Management of Intractable Aspiration
David E. Eibling
Aspiration pneumonia accompanies a wide variety of disease states, and often contributes substantially to the impact on the patient. Inhalation of food and liquid into the lower airways is recognized as a contributing factor in the death of many patients, and is frequently the terminal event. Stroke is a well-known example, in that although aspiration risk is transitory in most stroke patients, a considerable percentage of those with persistent dysphagia (20% to 50%) will eventually succumb to aspiration pneumonia (1,2,3). Mitchell et al. reviewed the clinical course of 323 nursing home patients with advanced dementia and noted that more than 50% had died within 18 months, and that the combination of dementia and aspiration was particularly deadly. The 6-month mortality rate for patients with advanced dementia who had eating difficulties was 38.6%; if they developed pneumonia the figure rose to 46.7% (4). Despite the prevalence of aspiration in many disease states, and its often grave impact on the patient, (not to mention the cost to the health care system) the evaluation and management of aspiration remain enigmatic to many, if not most, health care providers. Most aspirating patients are managed by nonsurgical means, addressed in Chapter 58. This chapter focuses on surgical management of aspiration unresponsive to conservative measures.
IDENTIFICATION OF ASPIRATION
One might suspect that clinically significant aspiration would be readily apparent to the patient’s caregivers. However, the signs of aspiration are frequently attributed to the primary disease, and aspiration may remain unrecognized until the terminal phase of the disease process. Neurologic impairment masks the usual symptoms of aspiration, particularly by facilitating so-called silent aspiration. Common manifestations of aspiration are enumerated in Table 60.1.
Aspiration pneumonia entails substantial costs for the health care system (not to mention the patient) hence most health care facilities have introduced standard screening procedures to identify patients at risk for aspiration. These are most commonly developed and overseen by a dysphagia team, typically organized and led by a senior speech-language pathologist (SLP). Screening is usually performed by admitting nursing staff. Patients determined to be at risk are then evaluated by the multidisciplinary dysphagia team headed by a SLP with expertise in dysphagia who makes recommendations for further evaluation and/or intervention. In some facilities, an otolaryngologist is an integral part of the team (5); however, in others the team functions effectively without physician oversight. The Joint Commission removed the requirement for universal dysphagia screening of all stroke patients in 2010; however, other performance-monitoring organizations continue to include screening for aspiration risk in their bundles (2). High-level evidence exists that improved outcomes (reduced episodes of pneumonia) are correlated with the presence of a dysphagia team, but no clear evidence exists to guide the team activities. In other words, paying attention in and of itself seems to be the most critical factor in promoting improved outcomes in hospitalized patients with swallowing disorders!.
ETIOLOGY OF ASPIRATION
Otolaryngology trainees encounter aspirating patients most often on the head and neck cancer service; however, the majority of patients suffering severe aspiration are those with neuromuscular dysfunction. A retrospective review of patients with intractable aspiration who required laryngotracheal separation revealed that more than twothirds had suffered devastating neurologic disease, such as amyotrophic lateral sclerosis, multiple sclerosis, or brainstem stroke (6). The aging baby boomer population
and attendant increases in the numbers of patients with dementia predict that otolaryngologists practicing in the second and third decades of the 21st century will encounter an epidemic of aspirating elderly patients. Decision making for this group of future patients will challenge today’s trainees.
and attendant increases in the numbers of patients with dementia predict that otolaryngologists practicing in the second and third decades of the 21st century will encounter an epidemic of aspirating elderly patients. Decision making for this group of future patients will challenge today’s trainees.
TABLE 60.1 DIAGNOSIS OF ASPIRATION | ||||||
|---|---|---|---|---|---|---|
|
Increased numbers of patients with head and neck cancer will survive their disease only to suffer from longterm dysphagia and aspiration. Treatment-induced acute inflammation and mucositis, as well as long-term fibrosis, xerostomia, web formation, and stenosis (or even obliteration) of the cricopharyngeal lumen, result in severe dysphagia and often frank aspiration for many cancer survivors. Acute radiation-induced dysphagia abates several weeks following completion of therapy, only to be replaced with chronic dysphagia as fibrosis develops. This dysphagia typically increases in severity with the passage of years due to progressive fibrosis and muscle weakness (7). If recent trends in the incidence of human papilloma virus—associated oropharyngeal (OP) cancer continue, otolaryngologists can anticipate growing numbers of OP cancer survivors presenting to their offices with progressive dysphagia, possibly many years after treatment. Although recent alteration in radiation fields and dose de-escalation may reduce dysphagia rates for patients treated in coming years, for the short term at least, standard doses of combined chemotherapy and radiotherapy will likely lead to increasing prevalence of posttreatment dysphagia and even morbid aspiration.
PHYSIOLOGY OF SWALLOWING
Aspiration is a sequella of disordered deglutition, so a basic knowledge of the physiology of normal swallowing is required to understand the pathophysiologic underlying etiologies of aspiration. The reader is referred to Chapters 56, 57 and 58 and to the classic references on the topic (7,8). Some indication of the primacy of airway protection can be seen by examining the phylogeny of the larynx (9). Humans are at particularly high risk for soilage of the lower airways during deglutition due to the caudal location of the human larynx. This location facilitates vocalization by enlarging the resonance cavity, but increases the risk of aspiration associated with relatively minor abberations in swallowing function. Effective swallowing requires that food and liquid be formed into a finite bolus and then moved rapidly and completely past the closed glottis. Failure to form a finite bolus, premature leakage of bolus material into the pharynx, delay in moving the bolus through the pharynx or incomplete emptying of the pharynx at the completion of deglutition permits material to be aspirated into an open glottis. Glottic incompetence during swallowing can lead to aspiration, particularly when accompanied by sensory changes or pharyngeal weakness. Aspiration pneumonia, therefore, is the end result of laryngopharyngeal dysfunction, and typically is due to neuromuscular disease.
Glottic Closure
Glottic closure is required for effective swallowing. Closure occurs rapidly (the glottic closure reflex is less than 25 ms in duration) and is reflexively triggered by the presence of bolus material in the pharynx. Interruption of the afferent limb through loss of sensation of the larynx and pharynx causes loss of this reflex and can lead to clinically significant aspiration. Aspiration often is associated with the effector limb of the reflex through vocal cord paralysis, atrophy, or other causes of inadequate glottic closure (Fig. 60.1). Sasaki et al. (10) have demonstrated that glottic closing pressure also impacts effectiveness of closure, and may be reduced following thyroplasty even if the glottis is anatomically closed. Surgical procedures designed to improve glottic closure can have a dramatic effect in the care of some patients (11).
Upper Esophageal Sphincter Relaxation
Relaxation of the cricopharyngeal muscle allows opening of the upper esophageal sphincter, facilitating passage of the bolus from the pharynx into the esophagus. The upper
esophageal sphincter is actively dilatated by anterio-superior elevation of the laryngeal cartilage immediately before arrival of the bolus. Failure of either relaxation of the muscle or of hyo-laryngeal elevation will result in retained food and bolus in the pharynx.
esophageal sphincter is actively dilatated by anterio-superior elevation of the laryngeal cartilage immediately before arrival of the bolus. Failure of either relaxation of the muscle or of hyo-laryngeal elevation will result in retained food and bolus in the pharynx.
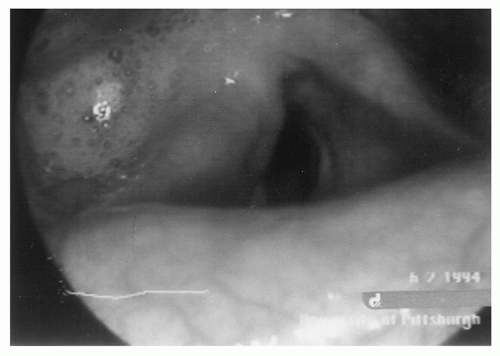 Figure 60.1 Right vocal cord and ipsilateral pharyngeal paralysis cause hoarseness and aspiration in a patient with a large glomus jugulare tumor. Saliva has pooled in the right pyriform sinus. Medialization thyroplasty was performed before tumor excision to facilitate pulmonary toilet in the postoperative course. |
TRACHEOSTOMY AND ASPIRATION
Aspiration has been noted in patients with a tracheostomy for nearly 50 years (12); however, controversy exists as to whether a cause-and-effect relationship exists. Sasaki (9) noted loss of the glottic closure reflex in the presence of a tracheostomy and Muz et al. (13) noted aspiration, which varied in extent depending on whether the tube was open or plugged. Several investigators (13,14,15) noted that plugging or placing an expiratory valve on a tracheostomy tube appeared to benefit swallowing and reduce aspiration, suggesting that subglottic air pressure played a role. Others (16) have been unable to duplicate these findings, suggesting that the specific relation between tracheostomy and aspiration varies based on patient comorbidities, age, and underlying disease.
SENSORY LOSS
Aviv et al. (17) found that stroke patients have marked reductions in pharyngeal and supraglottic sensation and that these reductions correlate with aspiration risk. Pharyngeal sensation can be measured utilizing a puff of air directed against the supraglottic structures while the larynx is observed with a flexible laryngoscope, although most examiners utilize other findings as surrogates for sensory loss (Chapter 57).
EVALUATION OF A PATIENT EXPERIENCING ASPIRATION
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


