21

Meningoencephaloceles and
Cerebrospinal Fluid Leak
Although cerebrospinal fluid (CSF) leaks and meningoencephaloceles are uncommon problems facing the nasal sinus surgeon, their consequences are significant and may even be catastrophic. These intracranial and sinus-related problems may be congenital, idiopathic, traumatic, or iatrogenic. Many nasal and sinus surgeons have the ability and technology to endoscopically diagnose and manage meningoceles, meningoencephaloceles, and cerebrospinal fluid leak. Office nasal endoscopy and intraoperative endoscopy with image-guided triplanar localization surgery have advanced the success in managing these problems and reduced the morbidity and mortality for the patient. Many physicians now feel that an intranasal endoscopic approach is warranted as a first try for the majority of patients with pathology arising in the anterior cranial fossa and extending into and involving the paranasal sinuses.
 Cerebrospinal Fluid Leak
Cerebrospinal Fluid Leak
Since World War I CSF leakage has been described as traumatic or nontraumatic.1 Approximately 90% of CSF rhinorrhea is traumatic in origin, and the trauma may be surgically or nonsurgically induced. Nonsurgical trauma is usually from blunt or projectile injury and is generally associated with other intracranial injuries. Surgical trauma is usually from intracranial surgery, pituitary surgery, or paranasal sinus surgery. One to 3% of head trauma will have CSF leaks.2 Over two-thirds of traumatic CSF leaks stop within the first month. CSF otorrhea has a greater chance of spontaneous resolution than sinus and/or paranasal rhinorrhea.2–4 Consideration is given to repairing post-traumatic CSF leaks if there is still active leaking after 14 days especially because prophylactic antibiotics do not always prevent meningitis.5 The most common nasal and paranasal sinus locations for CSF leakage are the frontal sinus, cribriform plate, and sphenoid sinus.
Nontraumatic sources of CSF leak are from the cribriform plate, sella turcica, sphenoid sinus, or posterior ethmoid sinus. Nontraumatic causes of CSF leak are divided into normal pressure and high pressure. Females are more affected than males, and most often the spontaneous rhinorrhea begins with a sneeze, cough, or straining. About 45% of spontaneous leaks are from high pressure. High pressure in the subarachnoid space probably forces spinal fluid through a weakened area such as the cribriform plate. Slow-growing tumors (usually pituitary) account for 84% of high-pressure CSF rhinorrhea. The remaining cases of CSF rhinorrhea are related to hydrocephalus.6
Normal-pressure CSF leaks account for 55% of spontaneous leaks. These are usually caused by slow erosion of the skull base associated with intracranial tumors, mucoceles, osteomata, and nasal and/or sinus neoplasms (nasopharyngeal angiofibromaa, nasopharyngeal carcinomas), or through congenital pathways (craniopharyngeal canal, meningoencephaloceles), hydrocephalus, or low-pressure flow as with bony erosion, seller atrophy, olfactory atrophy, congenital anomalies, and idiopathic.6
The preoperative CT scan provides data helpful in the prevention of CSF leaks. Critical areas to look at are the roofs of the ethmoid sinus and the cribriform plate. It is important to look at the level of the cribriform plate and the relationship to the roof of the ethmoid sinus. The cribriform plate is generally lower than the roof of the ethmoid sinus but may be lower by several millimeters. Ideally, axial, coronal, and sagittal CT scans are needed to have the most complete views of the sinuses. The axial CT provides valuable information about the anteroposterior dimension of the frontal and sphenoid sinuses. The sagittal view provides information about the height and roof of the ethmoid and sphenoid sinus. For difficult cases where the pathology has altered the anatomy or in revision surgery, image-guided technology is helpful in minimizing the chances of trauma.
To minimize the chances of intraoperative trauma causing CSF leak, it is important to consider the areas to avoid, proper instrumentation, and surgical technique.
There are a few common places where intracranial violation of the nasal sinus cavity occurs during sinus surgery. Each of these relates to the anatomical features of that area. One of the most common areas is the junction between the middle turbinate and the roof of the ethmoid sinus. Here the bone is generally quite thin (Fig. 21–1). It is apparent on many CT scans that there is a thicker bony plate forming the majority of the middle turbinate; however, the bone becomes very thin superiorly near the attachment. The roof of the ethmoid sinus is generally higher than the nasal cavity roof (cribriform plate) (Fig. 21–2). The attachment of the middle turbinate to the roof of the fovea ethmoidalis is not a simple vertical attachment. Rather, the middle turbinate tends to slope slightly laterally in this area, narrowing the region. This puts this bone at risk because of the sloping and thinness and because there frequently are polyps present in this region that may have altered the anatomy.
The area of the cribriform plate is a potential area for injury. Although the bone is generally thicker than the fovea ethmoidalis, it is perforated by the olfactory fibers, and the dura is tightly adherent. The lateral cribriform plate is especially vulnerable in the region of the anterior ethmoid artery. This is one of the areas of least resistance in the anterior skull base.7
Another area at risk for injury is the junction of the posterior ethmoid sinus air cells and the front wall of the sphenoid sinus. The bone of the anterior sphenoid wall is generally very thin, making this region vulnerable to injury. This area may be injured in following the ethmoid sinus air cells posteriorly and inadvertently working superiorly (Fig. 21–3). Injury also may occur in trying to open the front face of the sphenoid sinus.
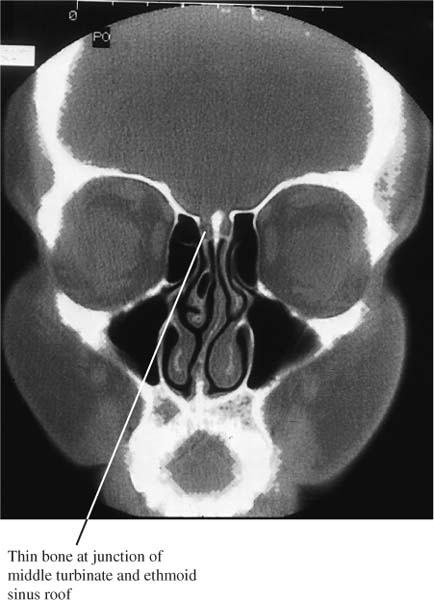
FIGURE 21–1 Thin bone at the junction of the fovea ethmoidalis of the ethmoid sinus and the middle turbinate is an area of injury causing CSF leak.

FIGURE 21–2 Care must be taken when operating in the region of the ethmoid sinus roof and cribriform plate. The roof of the ethmoid sinus is higher than the cribriform plate; therefore, knowing the location of one does not ensure knowing the location of the other.
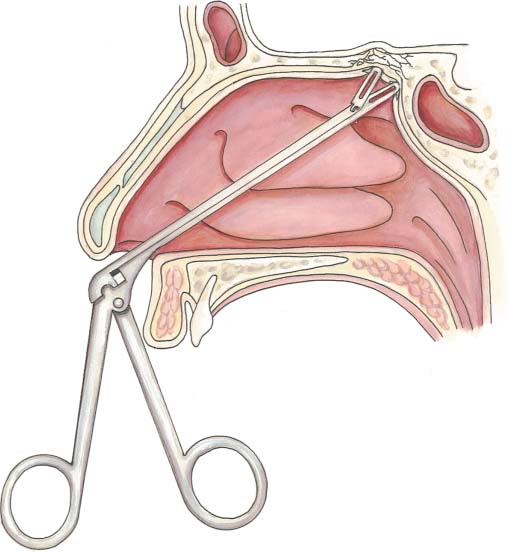
FIGURE 21–3 Injury may occur at the junction of the ethmoid sinus roof and the anterior face of the sphenoid sinus, causing CSF leak.
Proper choice and use of surgical instruments help to avoid trauma to the roof of the sinus and nasal cavity. Typical instruments for traditional and endoscopic sinus surgery have been grasping forceps and curettes. Curettes have been used in the removal of the air cell partitions of the ethmoid sinus. Removal of bone with curettes can inadvertently fracture the bone into the roof either exposing dura or lacerating dura and creating a CSF leak.
CONTROVERSY
This author does not use curettes because of the seemingly increased risk for injury when working along the fovea ethmoidalis. In this region, small spicules of bone extending down from the fovea ethmoidalis from ethmoid air cell partitions may be fractured with a curette and cause injury to the sinus roof. In the past, soft tissue–type cup forceps have been used to remove polyps and thin bony partitions. These have the tendency to tear mucosa. This has the potential of tearing bone along with the mucosa and creating an injury. Newer micro-powered endoscopic instruments preserve mucosa and create a delicacy when coupled with endoscopes and accuracy when combined with image-guided triplanar surgical localization.



