Management of Posterior Capsule in Pediatric Cataract Surgery
Paolo Nucci
Massimiliano Serafino
M. Edward Wilson
Posterior capsule opacification (PCO) caused by postoperative proliferation of cells in the capsular bag remains the most frequent complication of pediatric cataract surgery. In the normal lens, epithelial cells are located to the anterior surface at the equatorial region and at the equatorial lens bow. Lens epithelial cells can be divided into two different types1:
Anterior epithelial cells (A-cells) with minimal mitotic activity and the capability to proliferate and undergo fibrous metaplasia if stimulated. A-cells are responsible for fibrosis PCO.
Equatorial lens bow cells (E-cells) with active mitoses and migration. E-cells are responsible for pearls or cluster PCO.
PCO is actually a misnomer because it is not the capsule that opacifies. Actually, retained epithelial cells proliferate and migrate on the posterior capsule surface, resulting in loss of transparency at the level of the posterior capsule (Fig. 99.1).
Several factors contribute to secondary membrane formation after cataract surgery influencing the incidence of PCO. These include the age of the patient at the time of cataract surgery, associated ocular anomalies, the extent of cortical clean up, management of the posterior lens capsule and anterior vitreous, intraocular lens (IOL) design, material, and site of fixation, and surgical trauma.2,3
Definitely, PCO prevention has been an active research interest for many authors. The main strategy has been to minimize the number of retained epithelial cells and lens cortex with careful and complete aspiration during cataract removal. The second strategy has been to prevent the retained cells from migrating posteriorly. The edge design of the IOL is crucial for this purpose.1 For pediatric patients, the following questions are important when considering PCO: When should the posterior capsule be opened and when can it be left intact? Is an anterior vitrectomy necessary when a surgical posterior capsulotomy is performed? When performing a posterior capsulotomy and an anterior vitrectomy, is an anterior (limbal) or a posterior (pars plana/plicata) approach preferable? At what age is a Nd:YAG laser capsulotomy preferred over a surgical capsulotomy? Is it safer to perform a surgical capsulotomy before or after IOL implantation? When performing an anterior vitrectomy, how much vitreous should be removed?
POSTERIOR CAPSULE OPENED OR INTACT?
If the posterior capsule is left intact in young children, PCO is fast and inevitable with reported rates up to 100%.6,7 There is a strong relationship between the rate of PCO and the age at surgery. This probably reflects the increased metabolic activity of lens epithelial cells in young children. Most surgeons prefer to perform a primary posterior capsulotomy when operating young children to prevent PCO and thus prevent worsening of the amblyopia. Others advocate leaving the posterior capsule intact initially, even in young children, because it is a physiological barrier between anterior and posterior segments of the eye. Considering that visually significant PCO most commonly develops 18 months to 2 years after surgery, it is reasonable to leave the posterior capsule intact if after that period, the child will be cooperative enough to undergo a Nd:YAG laser procedure.
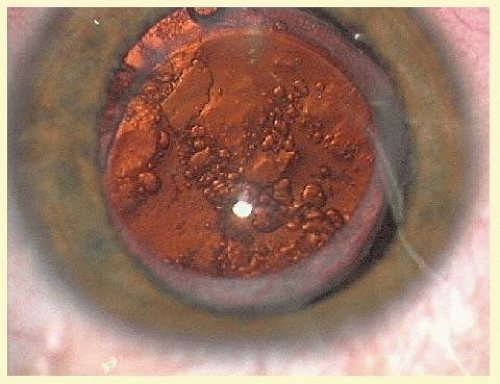 FIG. 99.1 Dense PCO in a 7-year-old boy. |
Based on our experience and a review of the literature, we recommend leaving the posterior capsule intact if a developmentally normal child is 5 years of age or older at the time of surgery. We consider performing a primary surgical capsulotomy and anterior vitrectomy when the child is younger than 5 years, posterior capsule defects are present, a Nd:YAG laser is not available, or the child is deemed not likely to be cooperative for YAG laser procedure even 18 to 24 months into the future.
POSTERIOR CAPSULOTOMY AND ANTERIOR VITRECTOMY
In order to avoid vitreous face opacification, anterior vitrectomy is crucial in patients up to 5 years of age. After this age there are more chances that the visual axis will be clear for a long period. If the anterior vitreous surface is left intact and it opacifies later, pars plana or limbal anterior vitrectomy can be performed as a separate procedure when it becomes necessary.4
Hutcheson et al.8 concluded that with the removal of anterior vitreous at the time of cataract surgery, the scaffolding for cell migration is also removed and reopacification of the visual axis is rarely seen.9
Posterior capsulotomy can be performed with the manual technique (capsulorrhexis) or with the vitrector (vitrectorhexis). It is important to emphasize that the posterior capsule is three to five times thinner than the anterior capsule and that mechanical strength and forces required to break the posterior capsule decrease markedly with age.10 A manual posterior capsulorrhexis creates an opening with a strong margin. It allows for the possibility of a safe IOL implantation and yet a preserved vitreous face. However, when anterior vitrectomy is planned, we, and many surgeons, prefer to use the vitrector to perform the capsulotomy.
The risk of cystoid macular edema (CME) and retinal detachment is lower after posterior capsulotomy and anterior vitrectomy in children than originally thought.11,12
Surgical Technique
Posterior Capsulotomy
After aspiration of lens material, the capsular bag is filled with a high-viscosity ophthalmic viscosurgical device (OVD) and capsulorrhexis can be initiated. It is better to start the capsulorrhexis with a puncture of the posterior capsule with a cystotome. At this point some surgeons prefer to inject additional OVD between the posterior capsule and the anterior vitreous. The posterior capsulorrhexis can be accomplished using capsulorrhexis forceps.
Vitrectomy
If a pars plana approach is chosen, it is important to keep in mind that pars plana begins at 2.2 and 2.5 mm from the limbus for the nasal and temporal aspect, respectively, at less than 6 months of age, 2.7 and 3 at 6 to 12 months, 3.0 and 3.1 at 1 to 2 years of age, and 3.2 and 3.8 at 2 to 6 years of age. The term “pars plana” approach in very young infants is a misnomer because, in the newborn, the pars plana is not well developed. In these infants, the surgical approach is more accurately called a pars plicata entry13 (Fig. 99.2A and B).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


