FIGURE 2.1 Using a tongue blade on the thigh to maintain constant pressure, the dermatome is then applied at a 30- to 45-degree angle and activated.
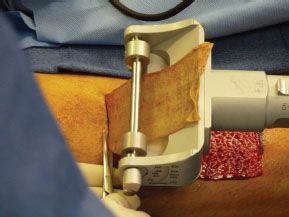
FIGURE 2.2 When the appropriate size of the skin graft is achieved, the dermatome is tilted away from the skin and the base of the graft is separated from the donor site using either a scalpel or scissors.
Before suturing the graft into the FOM defect, the graft is “pie-crusted” to allow for egress of any possible fluid accumulation. This is achieved by making small longitudinal incisions with a no. 15 blade. A nasogastric tube is inserted prior to suturing the graft into the defect.
The graft is sutured into the defect using 3-0 Vicryl sutures. A Xeroform gauze bolster is placed over the graft and sutured into place. 2-0 silk sutures are tied over the bolster to immobilize the graft. If there is significant edema of the FOM or retropulsion of the tongue, a tracheostomy should be considered.
Donor-site hemostasis is achieved by placing 1:100,000 epinephrine–soaked gauze. Once hemostasis is achieved, a Tegaderm is placed.
POSTOPERATIVE MANAGEMENT
Postoperatively, the patient receives his or her nutrition through a nasogastric tube. The bolster is left in place for 7 days. Revascularization of the graft usually begins after 2 to 3 days with full circulation achieved by 6 to 7 days.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


