Management of Soft Tissue Injuries of the Face
Scott Shadfar
William W. Shockley
Soft tissue injuries involving the face, head, and neck are becoming more frequent, and the experienced otolaryngologist is commonly the designated surgeon chosen to make a timely assessment and repair. The management of facial soft tissue injuries present challenges both from a functional and aesthetic perspective. Injuries to the face can affect speech, vision, alimentation, and facial expression. The resulting facial scars and deformities also can be associated with a host of psychosocial issues. This chapter is devoted to the initial evaluation, classification, and early management of facial wounds. We also provide specific anatomical considerations for different anatomic sites with respect to facial soft tissue injury management and care.
ETIOLOGY AND MECHANISM OF INJURY
The leading causes of facial soft tissue injuries are assault, motor vehicle accidents, work-related injuries, sport injuries, animal and human bites, as well as burns. In addition, there has been a surge in the literature highlighting injuries encountered from the battlefield (1). Details into whether protective measures were in place, such as helmets, seat belts, or air bags, can guide the evaluation. Injuries sustained despite these measures calls one’s attention to the force behind the injury and need for further workup.
EVALUATION
Patients with serious or life-threatening injuries are first assessed in the emergency room, or trauma bay when available. Advanced Trauma Life Support guidelines are followed where airway, breathing, circulation, disability, and exposure (ABCDE) take precedence. In the critically ill patient, stabilization will proceed in a standard fashion with the insertion of two large-bore intravenous lines. Acute hemorrhage from the head and neck region is addressed at this time. An airway is established if deemed necessary. Any oral or pharyngeal hemorrhage leading to inability to protect the airway calls for airway intervention, all while maintaining cervical spine precautions. In this setting, 3% to 10% of facial injuries with fractures have concomitant c-spine injuries (2,3). Although facial injuries can bleed profusely, they can distract health care providers from other more immediately threatening injuries. Often a moist gauze and pressure dressing can be applied to facial wounds if other injuries, such as chest or abdominal trauma, necessitate urgent treatment.
A thorough history, if obtainable, is necessary when a patient presents with a traumatic injury. Knowledge of the patient’s underlying comorbidities and past medical history is especially important in those patients with compromised host defenses as in patients with diabetes, immunosuppression, chronic corticosteroid use, malnutrition, and obesity.
Allergies to medications including local anesthetics, general anesthetics, and antibiotics should be documented. Social history regarding smoking, ethanol, and illicit drug use should also be obtained. In most cases of major trauma, serum alcohol levels and a drug screen should be checked as the presence of cocaine or amphetamines may delay elective operative intervention; these interactions with general anesthesia are known to increase cardiac risks. Tetanus history should also be noted at this time, with appropriate treatment based on the patient’s history (see section on “Tetanus”).
A complete head and neck examination should be performed with final attention focused on the injured site. A detailed description of the wound in terms of wound classification, location, depth, length, and condition of wound edges should all be assessed and documented. Cranial nerve examination is performed to identify any
deficits. Next, evaluate for deep tissue injury (clear fluids leaking indicative of cerebral spinal fluid [CSF], salivary, or lacrimal injury) (4) as well as presence of fractures or foreign bodies (gravel, wood, broken or loose teeth). When possible, photo documentation should be performed for medical and legal reasons.
deficits. Next, evaluate for deep tissue injury (clear fluids leaking indicative of cerebral spinal fluid [CSF], salivary, or lacrimal injury) (4) as well as presence of fractures or foreign bodies (gravel, wood, broken or loose teeth). When possible, photo documentation should be performed for medical and legal reasons.
Prior to extensive examination and wound preparation, appropriate anesthesia and analgesia should be provided for patient comfort. The authors seldom use sedation, outside of the pediatric population. Imaging studies pertinent to the head and neck region including plain films and computed tomographic (CT) studies should be obtained when there is concern for facial fractures, missing teeth, or foreign bodies. Noncontrast high-resolution CT imaging is the preferred imaging modality to evaluate facial fractures, while contrasted CT angiography is indicated for identification and delineation of a vascular injury as seen in penetrating neck injuries (see Penetrating Head and Neck Injury chapter). Once the patient has been stabilized, the involved physicians should prioritize further workup, management, and surgical repairs. Depending on the nature of the injuries, appropriate consultations should be obtained.
WOUND CLASSIFICATION Abrasions
Classifying wounds on assessment aids in sorting and developing a treatment algorithm. Wounds are most commonly classified by depth, which is influenced by the mechanism. When the epidermis and partial thickness dermis has been lost, secondary to scraping the skin, this is classified as an abrasion. For these injuries, the critical steps in management include irrigation and cleansing with meticulous removal of any embedded dirt and debris. Once the wound is fully clean, topical ointment is sufficient treatment. The patient is instructed to keep the wound clean and dressed. In most circumstances, a topical antibiotic ointment is both practical and effective. Maintaining a moist environment without crusting helps promote faster reepithelialization from the remaining undisturbed skin appendages. Avoidance of direct sun exposure is recommended as this can cause skin pigmentation at the site of injury, which is most often temporary. Sun avoidance and protection should be mandatory for a minimum of 6 months.
Contusions/Hematomas
Contusions are usually from blunt force trauma without breech of the overlying skin. Disruption of the small capillaries and vessels leads to swelling and ecchymosis. These changes usually resolve over time without intervention. Expectant management is usually sufficient with head elevation and ice packs. Soft tissue hematomas result in marked swelling and can sometimes organize into a localized hematoma. In most cases, all that is needed is supportive care and observation, assuming there are no functional or airway issues. Needle aspiration can be undertaken after liquefaction of the clot, usually around 10 days post injury. If hematomas occur in the tongue, floor of mouth, or neck one must consider the potential for airway compromise. In addition, underlying vascular injuries may be suspected.
Avulsion Injuries
Avulsion injuries result from the shearing or tearing of tissues. This leads to full-thickness cutaneous injury sometimes associated with loss of the involved tissue segment. Avulsion injuries may be associated with subcutaneous, cartilaginous, or bony structures. Avulsion injuries usually arise from high-velocity activities or exposures such as motor vehicle collisions, blasts, and assaults, resulting in shearing of tissues. On occasion, microsurgical techniques will be required for reattachment of avulsed tissues. Conservative trimming of nonviable tissue margins may be necessary; however, tissue-sparing management is preferred with frequent checks to confirm tissue viability. If there are concerns over viability, steps should be taken to optimize tissue vascularity, such as suture removal or wound drainage (5). Specific considerations with respect to management are discussed under each anatomical site.
Lacerations
Lacerations typically occur from impact or sharp objects resulting in a cutting of the skin as opposed to the tearing forces that result in avulsion injuries. Lacerations can be further categorized as linear, tangential, or stellate and are many times jagged with macerated edges. The majority of facial soft tissue injuries fall under this category and the tenants of closure and management are discussed in greater detail throughout the chapter.
Puncture/Penetrating
Wounds that puncture the skin are classified as puncture wounds. Those that enter and exit the skin such as a knife or bullet are known as penetrating wounds. Many times, the underlying damage is more severe than the visible portion of the wound and caution should be exercised in assessing the patient or probing of the wound. The basic principles of acute trauma care apply. Penetrating wounds of the neck can be stratified into a level I to III classification system. Please refer to Chapter 76 for further discussion and management strategies.
Crush Injuries
Prolonged or excessive force placed on any anatomical location can lead to a crush injury. Luckily, the face is seldom the site involved with isolated crush injuries. However when segments of the face, head, and neck are
involved disastrous consequences may occur. Devitalized tissue is frequently present due to small blood vessel injury leading to necrosis and poor wound healing. Management includes conservative trimming of nonviable tissue margins. Hyperbaric oxygen treatments have been shown to be beneficial for hypoxic wounds in limb crush injuries, but no randomized controlled trials have been performed that provide useful guidelines for facial soft tissue injuries (6).
involved disastrous consequences may occur. Devitalized tissue is frequently present due to small blood vessel injury leading to necrosis and poor wound healing. Management includes conservative trimming of nonviable tissue margins. Hyperbaric oxygen treatments have been shown to be beneficial for hypoxic wounds in limb crush injuries, but no randomized controlled trials have been performed that provide useful guidelines for facial soft tissue injuries (6).
WOUND MANAGEMENT
General Considerations
Regardless of whether the injury is an abrasion, avulsion, or laceration, the initial management is the same. Keeping the wound moist with sterile saline-soaked gauze is recommended. Most wounds can be examined and repaired in the emergency department trauma bay or exam room. Exceptions include those injuries with underlying fractures, nerve, salivary, or lacrimal duct injuries, which will require more complex techniques for repair. Additionally, the pediatric population will often require conscious sedation or a general anesthetic for appropriate examination and closure, depending on the injury, patient’s age, and level of cooperation.
Before repair, and many times before a thorough examination, local anesthesia is administered. Once appropriate anesthesia has been achieved, the surgeon can proceed with tissue manipulation and attention should be turned to systematic cleansing of the tissues using sterile normal saline. Various methods can be employed to accomplish removal of foreign debris and bacteria. Whether using a bulb syringe, intravenous catheter on a syringe, or pulsatile irrigator, the goal is to decrease the wound bacterial load. The presence of a wound inoculum of 105 bacteria per gram of tissue has been shown to increase the risk of wound infection. Three to five hours are generally needed for bacterial proliferation to reach this inoculum in a clean wound, and after 8 hours the bacterial load increases exponentially (7). Others have described using tap water (8) or forgoing any irrigation in the setting of a clean, noncontaminated, nonbite wound to the face and scalp and did not observe an increased rate of infection (9). The authors still advocate wound irrigation with sterile normal saline, as an inexpensive, effective, and noninvasive measure (4).
All dirt, debris, and foreign material must be carefully and thoroughly removed to avoid the risk of infection or traumatic tattoos. If irrigation techniques are not sufficient, then a scrub or wire brush may be used to remove all material, paying careful attention as to not further damage the delicate tissues or devitalize any partially avulsed flaps. Solvents used to dissolve materials such as tar are only used if absolutely necessary. Wound exploration and dissection may be needed to remove larger pieces of foreign material. Wound debridement of any nonviable soft tissue is performed with removal of necrotic tissue at the initial encounter and subsequent encounters. If there is a question of tissue viability, Futran advocates retaining the tissue and allowing a 24- to 72-hour window for final declaration (10).
For large open wounds, the use of negative pressure wound therapy (NPWT) can be utilized in those patients awaiting definitive therapy. This modality allows promotion of granulation tissue through increased blood flow to the wound, cellular proliferation from mechanical stress placed on the cells at the wound surface, as well as the removal of factors that inhibit wound healing, while avoiding painful dressing changes (11). Contraindications to NPWT related to soft tissue trauma are few, and include fragile skin, ischemic tissue, and the presence of infection (11). Contours of the face, nose, lips, and ears can make this technique difficult to apply in many cases.
Timing of Repair
The proper sequencing and staging of surgical care of facial trauma patients is important in decreasing postoperative complications and obtaining optimal results (5). Based on the wound classification and extent, decisions are made as to whether the injury is amenable to repair in the emergency room versus the operating room. Often patients will be prioritized based on other injuries.
Although the timing of repair has been controversial over the course of the past 20 years, the paradigm has shifted to immediate definitive repair after irrigation and initial meticulous debridement of devitalized tissue. Hochberg et al. argue that the best period for primary repair is within 8 hours of the injury. Tissues are less vulnerable to infection, and wound healing is at its optimum during that time, although this is also dependent on the etiology, the patient’s health, and the type of injury (12).
In patients with life-threatening injuries such as intracranial, cervical spine, and severe abdominal or thoracic injuries, surgical closure can be delayed. In those patients with contaminated wounds, delayed repair is preferred due to increased risk of infection. Local wound care and secondary healing can be considered in grossly contaminated wounds as well as those with tissue loss. Allowing wound contracture to occur may minimize the ultimate defect. Delayed closure is reserved for grossly contaminated wounds, selected animal bites, infected wounds, and wounds greater than 24 hours old. Treating with antibiotics and local wound care for approximately 3 to 5 days has been shown to yield the lowest bacterial counts at 96 hours after the injury, optimizing healing following delayed closure (7,13).
Anesthesia
Local Anesthesia
Local anesthesia is usually sufficient to repair most facial lacerations in adults and children. The choice of local anesthetic depends on the length of procedure as well as any known allergies or side effects noted by the patient.
Lidocaine (1%) with 1:100,000 dilution of epinephrine provides a dense block with appropriate time to close most lacerations. The epinephrine acts as a vasoconstrictor, which prolongs the anesthetic effects of lidocaine and provides hemostasis. In the authors’ experience, infiltration of lidocaine with epinephrine has been without consequence in end arterial areas such as the nose and ear, and feel there is no literature to substantiate its prohibition. The only exception would be its use in tissues, which appear to have a tenuous blood supply. Dosing limitations should be closely monitored in children and polytrauma patients, especially if multiple teams are using local anesthetics. The maximum recommended dose is 4.5 mg/kg for lidocaine and 7 mg/kg for lidocaine with epinephrine (13,14). The pain associated with the injection of the local anesthetic can be minimized and is influenced by temperature, pH, number of injections, rapidity of injection, and size of needle (15). Warming the anesthetic solution to body temperature, as well as achieving a more alkaline pH with the addition of 1 milliliter (mL) of sodium bicarbonate to 9 mL of lidocaine (1:10 dilution), should attenuate the pain of injection. Additionally, inserting the needle through the wound instead of penetrating the skin, as well as injecting slowly through a 27 or 30 gauge needle, will aid in lessening discomfort.
Lidocaine (1%) with 1:100,000 dilution of epinephrine provides a dense block with appropriate time to close most lacerations. The epinephrine acts as a vasoconstrictor, which prolongs the anesthetic effects of lidocaine and provides hemostasis. In the authors’ experience, infiltration of lidocaine with epinephrine has been without consequence in end arterial areas such as the nose and ear, and feel there is no literature to substantiate its prohibition. The only exception would be its use in tissues, which appear to have a tenuous blood supply. Dosing limitations should be closely monitored in children and polytrauma patients, especially if multiple teams are using local anesthetics. The maximum recommended dose is 4.5 mg/kg for lidocaine and 7 mg/kg for lidocaine with epinephrine (13,14). The pain associated with the injection of the local anesthetic can be minimized and is influenced by temperature, pH, number of injections, rapidity of injection, and size of needle (15). Warming the anesthetic solution to body temperature, as well as achieving a more alkaline pH with the addition of 1 milliliter (mL) of sodium bicarbonate to 9 mL of lidocaine (1:10 dilution), should attenuate the pain of injection. Additionally, inserting the needle through the wound instead of penetrating the skin, as well as injecting slowly through a 27 or 30 gauge needle, will aid in lessening discomfort.
In the case of children, or those intolerant to local injections, topical anesthetics are available and can be used as an alternative or adjunctive method of local anesthetic administration. Several topical anesthetics are available and are generally a combination of tetracaine, adrenaline, and cocaine (or TAC); a combination of lidocaine, epinephrine, and tetracaine (or LET); or a combination of 2.5% lidocaine and 2.5% prilocaine (16). Application of topical anesthetics as an adjunct prior to needle infiltration may reduce the pain of infiltration and can sometimes be used solely for small superficial lacerations. Bear in mind that these must be applied and left in place with an occlusive dressing for 30 to 60 minutes or more for a pronounced effect.
Regional Anesthetics
Local infiltration of anesthetic suffices for most wounds although regional nerve blocks may also be appropriate in some settings. Nerve blocks of the ophthalmic division of the trigeminal nerve (supraorbital, supratrochlear, infratrochlear) are performed with an injection along the supraorbital rim from lateral to medial, while stretching the eyebrow laterally. This can be used for scalp, upper eyelid, nose, and with the addition of auriculotemporal and zygomatic branch blockade, the temporal region can also be anesthetized. Anesthesia of the lower eyelid, cheek, nose, and upper lip through blockade of the infraorbital nerve aids in closure of lacerations in these areas. Nasal blockade can be more easily performed with appropriate regional blocks and topical anesthetics. Lidocaine or cocaine can be applied to the nasal mucosa by means of cotton tip applicators or pledgets, while the lower lip and chin can be blocked through the use of mental nerve blocks (15).
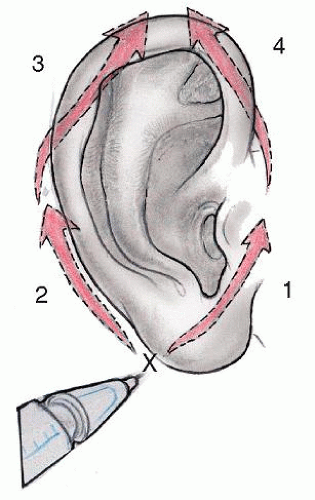 Figure 75.1 Regional block technique providing anesthesia to the entire ear, excluding the concha and EAC. “X” is the point of initial needle insertion. Numbers 1-4 denote the sequence of injections. |
Complete regional blockade of the ear is possible with the exception of the concha and medial surface of the tragus which require direct injection if necessary. Prior to injection, a cotton ball should be placed in the external meatus to block any blood from entering the external auditory canal (EAC). Using a circumferential approach, a single inferior injection aimed anterior superior in the auriculotemporal distribution is performed. This is followed by a postauricular injection directed from inferior to superior through the same injection site, without removing the needle below the lobule. Once anesthesia has set in a second pain-free needle stick can be performed superiorly into the posterior auricular area following the postauricular sulcus while avoiding the postauricular artery. The final block is placed superior to the root of the helix, from a posterior to anterior approach (Fig. 75.1).
Tetanus
Tetanus vaccination history is an important feature of any trauma patient. Wounds can be divided into tetanus-prone versus those that are not. Tetanus-prone wounds include those greater than 6 hours old, stellate lacerations, avulsion injuries, wounds deeper than 1 cm, and those with a mechanism of injury from a missile, crush, burn, or frostbite. Those wounds presenting with signs of infection, containing deinnervated or devitalized tissue or contaminants such as dirt, soil, feces, or saliva are also at high risk (7). If both tetanus immune globulin and tetanus-diphtheria toxoid are given, they need to be given in different syringes and at separate sites (7,16). Dosing is beyond the scope of this chapter but recommendations from the Centers for Disease Control and Prevention (CDC) are shown in Table 75.1.
Antibiotics
According to the guidelines distributed by the American Academy of Otolaryngology—Head and Neck Surgery, the use of prophylactic antibiotics are recommended
for traumatized or contaminated wounds, incisions or wounds crossing mucosal barriers, patients with prosthetic devices, and patients with compromised host defenses (13). Other factors that must be considered include the mechanism of injury and the time of presentation, with those patients presenting with wounds greater than 24 hours from the incident clearly having a higher bacterial inoculum and likelihood of infection. Other wounds such as compound fractures of the mandible or maxilla with mucosal breech, contaminated wounds, or injuries that occurred under water deserve prophylactic antibiotic treatment as well (17). No literature exists to support routine prophylactic antibiotic usage in soft tissue injuries to the face, so the authors follow the guidelines outlined above.
for traumatized or contaminated wounds, incisions or wounds crossing mucosal barriers, patients with prosthetic devices, and patients with compromised host defenses (13). Other factors that must be considered include the mechanism of injury and the time of presentation, with those patients presenting with wounds greater than 24 hours from the incident clearly having a higher bacterial inoculum and likelihood of infection. Other wounds such as compound fractures of the mandible or maxilla with mucosal breech, contaminated wounds, or injuries that occurred under water deserve prophylactic antibiotic treatment as well (17). No literature exists to support routine prophylactic antibiotic usage in soft tissue injuries to the face, so the authors follow the guidelines outlined above.
TABLE 75.1 TETANUS PROPHYLAXIS IN WOUND MANAGEMENT | ||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||
Oral penicillins are the antibiotics of choice, although in penicillin-allergic patients use of clindamycin or cephalexin should be considered. Fluoroquinolones are suitable for pseudomonal coverage in the case of underwater injury. In general 5 to 7 days is sufficient for prophylactic antibiotics. Grossly infected wounds are given therapeutic treatment with 48 hours of intravenous antibiotics, followed by a total 10 to 14 days of the oral equivalent. The pharmacology and microbiology of bite and burn wounds are discussed separately.
LACERATION REPAIR
When closing facial wounds the inherent bond between function and aesthetics cannot be overemphasized. The surgeon’s closure has bearing not only on societal cues, but also in the patient’s everyday functions of communication, breathing, alimentation, and display of emotions. This must also be considered when preparing and debriding the wound as distortion of contiguous structures can occur with overaggressive debridement or skin advancement. Complex or stellate wounds can sometimes be excised or converted to simple lacerations which can then be closed primarily. Delicate and atraumatic handling of the tissue edges is of utmost importance. The use of skin hooks is preferred in handling these damaged tissues as to avoid further crushing of the wound edges. Even with meticulous closure of complex lacerations, it is important to communicate to the patient and family that scar revision may be necessary.
Soft Tissue Principles of Closure
The aim of suture techniques in facial injuries is to achieve a tension-free closure with appropriate and accurate tissue approximation. When applicable, closure along the relaxed skin tension lines and abiding by the facial aesthetic units, can aid in making a scar more inconspicuous (Fig. 75.2). The amount of undermining necessary prior to closure varies with the degree of tension anticipated with the closure. A minimum number of nonreactive sutures should be used for the deep layer. Although meticulous closure may provide better tissue alignment, excess deep sutures may lead to a foreign body reaction. Too many skin sutures may compromise blood supply to the wound
resulting in local necrosis, most notably at the end organ sites of the nose, ear, or avulsed segments with a tenuous blood supply (5).
resulting in local necrosis, most notably at the end organ sites of the nose, ear, or avulsed segments with a tenuous blood supply (5).
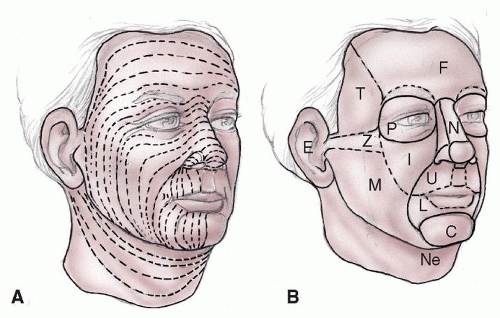 Figure 75.2 A: The relaxed skin tension lines (RSTL) should be used in closure design and incision planning. B: Depiction of the facial aesthetic units, highlighting the importance of separate reconstruction for each unit. F, forehead; T, temple; Z, zygomatic; M, mandibular; C, chin; L, lower lip; U, upper lip; N, nasal; I, infraorbital; P, periorbital; Ne, neck; E, ear. |
Suture selection is based on several factors including the depth of the injury, the extent of skin loss, the anatomic structures involved, and surgeon preference (18). Generally, a braided or monofilament deep absorbable suture is used with the knot inverted to take tension off the wound and provide appropriate reapproximation without undue strangulation or tension. Some authors, especially in the setting of contaminated or bite wounds, prefer minimally reactive monofilament sutures (e.g., polydioxanone) over more reactive, braided sutures (e.g., polyglactin) for deep closure. The theoretical increased risk of infection due to bacteria becoming embedded within the braids as well as these sutures eliciting increased tissue inflammation make monofilament absorbable preferred by some authors (19).
The subcuticular or dermal suture provides wound edge eversion and depth equality at the level of the skin for a smooth cosmetic result. The epidermal layer closure has multiple possible techniques (running, interrupted, locking) and options including sutures, staples, tapes, and liquid adhesives. Whether one uses a fine nonabsorbable (e.g., polypropylene) versus an absorbable suture (poliglecaprone 25 or fast absorbing gut) will depend on the surgeon’s preference, the likelihood of the patient returning for follow-up, and whether a child will cooperate with suture removal in clinic. Parell and Becker noted no difference in long-term cosmetic results of repairs with permanent versus absorbable sutures and thus preferred absorbable sutures. The advantages were that the sutures do not necessitate removal, thereby saving the surgeon time while lessening patient anxiety and discomfort (20). Others have investigated tissue adhesives as an alternative to suture closure as means of saving time and offering greater convenience and comfort to the patient, especially in the pediatric population. Their usefulness in the management of simple lacerations is well accepted; however, they are less useful in complex lacerations, have low tensile strength, and cannot be used around moist mucous membrane due to premature adhesive dissolution and release (21). Graphic representation of various suturing techniques is depicted in Figures 75.3 and 75.4.
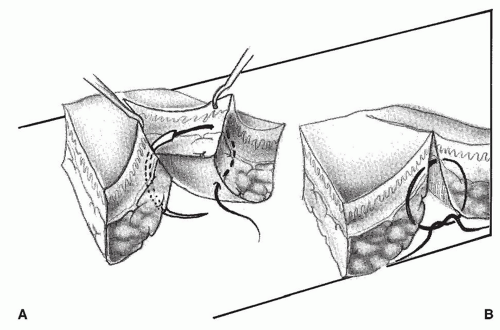 Figure 75.3 Suturing principles for facial wounds. A: Inverted deep sutures reapproximate the wound edges, eliminate dead space, and juxtapose similar tissue layers. B: Eversion of surface by well-placed sutures. |
Postoperative Care
The importance of wound care should be stressed to patients and families. The wound should be cleansed twice daily using half strength hydrogen peroxide to prevent crusting. A topical antibiotic ointment should be applied after each cleaning. Since 7% to 13% of patients develop atopic dermatitis associated with neomycin-containing ointments, we recommend avoiding ointments containing neomycin (22). Alternative ointments include bacitracin, mupirocin, or those not containing an antibiotic such as petroleum ointment or water-based ointments such as Aquaphor (Beiersdorf AG, Hamburg, Germany). Sutures on the face are generally removed in 5 to 7 days following repair.
Once the sutures are removed meticulous care should be taken to avoid sun exposure. The use of broad spectrum UV-A and UV-B sun block with an sun protection factor (SPF) greater than 45 is recommended for a minimum of 6 months to 1 year to prevent hyperpigmentation of the scar.
Intraoral and intranasal sutures are usually absorbable and these do not require removal. Antibacterial mouthwash such as chlorhexidine gluconate 0.12% is used three times daily after meals for 1 week for intraoral lacerations. The use of saline nasal rinses can be advised with avoidance of nasal manipulation or nose blowing in the setting of nasal injuries.
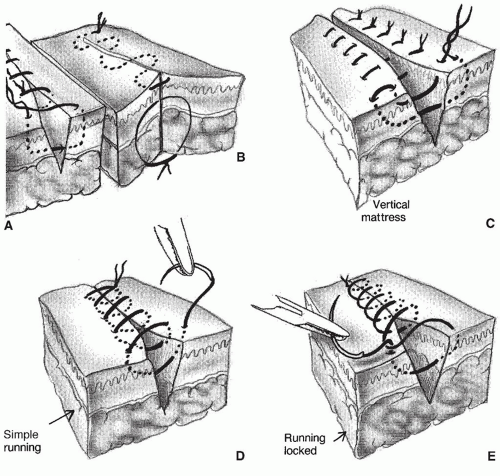 Figure 75.4 Suturing techniques. A: Simple interrupted. B: Subcuticular running. C: Vertical mattress. D: Simple running. E: Running locked. |
Drains
The use of drains in acute facial trauma is not routine but may be advisable in wounds with extensive dead space or following closure after evacuation of a hematoma. A simple latex (e.g., Penrose) drain may be used to facilitate drainage and inhibit reaccumulation. In areas with a large dead space closed suction drains may be more appropriate.
INJURIES BY ANATOMICAL LOCATION
Scalp
Injuries to the scalp are often present as gaping lacerations or avulsions. The scalp is made up of five distinct tissue planes easily remembered by the mnemonic SCALP: S (skin), C (subcutaneous tissue), A (galea aponeurotic layer), L (loose areolar tissue), and P (pericranium) (Fig. 75.5). The layered makeup of the scalp make scalp avulsion injuries more frequent, with each layer providing a plane for dissection (23). The vessels, lymphatics, and nerves course through the subcutaneous layer just superficial to the galea, while the loose areolar tissue or subgaleal plane allows for scalp mobility. As such, scalp avulsions routinely occur through this layer, thereby leaving pericranium intact, which is an important anatomic landmark that must be distinguished at time of closure and reconstruction (23).
The scalp is a highly vascular region. The presence of a rich network of vessels contributes to the profuse bleeding seen in scalp injuries, many times out of proportion to the wound size. Direct pressure is necessary and sufficient
to temporize bleeding until further examination can be undertaken. Injection of lidocaine with epinephrine into the wound edges can help in temporizing bleeding as well. When necessary full-thickness sutures can be placed to aid in hemostasis.
to temporize bleeding until further examination can be undertaken. Injection of lidocaine with epinephrine into the wound edges can help in temporizing bleeding as well. When necessary full-thickness sutures can be placed to aid in hemostasis.
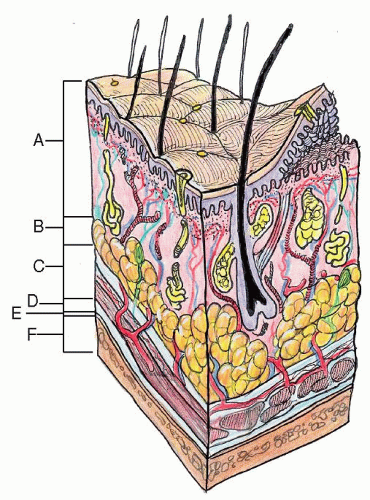 Figure 75.5 Five layers of the scalp: A, skin; B, subcutaneous tissue; C, galea aponeurosis; D, loose connective tissue; E, pericranium; F, calvarium (skull). |
Evaluation
Physical examination should proceed in a systematic fashion with specific attention turned to the neurological examination. Underlying skull fractures or associated intracranial processes must be considered. Particular attention should be paid to the present hair distribution and hairline. Wound closure should preserve these landmarks whenever possible. Small areas of alopecia may be managed by wide scar excision or hair transplantation in the future (24).
Closure
Wound preparation should be performed with copious irrigation, and undermining should proceed in the subaponeurotic plane. The scalp is known for its inelasticity, and moving adjacent tissue for wounds greater than 3 cm in size can pose great difficulty. Some authors recommend galeal incisions placed parallel to the laceration in hopes of recruiting an additional 1 to 1.5 cm of tissue and help decrease wound tension during closure. This maneuver requires clinical judgment and experience and is almost never performed by the authors. This strategy is at the expense of tensile strength and vascularity, limiting its use in larger defects (24).
For moderate defects of 2 to 2.5 cm in size, Leedy et al. (23) recommend use of V-Y flaps, V-Y-S flaps, subcutaneous pedicled flaps, or rotation advancement flaps. For large defects with intact pericranium, options include use of split-thickness skin grafts and secondary tissue expanders as well as flap reconstruction (23). If the pericranium is intact, the authors usually allow healing by second intention, thus allowing wound contraction to make the ultimate defect smaller. Reconstructive maneuvers mentioned above are seldom employed at the initial repair.
If the pericranium is not intact, but the surrounding scalp is viable, rotation or other scalp flaps can be used to fill the defect, with skin grafts or primary closure used at the donor-site defect. Large defects without pericranium can be treated with open wound care and complex reconstruction techniques such as rotation-advancement flaps or free tissue transfer can be performed in a delayed fashion.
Total avulsion or near-total avulsion injuries are best managed by microvascular reanastomosis and replantation if the scalp tissue is viable and available. If this option is not available, the authors would typically treat the open wound and then decide upon a strategy that might include a STSG versus flap reconstruction. Leedy et al. (23) feel that free tissue transfer is the best option such as a free latissimus-serratus flap.
The use of 4-0 running locking nonabsorbable suture is advocated for appropriate hemostasis and wound closure at the level of the galea and dermis. Cosmetic results following skin closure have been shown to be equivalent with the use of staples as opposed to sutures, in the pediatric population. Additionally, benefits from time savings, costs, and decreased wound closure times were noted (25




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
