FIGURE 8.1 Design of a right latissimus dorsi musculocutaneous flap for total glossectomy reconstruction. The skin paddle is oriented perpendicular to the axis of the muscle fibers.
Anterolateral Thigh Free Flap
The perforator-based ALT free flap emerged as an option for skin and soft tissue reconstruction after Song et al. described it in 1984. The use of the ALT flap for reconstruction of defects in the head and neck was first reported by Koshima et al. in a cohort of 22 patients. It gained widespread popularity for application in the Asian population, and Wei et al. have described outcomes for 475 patients, the largest series for head and neck reconstruction with the ALT available to date. The reduced application of the ALT flap in the Western population is attributed to a higher incidence of obesity, which causes excess thickness of adipose tissue in the thigh. Furthermore, variability in the vascular anatomy predisposes to difficult dissection. However, experience and expertise acquired by the microvascular surgeons to harvest and thin the flap have rekindled the interest in the application of the ALT flap for reconstruction in the head and neck in many centers.
HISTORY
Evaluation of medical comorbidities is an important component of preoperative history for free tissue transfers since these procedures subject the patient to prolonged anesthesia and fluid imbalance. Hematologic or hepatorenal abnormalities merit a thorough preoperative investigation and correction since these may affect the intraoperative blood loss, postoperative hematoma formation, and thus, the viability of flap. Conditions such as diabetes and active smoking cause small vessel obliteration and are known risk factors for microvascular complications, and necessary measures should be taken to avoid any compromise of the microvascular anastomosis. Preoperative correction of nutritional deficits helps optimize the healing process. Cigarette smoking, administration of more than 7 L crystalloids (approximately 6 mL/kg/h), and weight loss of over 10% prior to surgery have been found to be significant for the overall flap complication rate in our analysis of cases with free tissue transfer.
PHYSICAL EXAMINATION
Assessment of the general body habitus and performance status of the patient is important for any free flap reconstruction to design a plan for harvest, donor site closure, and functional preservation. Furthermore, a complete examination of the head and neck by the microvascular surgeon with prediction of the probable surgical defect following total glossectomy, and careful examination of the donor site are critical in decision-making. Previous traumatic or surgical scars in the head and neck, skin cancer and radiation damage are important considerations in planning the placement of incisions for resection and protection of suitable recipient vessels. Examination of skin and soft tissue bulk, presence of scar, and presence or absence of arterial pulses (axillary, femoral) also influence selection of the donor site. For example, a large, previous thoracotomy incision may have traversed the latissimus dorsi muscle.
INDICATIONS
The latissimus dorsi flap provides suitable bulk and volume for true total glossectomy defects that include the entire base of tongue and oral tongue in the resection. It is also an ideal mode of reconstruction where there is an anticipated need for motor innervation. The ALT flap is more suitable for reconstruction of total oral glossectomy defects and is the flap of choice when a sensate reconstruction is planned. It is also a more conveniently accessed donor site.
CONTRAINDICATIONS
Latissimus Dorsi Flap
Congenital absence of latissimus muscle associated with Poland anomaly or other familial defects of the shoulder girdle is an absolute contraindication. Patients with a scar on their back or with a preexisting disability of the back or shoulder girdle do not make ideal candidates for reconstruction with the latissimus dorsi flap. It is also relatively contraindicated in patients with a history of previous surgery in the axilla due to the risk of possible disruption of the proximal vascular supply to the muscle.
Anterolateral Thigh Flap
Absence of musculofasciocutaneous perforators from the descending branch to the skin paddle is an absolute contraindication to this flap (see below, Pitfalls). Previous injury or surgery of the upper thigh such as vascular bypass procedures are relative contraindications for reconstruction with the ALT flap. Also, atherosclerotic superficial femoral arterial occlusion may result in substantial collateral flow through the profunda femoris and its branches to the distal lower limb. If such a situation pertains, the patient should be evaluated by a vascular surgeon before proceeding to harvest an ALT flap. The presence of a thick saddle bag of adipose tissue in the thigh makes such patients less than ideal candidates for ALT reconstruction because of the excess tissue bulk transferred to the recipient site.
PREOPERATIVE PLANNING
Fundamental to preoperative planning is a thorough knowledge of the anatomy of the donor site, which is critical to the flap harvest and reconstructive technique. Pertinent anatomic details of the latissimus dorsi and ALT flaps are discussed below.
Anatomy of the Latissimus Dorsi Free Flap
The latissimus dorsi muscle originates from the spinous processes of the lower six thoracic vertebrae, posterior iliac crest, the thoracolumbar fascia, last four ribs, and inferior angle of scapula. It inserts at the medial aspect of the intertubercular groove of the humerus. The dominant blood supply of the flap arises from the thoracodorsal artery, which is one of the two branches of the subscapular artery. The latter is the largest branch of the axillary artery and originates from its third part, gives rise to the circumflex scapular artery before continuing as thoracodorsal artery. The thoracodorsal artery enters the upper border of the latissimus dorsi and divides within the muscle into superior and lateral branches. It also gives a branch to the serratus anterior muscle that needs to be ligated during flap harvest. In its inferior half, the muscle receives perforators from the thoracic intercostal and lumbar arteries. The overlying skin is nourished by multiple musculocutaneous perforators that are more abundant over the upper two-thirds of the muscle, making it the preferred site for harvest of the skin paddle.
Venous drainage of the muscle is via the venae comitantes that accompany the thoracodorsal artery during their course along the undersurface of the latissimus dorsi muscle, draining to the axillary vein. The artery may vary in diameter from 1 to 4 mm, and the diameter of the vein may range from 2.5 to 4.5 mm. The motor innervation to the latissimus dorsi is provided by the thoracodorsal nerve (middle subscapular nerve), derived from the posterior cord of the brachial plexus (C6, C7, and C8). The nerve travels distally with the vascular pedicle, but closer to the vein.
Anatomy of the Anterolateral Thigh Flap
For reconstruction following a total glossectomy, the ALT flap is usually harvested as either a perforator-based myocutaneous flap including portions of vastus lateralis muscle or a fasciocutaneous flap (Fig. 8.2).
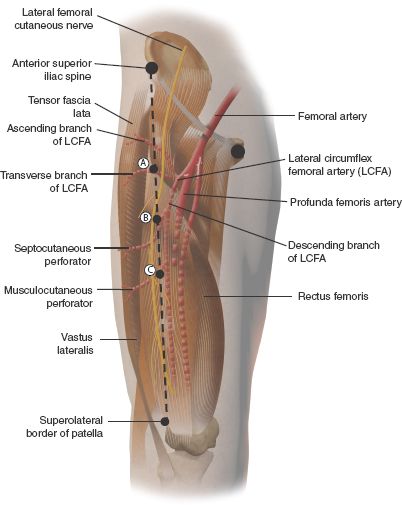
FIGURE 8.2 Anatomy of a right ALT flap. Black line represents the intermuscular septum between rectus femoris and vastus lateralis. A, B, and C represent the likely location for proximal, middle (most common), and distal perforators, typically separated by 5 cm. LCFA, lateral circumflex femoral artery.
Fascial and Muscular Anatomy
The superficial fascia of the thigh forms a continuous layer over the thigh and consists of areolar tissue. It may be separated into two or more layers, between which are found the superficial vessels and nerves. The deep fascia of the thigh, the fascia lata, varies in thickness in different parts, being thicker in the superior and lateral aspect of the thigh. The muscles encountered during ALT flap harvest include the rectus femoris, vastus lateralis, and the tensor fascia lata. The rectus femoris arises from two tendons: one from the anterior inferior iliac spine and the other from the acetabulum. It occupies the middle of the front of the thigh and ends into a flattened tendon that inserts into the superior patella. The vastus lateralis is the largest part of the quadriceps femoris. It arises by a broad aponeurosis attached mainly to the superior part of the intertrochanteric line and to the anterior and inferior borders of the greater trochanter. The fibers run inferiorly over the lateral side of the thigh and thicken into a flat tendon for insertion into the lateral border of the patella. The tensor fascia lata occupies the lateral border of the thigh. It arises from the posterior part of the iliac crest, anterior superior iliac spine, and the deep surface of the fascia lata and gets inserted between the two layers of the fascia lata close to the junction of the middle and upper thirds of the thigh.
Vascular Anatomy
The ALT flap is based on the perforating vessels arising from the descending branch of the lateral circumflex femoral artery (LCFA). The LCFA is a branch of the profunda femoris artery and divides into ascending, descending, and transverse branches. The descending branch of LCFA is usually associated with two venae comitantes. It travels obliquely and inferiorly in the intermuscular groove between the rectus femoris and vastus lateralis along with the nerve to the vastus lateralis and terminates in the vastus lateralis just above the knee. The descending branch provides several perforators to the skin of the lateral thigh. These vessels pass in either a septocutaneous or myocutaneous pattern. The septocutaneous perforators run between the rectus femoris and vastus lateralis muscles and traverse the fascia lata to supply the skin of the lateral thigh as septocutaneous perforators. Alternatively, the perforators can traverse the vastus lateralis muscle tissue and the deep fascia and supply the skin as musculocutaneous perforators.
Septocutaneous perforators are highly inconsistent in their number and origin. The proportion of septocutaneous (vs. musculocutaneous perforators) varies from 10% to 60% across different clinical and cadaveric studies. By contrast, musculocutaneous perforators are more constant, present in 50% to 90% of cases. This variation in vascular anatomy is important to know since elevation of the ALT flap requires meticulous intra-muscular dissection for preservation of musculocutaneous perforators.
The average diameters of the vascular pedicle are reported to be 2.1 mm for the artery and 2.6 mm for the vein. These measurements may, however, range from 1.5 to 4 mm and from 1.5 to 5.0 mm, respectively, for the artery and the vein.
Classification of the Perforators
The perforators have been classified by Yu et al. for better identification during flap harvest.
1. Classification Based on the Pattern of Location: The cutaneous perforators are usually concentrated within a radius of about 3 cm around the midpoint of the line between the anterior superior iliac spine and superolateral patella. However, more perforators have been discovered that are spread over a larger part of the ALT flap. These are usually present in predictable locations about 5 cm apart and have been named as perforators A (most proximal), B (middle), and C (most distal); Perforators B are present most consistently.
2. Classification Based on the Origin: The cutaneous perforators have been classified as types I, II, and III based on their origin from the parent artery.
Type I: This is the most common type in which perforators originate from the descending branch of the lateral circumflex femoris artery and travel as septocutaneous or musculocutaneous perforators.
Type II: A single cutaneous perforator derives from the transverse branch of the lateral circumflex femoris artery and travels longitudinally within the vastus lateralis muscle for its entire length before it enters the fasciocutaneous flap.
Type III: A single perforator derives directly from the profunda femoris artery and pierces through the rectus femoris muscle to reach the fasciocutaneous flap.
Sensory Innervation
The lateral femoral cutaneous nerve is the dominant sensory nerve of the ALT. It is a direct branch of the lumbar plexus (L2, L3) and enters the thigh deep to the lateral aspect of the inguinal ligament near the anterior superior iliac spine. It consistently runs along the line connecting the anterior superior iliac spine and the superolateral patella in the deep subcutaneous tissue immediately above the fascia.
Nerve to the Vastus Lateralis Muscle
The nerve innervating the vastus lateralis muscle is intimately related to the descending branch of the lateral circumflex artery. Two particular variations of the anatomy of the nerve make it susceptible to interruption during harvesting of the ALT flap, thus increasing the risk of denervation of the muscle: One where the motor nerve courses through the vascular pedicle or another where it travels between the perforators supplying the flap. The frequency of the presence of at least one of these unfavorable variations had been reported to be 28% in one of the anatomical studies. However, denervation of the vastus lateralis appears to cause little or no functional loss.
Assessment of Recipient Vessel Availability
Evaluation of the history of previous treatment and physical examination of the entire head and neck will alert the reconstructive surgeon, especially in the setting of previous radiotherapy or neck dissection, to vessel abnormalities. Doppler ultrasonography or angiography in patients with known vessel depletion or carotid artery disease may be required to assess the adequacy of the external carotid artery and its branches for selection of an appropriate recipient vessel for microvascular anastomosis.
SURGICAL TECHNIQUE
Latissimus Dorsi Free Flap
Flap Design
The unique features of my latissimus dorsi flap design include transverse orientation of the skin paddle, demarcation of the skin paddle into two portions—one anterior and another posterior—incorporation of two lateral skin and muscle “wings” (Fig. 8.3), and incorporation of the motor nerve to the latissimus dorsi muscle.
FIGURE 8.3 Right latissimus dorsi free flap harvest. Two silk marker sutures placed on the sides of the muscle component to reference the in situ length–tension relationship.
The flap is fashioned in a way so that the musculature forms a transverse sling or “hammock” across the floor of the mouth, and the skin is sufficiently redundant so as to be sculpted vertically at the front of the mouth for articulation. The longitudinal dimensions of the flap allow adequate curvature and suspension of the midportion of the skin and muscle component at the isthmus of the oropharynx. This design facilitates creation of oral and pharyngeal portions of the skin paddle that partially simulate oral tongue and the base of tongue, respectively, in structure and function.
Flap Harvest
Harvesting of the latissimus dorsi flap requires a lateral decubitus and a 45-degree shoulder and trunk up position. By rotating the table toward the donor site, resection is facilitated and by rotating the table away from the donor site, harvest is facilitated. This avoids repositioning the patient during the procedure.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


