinus thrombosis, meningitis, or intracranial abscess formation.1,2 While both preseptal and orbital infections may develop from a number of etiologies, including trauma, retained orbital foreign body, and extension of infection from ocular and adnexal structures, the most frequent cause of preseptal and orbital cellulitis is secondary extension of infection and/or inflammation from the paranasal sinuses.3 Both types of infections are much more common in the pediatric age group than in adults, and the infection is usually bacterial in origin, unless the patient is immunocompromised and at a higher risk for developing an invasive fungal infection.
In the early 20th century, without the benefit of modern day antibiotics or advanced radiographic imaging, most patients with orbital cellulitis were treated with nasal packs soaked in epinephrine or ephedrine.4 Surgical drainage of abscesses was delayed as late as possible until there was subconjunctival or subcutaneous pointing. Even with these limited therapeutic options, many patients had spontaneous recovery. However those patients that did not have spontaneous recovery often had severe complications such as blindness or death. In 1908, Birch-Hirschfeld reported a 17% mortality rate in patients with orbital cellulitis from meningitis, cerebral abscess, or cavernous sinus thrombosis.4 Over the past century, the introduction of antibiotic therapy and improvements in diagnostic technology and surgical techniques has greatly reduced the mortality and morbidity of orbital cellulitis. Despite these advances, however, the management of preseptal and orbital cellulitis remains challenging. Preservation of ocular function and prevention of ocular and systemic complications require a thorough understanding of the causes and pathogenesis of each of these conditions. Proper management necessitates prompt recognition of the clinical features, obtaining appropriate laboratory investigations, timely initiation of antibiotic therapy, and selected surgical intervention.1 The successful management of preseptal and orbital cellulitis may require a multidisciplinary approach with close communications between the ophthalmologist, otolaryngologist, neurosurgeon, radiologist, pediatrician, and infectious disease consultant.
ANATOMIC FACTORS
The orbital septum is a thin multilaminated fibrous structure originating from the orbital rims where it meets with the periosteum lining the facial bones and the periorbita lining the orbital walls to form the arcus marginalis.5 From the superior arcus marginalis, the orbital septum extends inferiorly in the upper eyelid until it fuses with the levator aponeurosis or inserts onto the anterior surface of the upper eyelid tarsus (Fig. 25.1). From the inferior arcus marginalis, the orbital septum extends superiorly in the lower eyelid until it inserts along the inferior border of the inferior tarsal plate.6 The anterior periorbita is relatively loosely adherent to the bony orbit and can allow abscess material to spread within the subperiosteal space. The intermuscular septa extend from one rectus muscle to the next and from the insertions of the muscles to their origins at the annulus of Zinn posteriorly. Thus, the four rectus muscles and their intermuscular septa establish an anatomic cone that divides the orbit into intraconal and extraconal compartments (Fig. 25.2). In the posterior orbit, the fascia between the rectus muscles is thin and often incomplete, and distinct compartments may be lacking.7 Therefore, orbital abscesses located within the orbit but outside of the subperiosteal space may extend between the intraconal and extraconal orbital spaces.
The paranasal sinuses surround three sides of the orbit and are the most common underlying infections source for preseptal and orbital cellulitis (Fig. 25.3).8,9,10,11 The medial orbit is a common location for orbital abscesses secondary to an adjacent sinusitis. The bony wall separating the medial orbit from the adjacent ethmoid sinus is extremely thin, especially in early childhood, and infections or inflammatory processes in the ethmoidal air cells can easily spill over into the medial orbit. The orbital floor is also comprised of relatively thin bone and is a location prone to the development of a subperiosteal abscess from an adjacent maxillary sinusitis. The frontal sinus lies above the orbit, and although the bone of the orbital roof is relatively thick, abscess of the superior orbit can develop with severe infections of the frontal sinus. Since the frontal sinus is also adjacent to the frontal lobe of the brain, infections of this sinus can also lead to meningitis, epidural and subdural abscesses, and even intracerebral abscesses.12 The sphenoid sinus is adjacent to the orbital apex and optic canals, and infections of this sinus can lead to significant visual loss even without the development of a subperiosteal or intraorbital abscess. There are no sinuses directly adjacent to the lateral orbital wall. Although subperiosteal abscesses can rarely develop or extend into the lateral orbit, other noninfectious processes such as inflammatory dacryoadenitis should be considered when a fluid space is identified in this area on radiographic imaging.
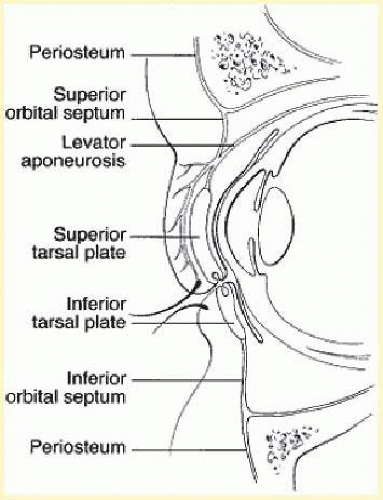 FIG. 25.1 The superior orbital septum extends from the arcus marginalis of the orbital rim to the levator aponeurosis. In the lower lid the orbital septum inserts along the inferior edge of the tarsal plate. |
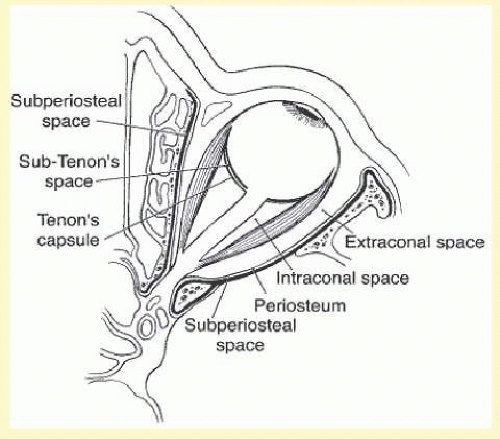 FIG. 25.2 Within the orbit, the four rectus muscles and their intermuscular septa constitute an anatomic cone that establishes two separate compartments: intraconal and extraconal. |
The orbital veins are without valves and therefore can allow passage of infectious processes in both anterograde and retrograde directions. The venous drainage of the middle third of the face and of the paranasal sinuses is mostly via the orbital veins, and then inferiorly into the pterygoid plexus, or posteriorly into the cavernous sinuses (Fig. 25.4). A septic process of the cavernous sinus may involve any of the structures located within, including the oculomotor nerve, the trochlear nerve, the trigeminal nerve, the abducens nerve, the internal carotid artery, and orbital sympathetic nerves (Fig. 25.5). Such an infection can also extend to the contralateral cavernous sinus, the pituitary gland, the surrounding meninges, and the parameningeal spaces.13
CLASSIFICATION
In 1937, Hubert14 categorized the orbital complications of acute sinusitis. This classification was modified by Smith and Spencer3 in 1948 and by Chandler et al.9 in 1970. Although this scheme does not dictate chronologically successive stages of preseptal and orbital cellulitis, it may have some usefulness in directing the management of these conditions. Group I is preseptal cellulitis. Group II is orbital cellulitis without the presence of an orbital abscess. The remaining three groups all represent orbital cellulitis with some form of abscess formation: group III includes a subperiosteal orbital abscess, group IV includes an intraorbital abscess, and group V includes cavernous sinus thrombosis (septic abscess) (Fig. 25.6). Although an adjacent sinusitis is the most common cause, other mechanisms such as endogenous spread, trauma, or retained orbital foreign bodies may also lead to preseptal and orbital cellulitis.
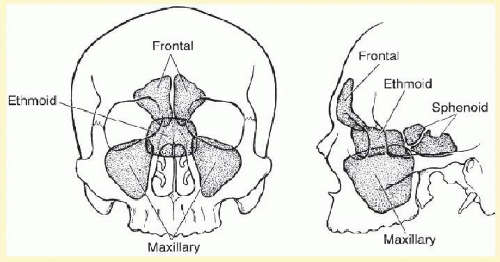 FIG. 25.3 The paranasal sinuses surround three sides of the orbit. Most orbital cellulitis is due to ethmoid sinusitis. |
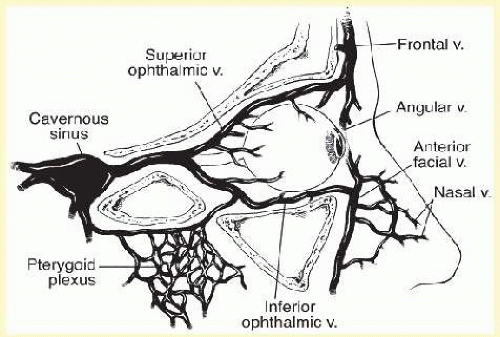 FIG. 25.4 The orbital veins drain posteriorly into the cavernous sinus and interiorly into the pterygoid plexus. |
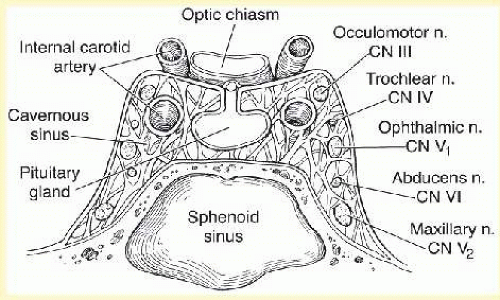 FIG. 25.5 The cavernous sinuses lie on either side of the pituitary gland, above the sphenoid sinus and below the optic chiasm. |
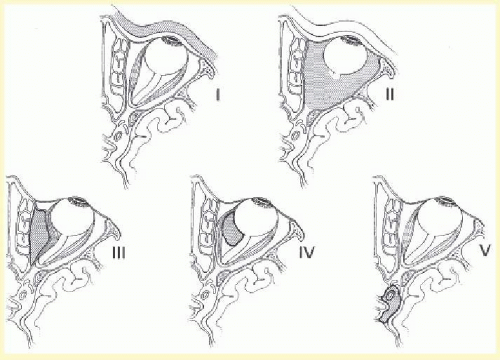 FIG. 25.6 Chandler’s classification of the orbital complications of acute sinusitis. Group I is preseptal cellulitis, and group II is orbital cellulitis. The remaining groups are all abscesses: group III is subperiosteal abscess, group IV is intraorbital abscess, and group V is cavernous sinus thrombosis (septic abscess). |
Preseptal cellulitis is much more common than orbital cellulitis, and it is also associated with a much better prognosis.1 Although by definition the orbital tissues are not involved with preseptal cellulitis, visual loss can still result, such as when prolonged eyelid edema leads to occlusion amblyopia in young children. Orbital cellulitis is associated with higher morbidity than preseptal cellulitis; however, the presence and location of an orbital abscess do not necessarily correlate with severity of infection or prognosis.15 All patients with preseptal and orbital cellulitis require treatment with systemic antibiotics. When an orbital abscess is present, surgical drainage may be necessary in patients not improving with antibiotics alone, in patients with retained foreign bodies, in patients with impending visual loss, or in patients with concurrent cavernous sinus or intracranial involvement.16,17
PROBLEM-SOLVING ALGORITHMS
The initial management of acute preseptal and orbital cellulitis is simplified by recognition of the distinctive signs, the principal risk factors, and the most likely responsible organisms involved. Proper management of these entities can prevent loss of vision and can help obviate life-threatening intracranial complications (Fig. 25.7).18,19
Preseptal and orbital cellulitis usually present with eyelid inflammation and tissue distention (Fig. 25.8). There are several clinical findings that can be useful in differentiating between these two conditions. A careful ophthalmologic examination is essential, including visual acuity, evaluation of the ocular adnexa, pupil reaction, ocular motility, biomicroscopy of the anterior segment, tonometry, and ophthalmoscopy. The ocular examination should be as complete as the clinical setting permits. The most distinctive features of orbital cellulitis are proptosis and limitation of ocular motility; useful but variable additional signs are conjunctival inflammation with chemosis, orbital pain, reduced visual acuity, and afferent pupillary defect (Table 25.1). If the clinical signs suggest orbital involvement, immediate radiographic imaging with computed tomography (CT) or magnetic resonance imaging (MRI) should be performed to confirm the diagnosis of orbital cellulitis and assess for the presence of an abscess and the degree of orbital tissue involvement. CT scans provide rapid imaging of the paranasal sinuses and orbit (Fig. 25.9). The imaging should be performed with contrast enhancement to differentiate between true abscess formations from inflammatory phlegmatous involvement or orbital tissues. MRI may provide improved imaging of intracranial involvement or retained orbital foreign bodies. CT or MRI scans should also be considered in cases of preseptal cellulitis if there is a history of trauma with the possibility of a retained foreign body.
Preseptal cellulitis can be caused by seemingly minor trauma or by blunt trauma. If the history suggests a possible foreign body injury, imaging should be obtained to identify any orbital injury or retained foreign bodies. Abscess formations in posttraumatic preseptal cellulitis are usually caused by Staphylococcus aureus or Streptococcus pyogenes. When a foreign body or an eyelid abscess is identified, management usually requires surgical debridement, drainage, and microbiologic evaluation of the material obtained. Appropriate antibiotic therapy should be initiated and modified depending on the interpretation of the Gram stain and culture and sensitivity results. In the absence of trauma or retained foreign bodies, the most likely cause of preseptal cellulitis in the United States is Streptococcus pneumoniae.20,21 In developing countries, in nonimmunized persons, and in immunocompromised patients, Haemophilus influenzae type B should be suspected. Upper respiratory infection or otitis media are present in approximately one half of such children. Appropriate treatment may be intravenous antibiotics in young children or patients with signs of sepsis. Older children who have mild cases without systemic disease are often treated with oral antimicrobials. Adjunct corticosteroids can be considered if an abscess forms and the patient is also being treated with broad-spectrum antibiotics.
When orbital cellulitis is suspected, a CT or MRI scan should be obtained, and the treatment program started promptly. Orbital imaging is the most effective method for differentiating orbital cellulitis from other causes of inflammatory orbital proptosis (Table 25.2). Once orbital cellulitis is confirmed, additional evaluation of the imaging should identify potential sources of the infection. For example, the most common cause of orbital cellulitis is secondary extension of infection from an adjacent sinusitis.16 In these cases, the affected sinus should be readily identified on the CT or MRI scan. If the cellulitis originated from infection of an adjacent adnexal structure (such as endophthalmitis or dacryocystitis), the sinuses may be clear, but the infectious source should be readily identified (Figs. 25.10 and 25.11).2,22 If there is a retained orbital foreign body, or if the cellulitis is felt to have originated from the nasolacrimal sac or the globe, surgery should be performed promptly (Fig. 25.12). If the orbital cellulitis originates from an adjacent sinusitis or endogenously, then medical therapy should be initiated first, even if an abscess is present. Additionally, aggressive nasal hygiene should also be prescribed.23 The most common bacteria identified in sinusitis are Streptococcus pneumoniae, nontypeable H. influenzae, other streptococci, and Staphylococcus aureus. Anaerobes may also play a significant role. In patients who do not respond to medical therapy alone, have impending visual loss, or have concurrent intracranial involvement, surgical drainage of the abscess should be considered.17
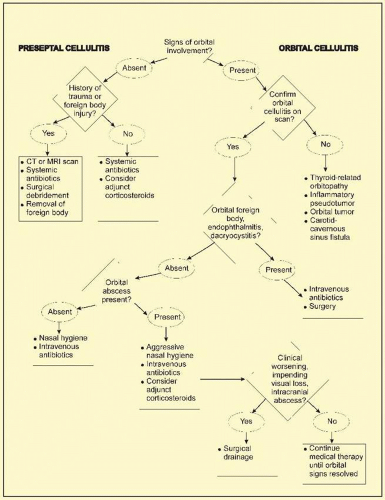 FIG. 25.7 Summary algorithm for preseptal and orbital cellulitis. |
Finally, in the case of an immunosuppressed patient, one must consider the possibility of fungal disease, primarily mucormycosis or aspergillosis, despite the rarity of these infections.24,25,26 Neuro-ophthalmologic signs, particularly the orbital apex syndrome (i.e., dysfunction of cranial nerves II, III, IV, and VI and of the ophthalmic division of V) in the presence of reduced host defenses, such as metabolic acidosis or immunosuppression, suggest mucormycosis and should prompt a search for necrotic tissue. A biopsy for histopathology and culture should be done if such a lesion is found. Aspergillosis, often occurring in otherwise apparently healthy patients, is suggested by similar signs but has a more chronic course. Treatment of both conditions includes intravenous and local antifungal therapy and often involves extensive surgical debridement.
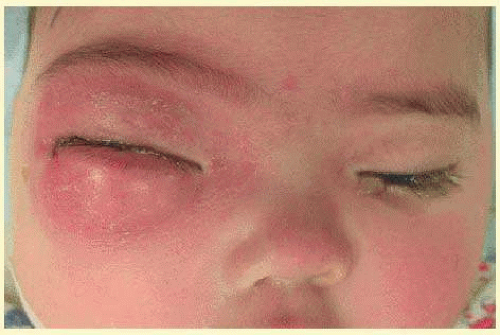 FIG. 25.8 Patient with right orbital cellulitis presenting with severe eyelid edema and erythema associated with proptosis. |
PRESEPTAL CELLULITIS
By definition, preseptal infections do not involve the globe or the orbital tissues around the eye. However, preseptal cellulitis can still lead to visual dysfunction, especially in very young children where prolonged eyelid edema may lead to occlusion amblyopia. Furthermore, any preseptal infection can progress posteriorly to the orbit if improperly diagnosed or inadequately treated. It is also important to remember that preseptal cellulitis may be the first sign of sinusitis, which can progress to significant orbital and intracranial disease.27
TABLE 25-1 Distinguishing Features of Bacterial Preseptal and Orbital Cellulitis | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
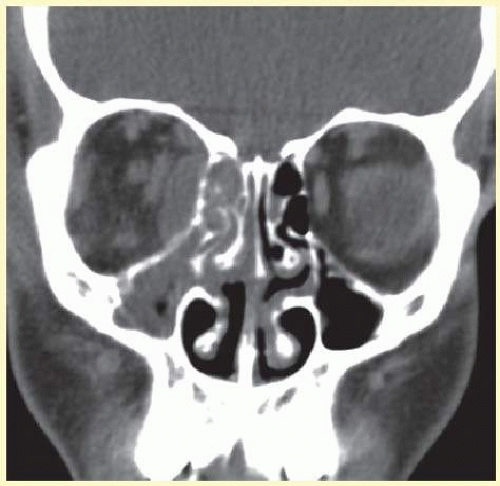 FIG. 25.9 A coronal CT scan reveals pansinusitis of the right side with an adjacent subperiosteal abscess along the right medial orbital wall. |
Before the widespread availability of appropriate vaccines, preseptal cellulitis in children was commonly caused by H. influenzae type B.28,29 H. influenzae type B can cause severe, life-threatening infections in children, including meningitis, epiglottitis, bacteremia, pneumonia, arthritis, and cellulitis. Before 1990, approximately 18,000 cases of severe H. influenzae infection occurred annually in the United States among children younger than 5 years of age, and every year, 900 to 1,200 of such cases were fatal.30 H. influenzae type B causes two principal forms of soft tissue infections: preseptal cellulitis and buccal cellulitis. These two forms share several epidemiologic and clinical features, notably peak incidence in winter months, predominance in children aged 4 to 12 months, a violaceous tender swelling of the involved soft tissues, and concurrent bacteremia. The pathogenesis of H. influenzae buccal cellulitis is uncertain. The principal theories are (1) lymphatic spread from ipsilateral otitis media or from the nasal passages, (2) hematogenous spread from another site, or (3) invasion of the organism across the mucous membrane of the oropharynx.31,32 Most serious H. influenzae type B infections occur between the ages of 6 months and 2 years. Before age 6 months, infants are partially protected by passively acquired maternal antibodies. Natural antibodies to the capsular polysaccharide of H. influenzae type B develop between the ages of 18 and 24 months in nonimmunized children. Since December 1993, several vaccines for H. influenzae type B have been approved for use in the United States.33 The use of these vaccines has now resulted in a marked reduction in the number of cases of cellulitis caused by this organism.34 In developing countries and in locations where the vaccines are not widely available or adequately used, it is still possible to find frequent cases of type B H. influenzae infections. In the United States, the most common bacterial agent identified in preseptal cellulitis in children is now Streptococcus pneumoniae followed by Staphylococcus aureus and Streptococcus pyogenes.20,21 Polymicrobial infections may occur, especially if a wound remains open. Anaerobic, non-spore-forming bacteria, such as Peptococcus, Peptostreptococcus, and Bacteroides, are associated with infections following human or animal bites. Contamination with soil can produce myonecrosis with gas gangrene or tetanus due to clostridial infection.35
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


