Chapter 60 Management of Postoperative Cerebrospinal Fluid Leaks
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
PRESSURE DRESSING
Technique
The dressing is applied in similar manner to the initial postoperative dressing. First, a vertical gathering tie is placed in the temporal fossa. Dressing sponges (4 × 4) are folded in half and placed directly over the fat graft and in the postauricular sulcus to support the auricle (Fig. 60-1A). Next, fluffed Kerlix is placed over the 4 × 4 sponges and the auricle (Fig. 60-1B). A tight wrap of roller gauze is applied (Fig. 60-1C). The direction of the wrap should be from the ear toward the occiput, which ensures that the auricle is not damaged by anterior folding. Also, the vertical tie must be as lateral as possible in the temporal fossa to avoid a pressure point on the forehead. Pressure necrosis of forehead skin can develop easily if attention is not given to this point.
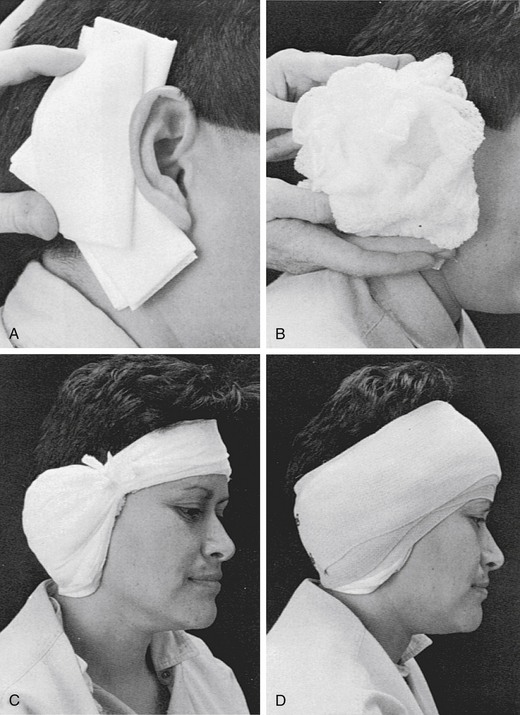
The last layer of this dressing is a 3-inch elastic bandage, which provides the final compression (Fig. 60-1D). The elastic bandage should be wrapped firmly, but patient comfort must be accommodated. Usually, the last several turns can be altered to adjust the exact amount of compression. Ideally, a pressure dressing should be left in place for 4 or 5 days, which allows time for healing of the CSF leak site to occur. A minimum of 48 hours without leakage must pass before the dressing is removed.
LUMBAR DRAIN
Technique
To place the catheter, a lumbar puncture is performed at the L4-L5 level. The patient is placed in either a sitting or a lateral decubitus position. The spinous processes are palpated, and L4-L5 is identified at the level of the iliac crest. The patient is asked to flex the back and bring the knees and chin to the chest. A prepared catheter kit contains all the necessary supplies for preparing, draping, and anesthetizing the site. A 14 gauge Tuohy needle is introduced in the midline with a slightly superior angle between the spinous processes (Fig. 60-2). The obturator is removed at intervals so that the surgeon can look for a flow of CSF. When a good flow of CSF is established, the epidural catheter is introduced through the needle and threaded into the epidural space. The opened side of the bevel of the needle faces the patient’s left or right side on penetrating the spinous ligaments and arachnoid. Before the catheter is threaded, the bevel is turned to open superiorly, facilitating directing the catheter cephalad. With a flow of CSF established, the needle is withdrawn, and the connector is placed on the end of the catheter so that a connection to intravenous tubing can be made. An empty intravenous fluid bag is attached to the tubing, and all connections are secured with tape (Fig 60-3A).

Several methods of regulating CSF output exist. This regulation is important because, if CSF is removed too rapidly, tension pneumocephalus and brain herniation can occur.1–3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


