Fig. 12.1
Anterior-segment optical coherence tomography image of the anterior chamber angle in a patient before (a) and after (b) Boston Type I Keratoprosthesis surgery. Progressive synechial angle closure was noted postoperatively and the patient suffered secondary glaucoma, necessitating glaucoma drainage implant surgery
Removal of the iris at the time of KPro surgery does not eliminate the significant risk of postoperative glaucoma. In the series reported by Netland et al., glaucoma was not eliminated in 21 (58 %) of 36 eyes treated with total removal of the iris during KPro surgery [1]. Direct injury to the trabecular meshwork and/or its distortion and collapse with resulting dysfunction may lead to glaucoma in these cases. Although pupillary block and acute angle closure glaucoma have not been reported, this event is certainly plausible and may go undetected in the postoperative period. In the absence of a surgical iridectomy, 360° irido-backplate touch could potentially lead to pupillary block and acute angle closure glaucoma.
In the postoperative period, patients that have undergone KPro surgery are often maintained on a topical steroidal agent. Steroid-response glaucoma may certainly occur in this setting to serve as a co-contributor of IOP elevation and subsequent glaucoma. It should also be noted that due to corneal opacities precluding a view of the optic nerve on preoperative assessment, preexisting glaucoma may go undetected. The increased prevalence of postoperative glaucoma may relate not only to surgical events but also to an enhanced ability to detect the disease once optic nerve visualization becomes possible in the postoperative period.
12.3 Diagnosis/Monitoring
The most challenging aspect of managing glaucoma in KPro eyes is the diagnosis and monitoring of glaucoma. As mentioned earlier, the majority of candidates for KPro surgery have preexisting glaucoma, and even those without preexisting glaucoma often develop glaucoma after surgery [4]. Hence, preoperative glaucoma evaluation and postoperative surveillance are essential in the management of patients that have undergone KPro surgery.
The evaluation of preoperative glaucoma is usually limited by poor vision and media opacity. Thus, a complete history of prior glaucoma-related evaluations and treatment should be obtained. Additionally, the angle structures and the position of glaucoma drainage devices in the eyes can be visualized with ultrasound biomicroscopy in preparation for surgery. Furthermore, it is imperative to obtain a baseline IOP with a tonometer that is less likely than a conventional Goldmann tonometer (e.g., pneumatonometer) to be affected by corneal edema and/or scarring. Lastly, if the preoperative vision allows, a baseline visual field such as a Goldmann visual field should be obtained. Otherwise, a visual field assessment by light projections should be acquired for eyes with extremely poor vision.
Postoperative surveillance of glaucoma is important for the prevention of irreversible visual loss from an otherwise successful KPro surgery. Thus, close monitoring of the IOP, visual field, and changes in the optic nerve is essential. In clinical practice, IOP measurements usually rely on palpation, since the IOP cannot be measured with current methods through the central optical zone of the KPro. A technique for assessing the IOP by palpation has been described [14, 15]. First, a patient is asked to close his/her eye while looking down. Any redundant skin of the upper eyelid can be then moved upward by the examiner’s index fingers. By alternately applying pressure with each index finger, a ballottement of the globe can be performed at the 12 o’clock meridian. Consequently, the IOP can be estimated by the firmness of the globe or the amount of force needed to move fluid between the two fingers. Baum et al. showed that although IOP estimation by palpation is not ideal, it can be useful for identifying an IOP greater than 30 mmHg [14].
In addition to an assessment by palpation, other techniques may be used as alternative methods for measuring IOP in KPro eyes, with some limitations. For example, Kapamajian et al. and Bang et al. demonstrated that IOP measurements on the sclera via pneumatonometry may be used when IOP measurements on the central cornea are not possible [16, 17]. The validity of this method is based on the positive correlation between scleral and corneal IOP measurements by pneumatonometry in healthy subjects and cadaveric eyes. However, the scleral IOP is consistently higher than the corneal IOP (an 8 mmHg difference, on average) and more accurate at a lower IOP range than a higher one. Another method that may be considered for measuring IOP in KPro eyes is the determination of transpalpebral IOP with a TGDc-01 or Diaton (BiCOM, Inc., Long Beach, NY, USA) tonometer. Losch A et al. and others have found that transpalpebral IOP measurements generally yield lower IOP readings (2–4 mmHg on average) when compared to IOP measurements by a Goldmann tonometer [18, 19]. Nonetheless, it is important to note that the accuracy of palpation, scleral pneumatonometry, and transpalpebral IOP measurements in eyes with KPro is unknown, since previous studies were performed in healthy eyes. However, a need is present for more accurate IOP measurement in KPro eyes, and the aforementioned methods offer a potential means for obtaining these measurements. Additionally, several novel methods for IOP measurements, such as radio wave telemetry and an implantable IOP sensor, have been investigated [20, 21]. These methods are not currently approved and available for clinical use.
In addition to IOP estimation, the close monitoring of changes in the visual field and optic nerve in patients with or without preexisting glaucoma remains crucial to detecting the development or progression of glaucoma after KPro surgery. Depending on the level of postoperative visual acuity, either automated (Fig. 12.2) or manual (Fig. 12.3) visual field testing may be reliably performed in KPro eyes. In patients with no glaucoma, the Goldmann visual field with the largest and brightest target (V-4e isopter) subtends approximately 95° in diameter (50° temporally and 44° nasally) [15, 22]. The optimal quality for stereoscopic optic disc photography and optical coherence tomography can be obtained through a small optical zone in the KPro eye (Fig. 12.4).
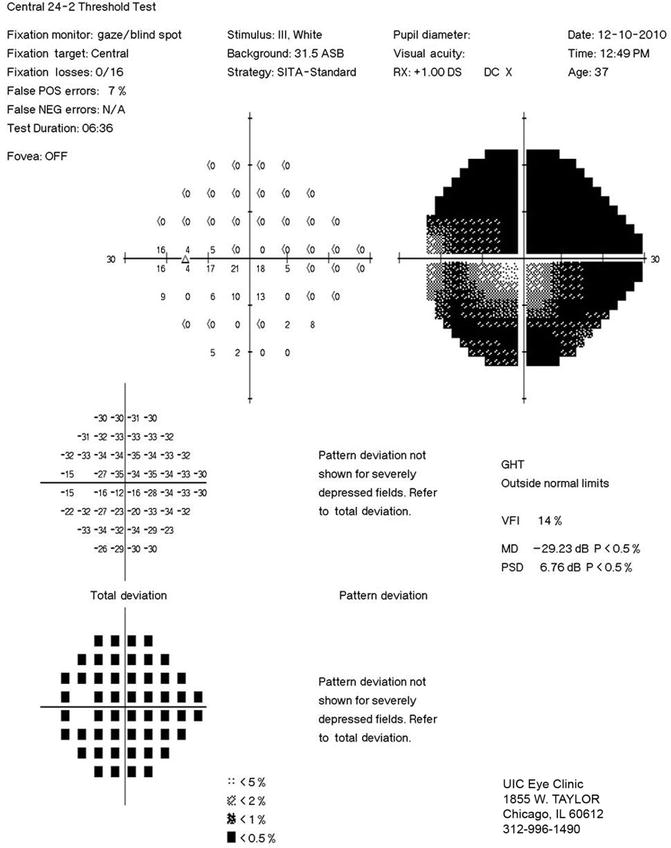
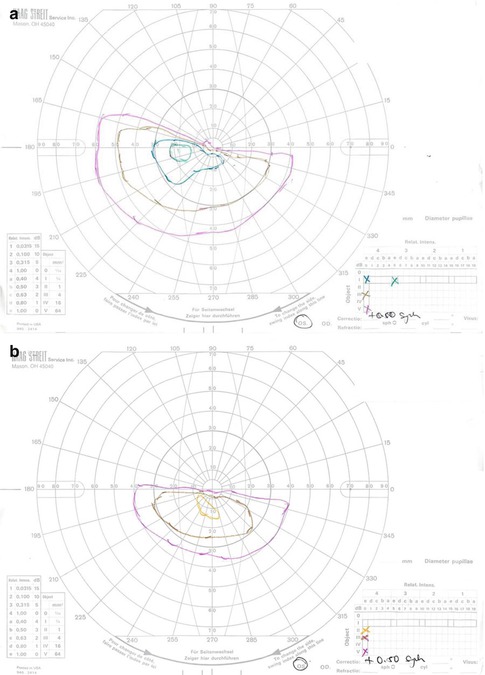
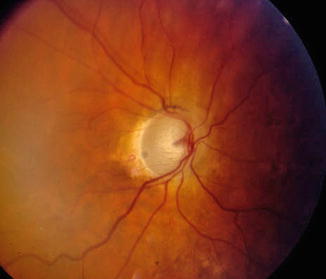
Fig. 12.2
Automated visual field plot depicting advanced double arcuate scotomas sparing fixation in a patient with secondary glaucoma of the left eye related to prior Boston Type I Keratoprosthesis surgery
Fig. 12.3
Manual Goldmann visual field plot depicting an advanced superior arcuate defect of the left eye (a) in a patient with secondary glaucoma related to prior Boston Type I Keratoprosthesis surgery. A decreased ability to detect smaller-sized targets in the inferior hemifield was noted in a subsequent plot (b) within an 8-month testing interval. Intraocular pressure-lowering therapy was escalated based on evidence of progressive functional deterioration
Fig. 12.4
Optic disc photograph of the right eye of a patient with advanced glaucomatous optic neuropathy associated with prior keratoprosthesis surgery. The patient underwent successful glaucoma drainage implant surgery for long-term intraocular pressure control and preservation of remaining visual field
Ultimately, follow-up remains challenging, and glaucoma may continue to progress despite best efforts [1, 2]. Thus, we recommend frequent routine testing. For each 3- or 4-month follow-up visit, patients with KPro should undergo IOP measurements and either visual field testing or imaging of the optic nerve to detect any early sign of glaucomatous progression.
12.4 Therapeutic Options
Current evidence indicates that glaucoma occurs in a majority of KPro patients in the postoperative period. The grave nature of this secondary glaucoma with potentially irreversible visual consequences requires an aggressive approach on the part of the treating clinician.
12.5 Medical Therapies
The degree of intraocular penetrance of currently available topical IOP-lowering agents in the setting of a KPro graft is unknown. The central polymethylmethacrylate optic likely diminishes ocular penetrance when compared to human corneal tissue. Topical medical therapies may therefore have a limited role in management of the aggressive glaucoma characteristic of KPro eyes in the postoperative period. Oral carbonic anhydrase inhibitors such as methazolamide and acetazolamide may provide an alternative medical therapeutic option in these cases. These agents are often efficacious in terms of IOP lowering, but chronic use is often limited by a host of potential systemic effects, including metabolic acidosis, urolithiasis, gastrointestinal illness, paresthesias, somnolence, confusion, bone marrow toxicity, aplastic anemia, and mental depression [23, 24]. Although Stevens-Johnson syndrome has been associated with sulfamethoxazole derivatives, its recurrence after use of oral acetazolamide in KPro patients with corneal blindness from the disease has not been noted [25].
12.6 Laser Therapies
Peripheral donor corneal opacification after KPro surgery often limits view of anterior chamber angle detail and therefore precludes the use of laser trabeculoplasty procedures for IOP-lowering purposes. Likewise, laser peripheral iridotomy or laser peripheral iridoplasty would be difficult maneuvers to perform in the postoperative period. Diode laser cyclophotocoagulation may be performed on the external ocular surface for IOP lowering after KPro surgery. In a retrospective series of 18 eyes of 18 KPro patients, Rivier and colleagues reported a significant mean IOP reduction at 6, 12, 24, 36, and 48 months after diode laser cyclophotocoagulation [26]. By final visit, mean best-corrected visual acuity was not decreased from pre-laser levels. Two post-laser complications were encountered in this series and included one case of conjunctival dehiscence, which resolved spontaneously, as well as one case of fungal endophthalmitis, which was believed to have reactivated from a subclinical level post-laser.
12.7 Incisional Therapies
Glaucoma drainage implant (GDI) surgery is an effective method for control of glaucoma associated with KPro implantation. Netland et al. reported IOP control in 81 % of eyes after GDI and KPro surgeries [1]. GDI surgery was performed in combination with the initial KPro procedure in 81 % of eyes, and sequentially in 19 % of eyes. The series involved 35 Ahmed Glaucoma Valve (AGV; New World Medical, Inc., Rancho Cucamonga, CA, USA) implants and 1 Krupin Valve implant. All implant tubes were placed in the anterior segment. Kamyar et al. also reported on the important role of GDI surgery in 30 eyes of 29 patients that underwent KPro implantation [3]. In that series, eyes that underwent GDI surgery were less likely to experience glaucoma progression or IOP elevation than those that did not.
Though effective in control of postoperative IOP, GDI surgery may certainly be fraught with long-term complications in the setting of a KPro implant. Li et al. reported on the long-term complications associated with GDIs and KPro surgery in 25 eyes after an average follow-up of 33.6 months [27]. Most implant tubes were placed in the anterior segment and a contact lens was routinely used after KPro implantation in all cases. Ten cases of conjunctival erosion over the GDI plate or tube were noted in 9 eyes in this series. Associated complications included endophthalmitis, hypotony, and keratoprosthesis extrusion, requiring GDI removal in 6 eyes. The authors postulate that preexisting ocular surface disease as well as possible focal mechanical conjunctival trauma induced by the postoperative contact lens contributed to the risk of GDI exposure. Kamyar and colleagues observed five cases of anterior-segment tube obstruction, requiring surgical revision, among 21 eyes that underwent concomitant GDI and KPro surgeries [3]. Netland et al. noted that tube obstruction was the most common complication to occur among eyes treated with GDI surgery in association with KPro implantation [1].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


