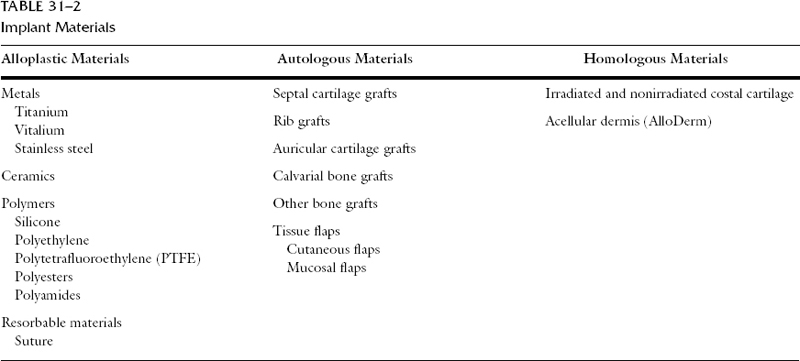
Functional and cosmetic rhinoplasty often mandates the need for implantable materials to change nasal contour or provide improved support for the nasal framework and overlying soft tissues. There are many implant materials, which can be divided into three main categories: autografts, homografts, and alloplasts. Autografts are those harvested from the patient and include, among others, cartilage, bone, dermis, fat, and fascia. Homografts, such as cartilage, bone, and dermis, are materials procured from donors of the same species. Alloplasts encompass a large group of synthetic and semisynthetic materials used as implants. A fourth group of materials, xenografts, are those implant materials harvested from other species, such as bovine collagen. The latter group is relatively small and therefore is not discussed further. Each category of graft maintains notable advantages and disadvantages, as outlined in Table 31-1. The controversy as to which material is superior is not a new one, and will continue to be debated until a group of alloplastic materials are developed that satisfy the basic needs of the ideal implant. A suitable implant must be biocompatible, strong, and elastic. The material should be completely inert, incapable of inducing inflammation or allergy, noncarcinogenic, resistant to mechanical strain, easily modified for shaping, and sterilizable. Surgical needs, patient selection, and the surgeon’s preference and experience are all factors that influence the choice of material for a given circumstance. Most would agree that auto-grafts should remain the primary choice for nasal reconstruction and rejuvenation. Situations do arise, however, in which harvesting a graft is impractical or increases the morbidity of a procedure in a patient with borderline medical status. Additionally, sufficient autogenous material may not exist to satisfy the surgical needs of the patient. For these situations, homo-graft materials are an adequate substitute to autografts. Graft location must also be considered when choosing an implant. Grafts for the relatively immobile dorsum may undergo less resorption than those placed in the nasal tip (Table 31-2).
| Alloplastic Materials | Autologous Materials | Homologous Materials |
| Metals | Septal cartilage grafts | Irradiated and nonirradiated costal cartilage |
| Titanium Vitalium | Rib grafts | Acellular dermis (AlloDerm) |
| Stainless steel | Auricular cartilage grafts | |
| Ceramics | Calvarial bone grafts | |
| Polymers | Other bone grafts | |
| Silicone Polyethylene | Tissue flaps | |
| Polytetrafluoroethylene (PTFE) | Cutaneous flaps | |
| Polyesters | Mucosal flaps | |
| Polyamides | ||
| Resorbable materials | ||
| Suture |
Autografts
Autologous tissue is the most favorable implant material. Bio-compatibility is unsurpassed, and the risk of infection and extrusion is far lower with autologous materials as compared with alloplasts.1 Cartilage to reconstruct the nose can be harvested from the septum, concha, or rib. Bone can also be taken from the septum, calvarium, or rib. Soft tissue can be brought into the area using various pedicle or free flaps as well as dermis and dermal-fat grafts. Autologous materials offer the obvious advantage of unsurpassed biocompatibility, but they do cause donor site morbidity and can resorb over time. Cartilage has the additional disadvantage of potential warping or deformity. The limited supply of cartilage from the septum and ear can also be problematic.
Septal cartilage is the graft of choice for nasal tip grafting.2–4 Septal cartilage is usually straighter and more rigid than conchal cartilage. It is easier to carve and shape because it is less fragile. Tardy et al.5 documented a multitude of successful septal cartilage grafts placed during rhinoplasty, with nearly two decades of follow-up. Septal cartilage is commonly used for struts, batten grafts, lateral crural grafts, lateral crural strut grafts, and spreader grafts. This cartilage is also an excellent material for shield tip grafts and buttress grafts adding projection or length and definition to the nasal tip. Dorsal augmentation can be performed using septal cartilage. Single or multiple layered grafts fixed with resorbable suture can be used for differing degrees of augmentation. A radix graft can be fashioned with bruised septal cartilage to improve the deep nasofrontal angle and to increase the acute nasolabial angle in the form of a plumping graft. Crushing cartilage may hasten the onset and severity of cartilage resorption.6 Septal cartilage is also our choice for strut grafting for tip support and for caudal septal grafting to increase the length and support of the nose.
Septal cartilage can be harvested through a variety of approaches. Regardless of the approach, the amount of cartilage to be removed should be dictated by the amount of cartilage required for grafting. In addition, at least 1.5 cm of dorsal and caudal septal cartilage should be preserved to achieve adequate support of the nose. The degree of cartilaginous hump removal should be contemplated before septum is harvested; if excess cartilage is removed, support may be compromised. The cartilage can then be carved and chamfered for precise contouring to match the surrounding tissue. The graft should be affixed in place with suture material.
Conchal cartilage is an alternative site to harvest an auto-graft and yields approximately 4 cm2 of cartilage, as well as perichondrium. Composite grafts including, skin, cartilage, and perichondrium can be used for nasal tip reconstruction, repair of alar retraction, and septal perforation repair (perichondrocutaneous grafts).7, 8 Free perichondrium can be used to camouflage a graft over the nasal tip in thin-skinned patients. Conchal cartilage is an adequate substitute for septal cartilage, grafts when the septum has been harvested previously. Owing to its more brittle nature, conchal cartilage can be more difficult to carve than septal cartilage. In addition, conchal cartilage is curved and less rigid than quadrangular cartilage. Like septal cartilage, conchal grafts can be used as a single-layered implant or sutured together to increase bulk. Conchal cartilage is appropriate for contour improvement of the nasal tip or as an onlay graft. However, septum or rib cartilage is stronger, and provides more support. Previous extensive auricular cartilage harvesting may preclude harvesting of further conchal cartilage. Other contraindications include systemic diseases, such as collagen vascular disease, rheumatic disease, or immunologic disorders involving the auricle, such as lupus, polychondritis, sarcoidosis, and Wegener’s granulomatosis. Careful preoperative analysis and questioning will guide the surgeon as to which ear should be used to harvest cartilage. Complete conchal cartilage removal may result in slight medialization of the pinna. Therefore, if asymmetric, the more prominent ear should be harvested. Furthermore, for the patient who has a history of sleeping on only one side of the head, the contralateral conchal cartilage should be harvested.
Several techniques for harvesting conchal cartilage have been described.9, 10 We prefer the posterior approach. The posterior approach avoids an incision on the anterior surface of the auricle and should be used when the postauricular region is to be exposed for other reasons (e.g., during otoplasty or rhytidectomy) or if the patient has a predilection for keloid formation. Conchal cartilage is considered the graft of choice for most non-structural grafting needs when septal cartilage is unavailable.
Saddle–nose deformities or severe structural deficiencies often require larger grafts, such as rib cartilage. Costal cartilage supplies sufficient amounts of cartilage for almost any structural defect of the nose. Confluent ribs five and six or seven and eight are the preferred ribs to harvest for nasal implantation. The disadvantages of using this graft include the potential for warping and resorption,11 potential pneumothorax, and postoperative pain.12 In older patients, cartilage calcification can make carving and shaping nearly impossible. Harvesting rib cartilage in the elderly should therefore be avoided. Carving techniques that attempt to remove equal proportions of cartilage from all surfaces of the rib have been associated with less warping.12 Despite careful technique unpredictable warping continues to be the primary problem associated with costal cartilage implantation. Costal cartilage should be used primarily as a strut graft for the nose lacking tip support or for dorsal augmentation in patients with saddle–nose deformity. Graft fixation may reduce the risk of malposition and warping.13 A boat–like configuration is the desired design for carving the graft to re–create the anatomy of the dorsum and allow for camouflage with adjacent nasal anatomy.14
Bone is a viable alternative to cartilage for dorsal nasal augmentation.15, 16 Split calvarium (membranous) is less likely to resorb than is iliac crest (endochondral).17, 18 In addition, calvarium can be harvested via the same operative field. The osteotomy required to harvest iliac crest is also associated with significant postoperative pain. For the above reasons, split calvarium is the graft of choice when bone is used for dorsal augmentation. The risks associated with harvesting calvarium include penetration of the cranial cavity, laceration of a major venous sinus, brain injury, and a postoperative depression of the skull.19, 20 Bone used in the nose can create a rigid–appearing structure. Although the graft is usually well tolerated and resorbs minimally, the unnatural nasal appearance and difficulty in shaping the graft make calvarial bone a less desirable implant. Fixation is necessary to maintain graft position and reduce the risk for resorption.21
Autologous materials are the implant of choice for many reconstructive surgeons. Situations do arise, however, when harvesting such tissue may be deleterious to the patient, or the tissue is not in a sufficient quantity to correct the given defect. Homografts are a viable alternative. Alloplastic materials have also been used with varying success to augment the nose and serve as an additional, less acceptable, alternative to autografts.
Homologous Grafts
Homologous bone, cartilage, and dermal grafts alleviate donor site morbidity, but significant resorption has been reported. Toriumi et al.22 studied long–term resorption rates of demineralized bone split rib implants. The average rate of resorption after only 2 years was greater than 80%. The results obtained with homologous tissue can also be unpredictable. The surface structure of the implant material can change with time, leading to distortion of the overlying soft tissue. Despite these potential inadequacies, irradiated cadaveric costal cartilage serves as an adequate substitute for autologous rib cartilage. A number of things can be done to attempt to decrease the risk of warping and distortion. Gunter et al.13 describe the use of K–wire insertion into grafted cartilage to prevent such changes with time. Shaving equal amounts of cartilage from all surfaces of the graft may reduce the risk of graft distortion and warping. All perichondrium should be removed to further reduce the potential for cartilage distortion. Irradiated costal cartilage grafts have been used by several surgeons for dorsal nasal augmentation with success.23–25 Use of this material should be limited to the dorsum. Implantation into the mobile nasal tip has been associated with significant resorption.26
Cadaveric rib cartilage is obtained from donors who must meet the same criteria required for organ donation, such as screening for VDRL, hepatitis B, human immunodeficiency virus (HIV), tuberculosis, and slow virus testing. The selected donor rib is then exposed to 60,000 Gy g –waves to destroy cellular and viral pathogens. These grafts are well tolerated because their relative acellular makeup illicits minimal immune response by the host.1
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


