14
Meniett Device and Chemical Labyrinthectomy for Unilateral Cochleovestibular Meniere’s Disease
Meniere’s disease is a common inner ear disorder of unknown etiology that is associated with symptoms of episodic vertigo and fluctuant hearing loss, tinnitus, and ear pressure. The disorder is initially unilateral in over 90% of cases. The vertigo attacks vary from moderate to incapacitating, preventing normal daily activity at times. The unpredictability of vertigo attacks contributes additional stress, which may further exacerbate the condition. The high prevalence of Meniere’s disease1 and time lost from work impose a burden on affected people, their families, and employers, as well as a significant cost to society.
In spite of nearly a century of active investigation, Meniere’s disease remains an enigma. The etiology of hydrops is unknown, and its natural history is highly variable and unpredictable.2 Experience from morphological investigations 3 and animal experiments4 suggest that the symptoms in Meniere’s disease originate from a disturbance in the volume/pressure relationship of the endolymph. A distended scala media (i.e., hydrops) is the histologic hallmark of Meniere’s disease.5
Because specific curative therapy is not available, many treatment regimens have been used to reduce symptoms. Medical therapy (low-sodium diet, diuretics) is aimed toward decreasing the volume of the endolymph.6, 7 Although studies have been conducted to evaluate the efficacy of diuretic therapy, a restricted sodium diet has never been assessed using contemporary methods for clinical research. Vestibular suppressants are widely used for symptom suppression, but these have no effect on the underlying disorder. Vasodilators, herbs, acupuncture, and antiallergy therapy have all been employed as nonspecific measures. However, it has been postulated that therapeutic success in Meniere’s disease may reflect the natural history of the disorder more than the type of the pharmacological agent.2
The vertigo attacks typically occur episodically with symptom-free periods in between. For ~70% of patients the vertigo attacks gradually lessen in frequency and severity over several years. Many of these people demonstrate spontaneously reduced vestibular function in the affected ear, leading to the conclusion that vestibular burnout is the natural history of the disorder. Indeed, vestibular ablation therapy accelerates the time to reach this end point.
About 30% of patients have unrelenting attacks of vertigo in spite of medical therapy and may request surgical treatment. So many different types of procedures are included under this rubric it is little wonder that patients and physicians alike are uncertain about the best choice. Selecting from among these options is difficult because of the lack of scientific guidelines, the differences of opinions among physicians with similar backgrounds, and the absence of comparative studies.
This chapter (1) reviews the most important factors that influence therapeutic decision making for people with Meniere’s disease with life-disruptive vertigo, (2) reviews the evidence upon which to base a logical treatment rationale, and (3) briefly discusses the technique and consequences of these two minimallyinvasive procedures. The treatment approach for unilateral cochleovestibular Meniere’s disease described herein is that of the author and does not purport to be a consensus statement. Nonetheless it incorporates the existing evidence and, thus, has a rational basis.
■ General Elements to Consider in Treatment Decision Making
• Meniere’s disease is neither a uniform nor a predictable disorder. Therefore, there is no correct or curative treatment method. Patients may choose from an array of treatment methods.
• The treatment should fit the patient’s situation, age, general health, and ability to compensate for vestibular loss.
• An escalating treatment strategy, one that begins with the simplest measures, is a logical approach to treatment selection. Destructive procedures should not be used until nondestructive alternatives have been explored. The following levels of treatment illustrate this point.
Treatment Levels
Level 1: Diagnosis and medical therapy—reduced dietary sodium with or without diuretic, vestibular suppressants as needed
Level 2: Nondestructive therapy—Meniett Low-Pressure Pulse Generator (Medtronic Xomed, Inc., Minneapolis, Minnesota), endolymphatic sac surgery
Level 3: Vestibular ablation—chemical labyrin-thectomy, surgical labyrinthectomy, vestibular nerve section
Level 1
Diagnosis should be established by history, physical examination, audiometry, electrocochleography, and vestibular testing. Some providers use the term Meniere’s disease to refer to any disorder that causes vertigo. Delineation of the diagnosis is the first step in therapy.
Electrocochleography and glycerol testing are viewed by many as diagnostic of endolymphatic hydrops. Comparing the two tests, Mori et al8 found both were positive in 24% of 51 ears with a clear clinical diagnosis of Meniere’s disease, and either one was positive in 84%. Thus, although each test was abnormal in 50 to 60% of cases, the lack of congruence suggests that different pathophysiological aspects are being examined. These tests are often normal in the early stages of the disorder, they do not predict response to therapy, and they are not sufficiently sensitive or specific to be used as a diagnostic gold standard. Nonetheless, transtympanic or tympanic electrocochleography provides an objective correlate that lends support to the clinical impression.
Medical therapy begins with a review of the pathophysiology of the disorder, instructions on a 1500 mg sodium diet, a consideration of diuretic medication, and a discussion of lifestyle. Such consultations are lengthy and involved. Meniere’s patients typically have a long list of concerns that require detailed discussion.
Reassurance is vital. Patients need to understand that the majority of cases resolve over time, and that the vertigo spells can be stopped with ablative surgical therapy.
Level 2
Most patients achieve satisfactory control of their condition with the foregoing and simply require periodic case review for management. For those who deem their vertigo excessive, the next logical step is nondestructive therapy with either the Meniett device, which is described herein, or endolymphatic sac surgery, which is discussed in another chapter.
Level 3
Unilateral vestibular ablation (intratympanic gentami-cin, vestibular nerve section, or labyrinthectomy) has generally predictable and favorable results. All destructive procedures result in decreased vestibular function on the treated side, which most patients consider a fair exchange once central compensation has stabilized their balance. Further hearing loss is a risk with all three procedures, least with nerve section, and 100% with surgical labyrinthectomy.
■ Barotherapy Using the Meniett Device
Barotherapy for Meniere’s disease began with the common anecdotal observation that changes in ambient pressure (e.g., as with increasing altitude) improve Meniere’s symptoms.9 The first attempts at barotherapy were made when patients with acute symptoms were treated in a pressure chamber.10 Pressure chamber therapy has been used for acute attacks11, 12 but is cumbersome, expensive, and not widely available. Densert and colleagues13 demonstrated reduced symptoms and improved electrocochleographic findings in a randomized, blinded study using the Meniett device.
In 1999 the U.S. Food and Drug Administration cleared the Meniett device for sale in the United States as a Class II device under a 510k application. The Meniett low-pressure generator delivers pressure pulses within the range of 0 to 20 cm of H2O to the ear canal through a polyethylene tube with a close-fitting cuff. Each treatment sequence has three cycles, each consisting of 1 minute of pressure pulses and 40 seconds of pause, making each sequence last about 5 minutes. The frequency of the modulation is 6 Hz, and the duration of the pulse is 0.6 second (Fig. 14)
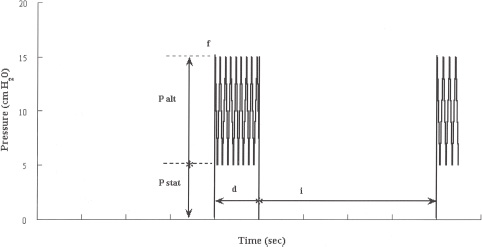
FIGURE 14-1 The details of the Meniett device’s pressure pulse are shown: amplitude of the alternating pressure component (P alt), amplitude of the static pressure component (P stat), frequency of the modulation (f), duration of the pulse (d), and interval between pulses (i). (Used with permission from Densert B, Densert O, Arlinger S, Sass K, Odkvist L. Immediate effects of middle ear pressure changes on the electrocochleographic recordings in patients with Meniere’s disease: a clinical placebo-controlled study. Am J Otol 1997; 18:726-733.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


