An unstable canal wall-down mastoidectomy cavity has the potential to impart a major negative impact on a patient’s quality of life due to the collective burden of chronic otorrhea, frequent office visits, expensive pharmacotherapy, and occasional discomfort.1,2,3,4 In the pediatric population, where tolerance of office examination and aural toilet may be poor, this is a particular dilemma.5 Even in the best cases, a cavity that is stable from a chronic infection standpoint can still require occasional cleaning, cause caloric-effect vertigo, and inhibit optimal hearing aid fitting. Given this reality, mastoid obliteration offers many advantages and the potential to eliminate some of the undesirable aspects of the canal wall-down scenario.6,7,8,9,10,11
A review of the literature portrays a rate of mastoid cavity instability that roughly ranges from 10% to 60%, with apparent heavy dependence on the skill of the surgeon in executing a sound canal wall–down mastoidectomy technique, such as what is detailed in Chapter 35.2,3,4,6,12 Even if a particular surgeon is averse to performing primary canal wall-down mastoid surgery, encountering and at times revising such cavities is an inevitable part of an otologic practice. Thus, familiarity with canal wall–down mastoidectomy and mastoid obliteration techniques should be viewed as a valuable tool within an otologic surgeon’s skill set.
41.2 Patient Selection
Candidates for mastoid obliteration include both adults and children undergoing either primary or revision canal wall-down mastoidectomy surgery. The general obliterative scheme utilized and extent of obliteration will vary depending on factors such as the nature of the underlying cholesteatoma, temporal bone pneumatization, and degree of infection. In general, obliterative techniques are frowned upon in areas deemed at high risk of cholesteatoma recurrence; however, such risk often does not particularly apply to the mastoid because cholesteatoma within the mastoid is rarely difficult to expose and definitively remove. This point is highlighted by the fact that recurrent cholesteatoma within the mastoid cavity during second-stage canal wall-up surgery is rare.13
If temporal bone pneumatization is limited, it is quite common to achieve a small self-cleaning cavity without the need for mastoid obliteration. However, combined mastoid and epitympanic obliteration in these cases may still be deemed advantageous as a means of repositioning the height of the tympanic membrane at the level of the native tympanic ring, thereby preserving normal middle ear volume and facilitating a successful ossiculoplasty. When infection is severe or factors are present that negatively impact healing, such as diabetes, radiation, immunosuppression, or tobacco use, mastoid obliteration is particularly advantageous given that patients with these conditions may be at high risk of developing an unstable cavity.1
41.3 Surgical Technique
41.3.1 Obliteration Schemes
The first step made by the surgeon is deciding which areas to obliterate. In the typical situation where the mastoid is deemed to be at low cholesteatoma risk, the mastoid is obliterated with application of filler and a liner in sequence. When doing so, the purpose of the filler is not only to eliminate cavity volume, but also, more importantly, to fill cavity irregularities and to provide a smoothly contoured platform upon which to apply a liner that will subsequently epithelialize.
If epitympanic cholesteatoma risk is also deemed low, the obliteration scheme can be expanded to include the epitympanum to re-create the natural annulus height. In the uncommon situation where the mastoid cavity is felt to be at high risk, such as infiltrative cholesteatosis involving the perilabyrinthine air cells, the obliterative scheme is limited by sparing part of the mastoid cavity or by applying only a thin liner alone without the use of fillers.
The technique of canal wall-down mastoidectomy may slightly differ in a pneumatized versus a sclerotic temporal bone, which may also impact the approach taken toward obliteration. In a pneumatized bone, the general scheme often will involve lowering the edges of the cavity via wide saucerization and amputation of the mastoid tip, which results in a broadened shallow cavity that will invite inward soft tissue collapse. Obliteration of these large cavities is often best approached with sensible application of filler materials followed by lining with vascularized soft tissue flaps.
In contrast, a sclerotic temporal bone that is also deemed amenable for epitympanic obliteration may be reconstructed with simpler techniques given that these cases may involve comparatively less drilling of canal wall and solid mastoid bone once the cholesteatoma and a limited number of diseased air cells have been eliminated. Mastoid obliteration in a sclerotic temporal bone thus may be completed with a much smaller volume of filler and simple application of a liner and any preserved native canal wall epithelium.
41.3.2 Obliteration Materials
Choosing obliteration materials is often dependent upon a surgeon’s bias and background as well as the nature of the underlying tympanomastoid defect. If the defect is small, the choice of obliteration materials tends to be more forgiving.
Bone Paté
Bone paté is a commonly used filler material, but it must be covered by a liner to prevent extrusion. Bone paté is abundantly available, in particular from the squamous temporal bone deep to the temporalis muscle. Harvest of bone paté is undertaken by reflecting the temporalis and drilling cortical bone with a cutting bur, followed by collection either using a commercially available reservoir connected to the suction tubing, or, if plentiful, by simply scooping paté from the surgical field into a specimen cup. It is crucial that paté only be harvested from outside of the mastoid so as not to include mucosa or infected material.
After harvest, bone paté is soaked in antibiotic solution while the remaining portions of surgery are completed. For placement, it is essential that the paté is applied into the defect and then densely packed utilizing a suction cannula and cotton pledget (▶ Fig. 41.1). In doing so, it is typical to sequentially apply paté several times in one site to achieve the desired tightly packed density. If bone paté is not densely packed, there is a tendency toward excessive reabsorption that can result in eventual formation of “potholes” within the obliterated cavity.
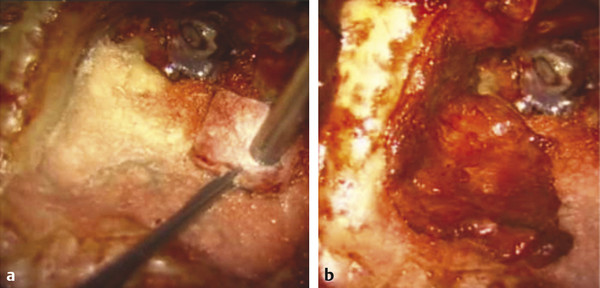
Fig. 41.1 Application of bone paté. (a) Bone paté harvested from the outside of the mastoid cavity is densely packed with a suction cannula and cotton pledget, with multiple applications to fill cavity irregularities (left ear), reduce cavity volume, and generate a smoothly countered platform upon which to apply a soft tissue liner. (b) In this case the middle temporal artery flap was utilized as a liner.
Cartilage Chips
Auricular cartilage chips are harvested either from the tragus or concha. Once large pieces of cartilage have been acquired from these sites, they are stripped of perichondrium and morselized with a scalpel blade. If there is concern for infection, cartilage chips may be soaked in antibiotic solution, similar to soaking bone paté. After application into the mastoid cavity, a liner is typically applied to prevent extrusion (▶ Fig. 41.2).

Fig. 41.2 Application of cartilage chips. Cartilage chips are harvested from the tragus and/or concha and morselized with a scalpel blade. Cartilage chips are favored for their high surface area and strong resistance to infection or extrusion.
Compared with bone paté, cartilage is more resistant to reabsorption and infection and, therefore, it is the authors’ filler of choice. The larger size of the cartilage chips results in greater surface area and less need for dense packing. However, in some instances, availability of a sufficient quantity of cartilage may be problematic, especially in a well-pneumatized temporal bone or if cartilage has been used extensively for tympanic membrane reconstruction. In these cases it is possible to combine the cartilage with bone paté or synthetic filler.
Synthetic Materials
Various synthetic materials have been described as fillers in mastoid obliteration, particularly biocompatible ceramics. As noted in Chapter 8, if use of a synthetic material is desired, porous ceramics in a granular form are favored over cements because the latter seem to bear a higher risk of infection. Also, if an extraordinarily large bone defect requires obliteration, osseo-inductive materials, such as bioactive glass (BoneAlive, Boston Medical Products Inc., Westborough, Massachusetts), which are gradually replaced by new bone, may have theoretic advantages. Commercially available xenograft materials, such as demineralized bone matrix (DBX, Osteotech, Inc., Eatontown, New Jersey), are also an option and have been used successfully in small quantities (<2 ml) by the authors for several years.14
Although synthetic materials offer the advantage of being readily available in bulk, they generally share a common tendency to extrude or to become infected. As such, it is favorable to use synthetic materials judiciously and/or in limited combination with autologous materials. Often, it is possible to obliterate the areas deep within the mastoid cavity, such as the sinodural angle and opened retrofacial air cell tract, using synthetic materials, and then to cover these with a layer of cartilage or bone paté that will constitute the outer interface (▶ Fig. 41.3). If it is deemed necessary to use synthetic fillers in larger quantities, lining with a vascularized soft tissue flap is recommended.
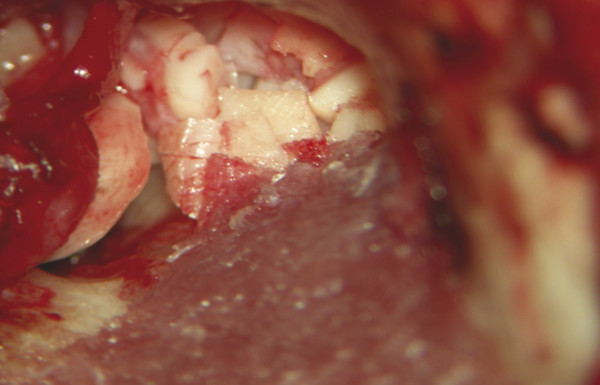
Fig. 41.3 Obliteration with demineralized bone matrix and cartilage chips. Demineralized bone matrix is applied to fill the sinodural angle (left ear), and cartilage chips are then used for obliteration of the more superficial areas near the reconstructed tympanic membrane. Synthetic materials may be useful when additional bulk is required to fill a mastoid cavity.
Fascia, Perichondrium, and Pressed Muscle
Thin autologous connective tissues, such as temporalis fascia, pressed skeletal muscle, and auricular perichondrium, can all be used as liners. Such tissue is readily available and easy to process. When very little filler material is required, when there is a large quantity of intact healthy native canal wall epithelium, and/or when the interface with filler materials is small, such as with a sclerotic mastoid defect, these materials generally work well (▶ Fig. 41.4). However, if extensive coverage of filler material is necessary, particularly if the filler is synthetic, non-vascularized grafts may undergo necrosis, infection, and/or delayed epithelialization.
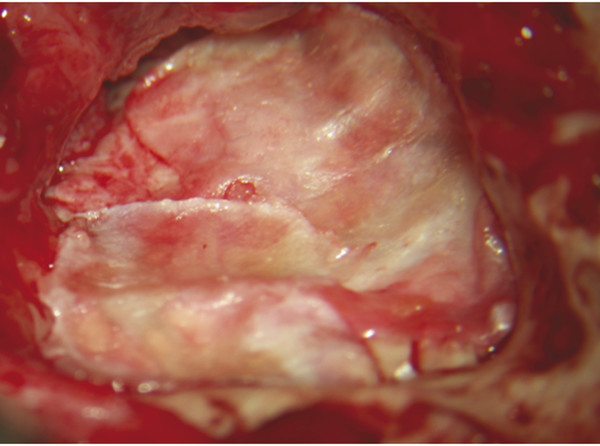
Fig. 41.4 Obliteration with demineralized bone matrix and cartilage chips. Demineralized bone matrix is applied to fill the sinodural angle (left ear), and cartilage chips are then used for obliteration of the more superficial areas near the reconstructed tympanic membrane. Synthetic materials may be useful when additional bulk is required to fill a mastoid cavity.
Soft Tissue Flaps
Rotational soft tissue flaps may variably comprise fascia, periosteum, and/or muscle, having either a distinct or random blood supply. These are pedicled either from a posterior-inferior base or superior-anterior base. In the case of the superior-anterior–based group, thick muscular flaps, such as those composed of temporalis muscle, are best avoided due to the potential for this thick pedicle to obstruct or narrow the external auditory meatus as it enters the tympanomastoid compartment.
Vascular supply to most rotational flaps described for mastoid obliteration is random or variably robust. For example, the commonly used Palva flap does not have a distinct vascular supply and, therefore, it is prone toward shrinkage and less apt to resist infection (▶ Fig. 41.5). Most posterior-inferior-based flaps are randomly fed by branches of the posterior auricular or occipital arteries proximally but tend to be avascular like the Palva flap at the most superior (distal) aspect.
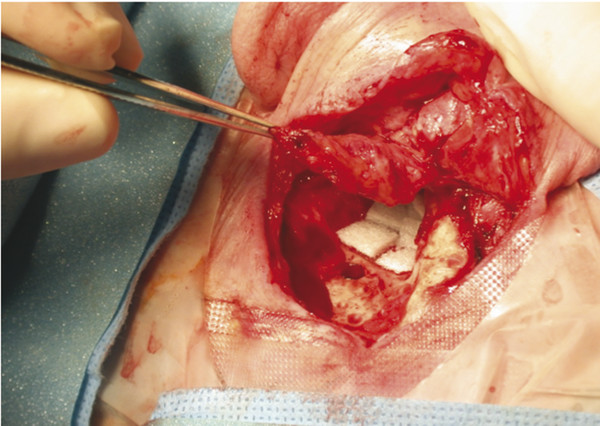
Fig. 41.5 Palva flap. A Palva flap consists of muscle, fascia, and periosteum that is hinged on the posterior aspect of the pinna (left ear). Although useful in some cases as a source of soft tissue obliteration, it lacks a robust vascular supply and therefore may be prone toward delayed shrinkage and fibrosis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


