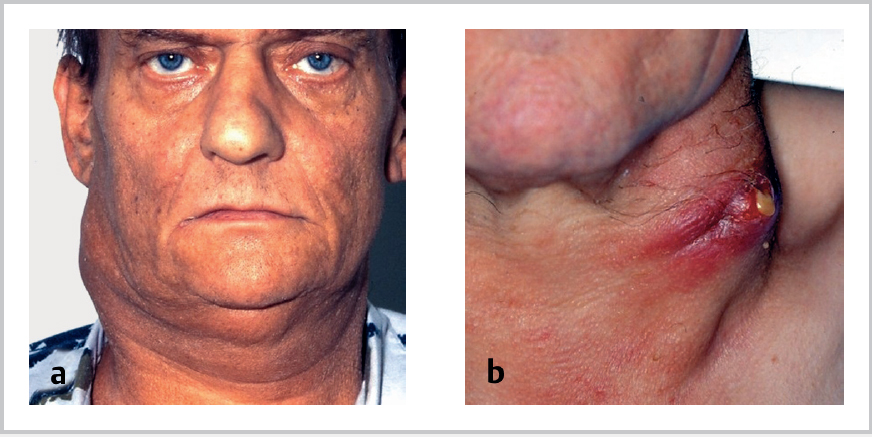
59 Metastatic Neck Disease • Anterior • Posterior • Circular collection of lymphoid tissue aggregates within pharynx at skull base • Superficial nodal system • Drains • Deep structures drain directly or through superficial system • Jugular trunks form from confluence of deep lymphatics • I • II = oral cavity, pharynx, supraglottic larynx • III = thyroid, larynx, hypopharynx, cervical oesophagus • IV = intra-abdominal organs, breast, lung, oesophagus, thyroid • V = nasopharynx, thyroid, oesophagus, lung, breast • VI = anterior compartment (visceral) group, e.g., para- and preotracheal LNs • VII = upper anterior mediastinum • N1—mets in single ipsilateral node £3 cm diameter Fig. 59.1a,b a Lymph-node metastases are solid, indolent, and fixed to the surrounding tissue. b Exulceration of the metastases produces haemorrhagic secretion and often an inflamed reaction in the surrounding skin. • N2—3 to 6 cm • N3—>6 cm diameter • >1 cm diam • Rim enhancement following IV contrast • Central necrosis • See Figs. 59.1 and 59.2 • Arguments for elective surgery Table 59.1 Incidence of neck metastases
59.1 Triangles of the Neck
 Submental
Submental
 Submandibular
Submandibular
 Carotid
Carotid
 Muscular
Muscular
 Occipital
Occipital
 Subclavian
Subclavian
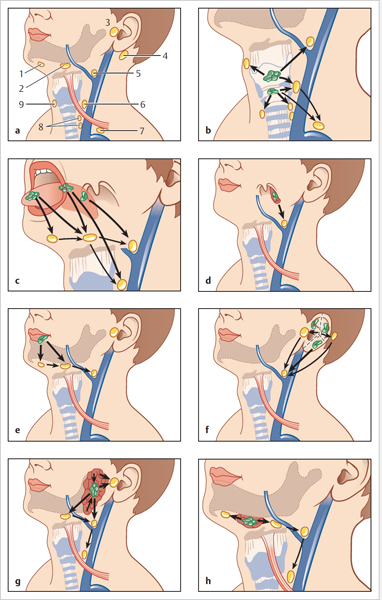
59.2 Head and Neck Lymphatics
59.2.1 Waldeyer Internal Ring
 Adenoids
Adenoids
 Tubal and lingual tonsils
Tubal and lingual tonsils
 Palatine tonsils
Palatine tonsils
 Aggregates of lymphoid tissue on posterior pharyngeal wall
Aggregates of lymphoid tissue on posterior pharyngeal wall
59.2.2 Waldeyer External Ring
 Occipital
Occipital
 Postauricular
Postauricular
 Parotid
Parotid
 Preauricular
Preauricular
 Buccal/facial
Buccal/facial
 Superficial cervical
Superficial cervical
 Submandibular
Submandibular
 Submental
Submental
 Anterior cervical
Anterior cervical
 Skin
Skin
 Scalp
Scalp
 Eyelids
Eyelids
 Face
Face
 Waldeyer internal ring
Waldeyer internal ring
 Sinuses
Sinuses
 Oral cavity
Oral cavity
59.2.3 Deep System (Cervical Lymph Nodes)
 Junctional
Junctional
 Upper cervical
Upper cervical
 Middle cervical
Middle cervical
 Lower cervical
Lower cervical
 Spinal accessory group
Spinal accessory group
 Nuchal
Nuchal
 Visceral
Visceral
 Upper mediastinal
Upper mediastinal
 On right ends at junction of IJV and brachiocephalic vein or joins right lymphatic duct
On right ends at junction of IJV and brachiocephalic vein or joins right lymphatic duct
 On left joins thoracic duct
On left joins thoracic duct
59.2.4 Drainage by Level
 Submental = lower lip, floor of mouth, lower gum
Submental = lower lip, floor of mouth, lower gum
 Submandibular = face, nose, sinuses, oral cavity, SMG
Submandibular = face, nose, sinuses, oral cavity, SMG
59.2.5 Nodal Classification in Malignancy
 N2a—single ipsilateral node
N2a—single ipsilateral node
 N2b—multiple ipsilateral nodes
N2b—multiple ipsilateral nodes
 N2c—bilateral/contralateral nodes
N2c—bilateral/contralateral nodes
59.2.6 Suspicious Imaging Features
 Spherical shape
Spherical shape
59.3 Features of Metastatic Neck Disease
59.4 The N0 Neck
 High incidence of occult metastatic disease (Table 59.1)
High incidence of occult metastatic disease (Table 59.1)
| Subsite | % Risk of neck metastases |
| Oral cavity | >20% |
| Glottis | 0–15% |
| Supraglottis | 8–30% |
| Oropharynx | >50% |
| Hypopharynx | >50% |
 Limited neck dissection has low morbidity and mortality
Limited neck dissection has low morbidity and mortality
 If primary lesion has to be removed from the neck, en-bloc resection is preferable
If primary lesion has to be removed from the neck, en-bloc resection is preferable
 No clinical ability to detect conversion of N0 to N1
No clinical ability to detect conversion of N0 to N1
 Allowing neck mets to develop increases incidence of distant mets
Allowing neck mets to develop increases incidence of distant mets
 Cure rate for neck dissection decreased if gland enlargement occurs or multiple nodes appear
Cure rate for neck dissection decreased if gland enlargement occurs or multiple nodes appear
• Arguments against elective surgery
 Cure rates are no lower in the N1 neck
Cure rates are no lower in the N1 neck
 Careful clinical follow-up will allow detection at earliest conversion from N0 to N1
Careful clinical follow-up will allow detection at earliest conversion from N0 to N1
 Radiation is as effective as neck dissection for non-palpable disease
Radiation is as effective as neck dissection for non-palpable disease
 Elective neck dissection results in a large number of unnecessary surgical procedures
Elective neck dissection results in a large number of unnecessary surgical procedures
 Removes barrier to spread of disease and may have detrimental immunological effect
Removes barrier to spread of disease and may have detrimental immunological effect
• Indications for elective neck treatment
 > 20 to 25% chance of subclinical disease
> 20 to 25% chance of subclinical disease
 Vigilant follow-up is not possible
Vigilant follow-up is not possible
 Clinical evaluation of neck is difficult
Clinical evaluation of neck is difficult
 Surgery is being performed for access or reconstruction
Surgery is being performed for access or reconstruction
 Imaging suggests possible occult nodal spread
Imaging suggests possible occult nodal spread
• Contraindications to neck dissection:
 Primary tumour untreatable
Primary tumour untreatable
 Unfit for major surgery
Unfit for major surgery
 Inoperable neck disease inc. carotid encasement and skull base/intracranial involvement
Inoperable neck disease inc. carotid encasement and skull base/intracranial involvement
59.5 Radiotherapy for Metastatic Neck Disease
• Clinically negative neck (N0)
• Clinically positive neck
• Electively after surgery
 Node-positive disease
Node-positive disease
 Other risk factor for local recurrence inc. extracapsular spread
Other risk factor for local recurrence inc. extracapsular spread
• Neck disease developing or recurring after initial treatment:
 Nodal mets developing in untreated neck after initial treatment of primary tumour alone
Nodal mets developing in untreated neck after initial treatment of primary tumour alone
 Recurrence after previous surgery to neck
Recurrence after previous surgery to neck
 Nodal recurrence after combined treatment
Nodal recurrence after combined treatment
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


