Fig. 15.1
(a) Preoperative slit lamp photograph of a patient with extensive symblepharon and forniceal foreshortening secondary to chemical burn. (b) Postoperative photograph of the same eye following fornix reconstruction and repair of symblepharon with mucous membrane graft in preparation for future Boston keratoprosthesis type 1 implantation
15.2 Exposure Keratopathy and Eyelid Malposition
The eyelids and periorbital tissue serve a vital role in promoting and maintaining a hydrated ocular surface. This is especially important after Boston KPro type 1 implantation, where surrounding dehydration of the corneal surface can lead to epithelial defects, stromal thinning, tissue recession from the front plate, and subsequent melt and device extrusion. Soft contact lens wear was found to be highly protective against evaporative damage and has significantly improved postoperative management [11]. However, ultimately, proper lid anatomy and blink function is critical in maintaining a hydrated surface and retaining a bandage contact lens to improve ocular surface stability.
The most common indication for oculoplastic intervention was exposure keratopathy (76.2 %) with most of these patients (56.3 %) also having eyelid abnormalities threatening KPro viability [10]. In these cases, lateral tarsorrhaphy was performed to reduce exposure keratopathy both by improving contact lens retention and by decreasing exposed ocular surface area. Similarly, tarsorrhaphy was also successfully used in cases of persistent epithelial defect [12].
In addition, in those cases where eyelid malposition is the cause of poor hydration or difficulty maintaining a contact lens, oculoplastic evaluation is crucial. Management depends on the underlying etiology. In some patients, eyelid retraction may cause exposure, poor contact lens tolerance, and lagophthalmos and can be corrected with lid recession (Fig. 15.2). In addition, lower lid laxity is frequently the cause of poor contact lens retention and can be resolved with a lower lid tightening procedure such as a tarsal strip procedure to improve eyelid apposition to the globe. However, certain patients may have eyelids that are tight. These eyelids can be “lengthened” with a canthotomy.
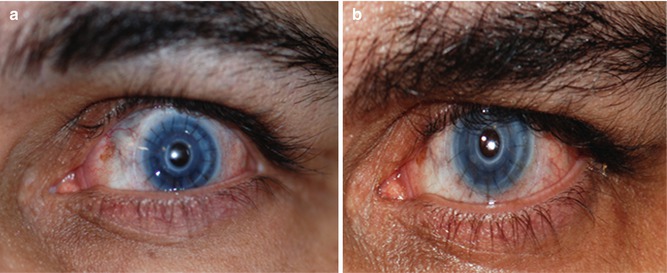
Fig. 15.2
(a) Preoperative photograph of a patient with an implanted Boston keratoprosthesis type 1 with contact lens intolerance and lagophthalmos secondary to upper eyelid retraction. (b) Postoperative photograph of the same eye after upper eyelid Müller’s muscle excision with levator recession and lateral tarsorrhaphy
15.3 Blepharoptosis
Similar to patients without a KPro, blepharoptosis can significantly decrease vision in those with an implanted KPro. When considering ptosis repair, it is important to keep in mind that while lifting the lid, there should be adequate coverage to protect the corneal graft and also to retain the bandage contact lens. Therefore, a more conservative approach is desired in these patients, and mild undercorrection is the goal. At our institution, we have performed both external levator resection and Müller muscle-conjunctiva resection (MMCR). Careful examination of the conjunctiva and fornices is vital before MMCR.
15.4 Special Considerations in Boston KPro Type 2
The Boston KPro type 2 is reserved for severe ocular surface disease, such as Stevens-Johnson syndrome, mucous membrane pemphigoid, and end-stage keratoconjunctivitis sicca [6, 13]. These patients typically have extensive symblepharon, severe aqueous tear deficiency, ocular surface keratinization, no fornices to support the device, and/or abnormal lid function.
Oculoplastic procedures are a part of the standard operative technique in KPro type 2, which has been previously described [1, 13]. The assembly of the Boston KPro type 2 is similar to type 1. However, type 2 is designed with only the anterior-most cylinder of the optic exposed through full-thickness surgically fused eyelids.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


