Fig. 14.1
Automated lamellar microkeratome 300 μm cut in a patient with granular dystrophy
A more recent modified technique of microkeratome-assisted LK consists of removing the anterior lamella from the host cornea and performing a partial trephination of the recipient bed with a 6.5 mm trephine. Then the Descemet’s membrane is exposed with a big bubble technique and donor tissue is sutured in place. The donor graft is cut about 100 μm thicker than the excised corneal lamella.
Technique: Donor Preparation for DSAEK and Ultrathin DSAEK
The following surgical technique is broadly described in Busin et al. [20, 21]. Central corneal thickness (CCT) is initially measured using ultrasound pachymetry. During the whole procedure, the ideal pressure in the artificial anterior chamber (AAC) is maintained by raising the infusion bottle at a height of 120 cm and clamping the tubing at about 50 cm from its entrance into the AAC. The first debulking cut is performed using a Carriazo-Barraquer (Moria, Antony, France) microkeratome with a 300 μm head. Pachymetry is then performed again to determine the residual tissue thickness. The second refinement cut is made with a 90, 110, or 130 μm microkeratome head, depending on the residual tissue thickness, with the goal of ultimately creating a graft that is approximately 100 μm or less (Fig. 14.2). For the second cut, the dovetail of the AAC is rotated by 180° in order to perform the second cut from a direction opposite to that of the first cut. In fact the depth of dissection is maximum at the beginning of the cut, and insisting with both cuts on the same spot would increase the risk of perforation and produce grafts of uneven thickness. Instead, the planar grafts obtained with this procedure are very thin but unlike DMEK grafts do not tend to roll onto themselves, thus allowing a relatively easy manipulation. The tissue is placed on a Barron punch with the endothelial side up and cut to the desired diameter (8.5–9.0 mm), and the stromal side can be marked to facilitate correct intraoperative orientation of the graft. A dedicated mini-glide is used to deliver the UT graft. The tissue roll obtained with UT grafts can pass easily through a small opening without being squeezed or damaged, and the mouth of the glide can be therefore inserted into a 3 mm wound to allow optimal tissue delivery.
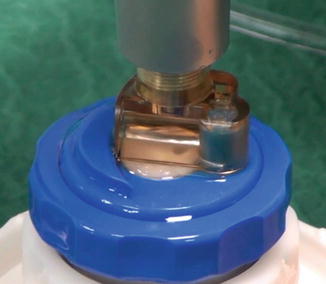
Fig. 14.2
Refinement cut during UT-DSAEK procedure
References
1.
2.
3.
4.
Krumeich JH. Indications, techniques, and complications of myopic keratomileusis. Int Ophthalmol Clin. 1983;23(3):75–92.CrossRefPubMed
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


