FIGURE 13.1 External markings on the left check for a pectoralis flap harvest.
First, the incision is made on the lateral aspect of the proposed skin paddle. The lateral border of the pectoralis major muscle is identified, which allows me to refashion the skin paddle if a significant portion is not overlying the pectoralis muscle. Once the muscle is identified, the avascular plane between the pectoralis major and the pectoralis minor muscle is bluntly dissected. This allows identification of the descending pectoral branch of the thoracoacromial artery (Fig. 13.2). Two vascular pedicles are often identified. For mobilization purposes, the lateral pedicle can be sacrificed safely. Once the pedicle is identified, the medial skin incision is made at the level of the midline of the chest and carried down to the level of the pectoralis major muscle.
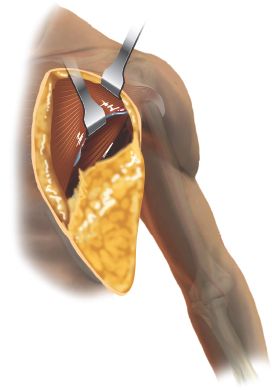
FIGURE 13.2 Pectoralis flap harvest. Vascular pedicle identified between pectoralis major and pectoralis minor muscles (arrow).
The skin paddle is tacked to the underlying pectoralis major muscles using 3-0 Vicryl sutures to avoid shearing during elevation of the flap. The pectoralis major muscle is then dissected off of the chest wall using electrocautery. Intercostal perforators must be carefully ligated or cauterized.
The medial attachments to the sternum are then transected to the level of the clavicle. Care must be taken to stay lateral to the internal mammary perforators in the second and third intercostal spaces. In a similar fashion laterally, the muscular attachments to the humeral head are divided up to the level of the clavicle, being careful not injure the cephalic vein.
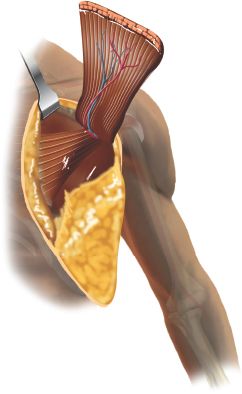
The nerve of the pectoralis major muscle is identified intimately associated with the vascular pedicle. Prior to its transection, the pectoral nerve can be confirmed by stimulation. In my experience, it is important to divide this nerve to avoid constriction of the venous pedicle especially if the muscular portion of the flap needs to be rotated for reconstruction. The flap is then completely harvested, keeping the vascular pedicle in view (Fig. 13.3).
A tunnel is created in a subcutaneous plane approximately four finger breadths in size to allow rotation of the flap into the neck without constriction of the blood supply to the flap. The flap is then brought through this tunnel into the oral cavity defect.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


