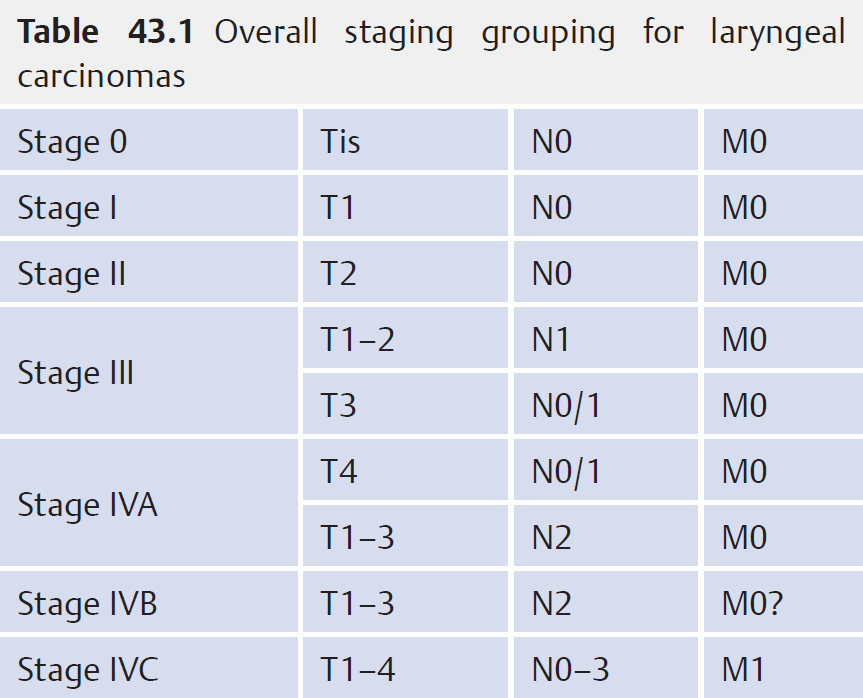
43 Malignant Laryngeal Tumours • 1% of all malignancies in British men • 85% of all laryngeal malignancies • 3 to 4 male: 1 female • Age 55–65 peak • High incidence = Brazil, United States, India, France • Low incidence = Japan, Scandinavia • Lower social class • African-Caribbean origin • Aetiological factors: • Keratosis—keratin formation by superficial layer only • Parakeratosis—nucleus retained abnormality in superficial layer of keratin-producing cells • Dyskeratosis—keratinization within prickle cell layer • Dysplasia—nuclear variation, mitosis, loss of normal epithelial layering • Ca in situ—malignant cells confined superficially to basement membrane • Ca in situ shows course abnormalities of differentiation and nuclear atypia in almost all areas of epithelium with basal cell proliferation and mitoses regards as premalignant • Classification • Suprahyoid and infrahyoid epiglottis • Chance of occult nodal mets • Classification – A—one VF – B—both VFs • Causes of VF fixation • Incidence of lymph node metastases • Classification Fig. 43.1a, b a Carcinoma of the right vocal fold (T1N0M0). b Carcinoma of the left vocal fold comprising the anterior commissure (T3N2M0). • See Table 43.1 • Verrucous carcinoma • Kaposi sarcoma All patients with malignancy should be discussed in a multidisciplinary meeting • Performance status • Patient preference • Previous treatment • Patient’s distance from treatment facility
43.1 Squamous Carcinoma (Fig. 43.1)
 Smoking
Smoking
 Dark spirit consumption
Dark spirit consumption
 Asbestos exposure
Asbestos exposure
 Formaldehyde exposure
Formaldehyde exposure
 Radiation (therapeutic for thyroid)
Radiation (therapeutic for thyroid)
 Keratosis and leukoplakia
Keratosis and leukoplakia
43.2 Squamous Intraepithelial Neoplasia
 Grade I—squamous cell hyperplasia with mild dysplasia and keratosis
Grade I—squamous cell hyperplasia with mild dysplasia and keratosis
 Grade II—keratosis and squamous cell dysplasia with occasional nuclear atypia
Grade II—keratosis and squamous cell dysplasia with occasional nuclear atypia
 Grade III—squamous cell hyperplasia
Grade III—squamous cell hyperplasia
43.3 Supraglottic Carcinoma (40%)
 T1—limited to 1 subsite of supraglottis; VF movement normal
T1—limited to 1 subsite of supraglottis; VF movement normal
 T2—>1 subsite of supraglottis/glottis/hypopharynx without fixation of larynx
T2—>1 subsite of supraglottis/glottis/hypopharynx without fixation of larynx
 T3—limited to larynx with vocal folds (VF) fixation and/or invades: postcricoid/pre-epiglottic/tongue base tissues
T3—limited to larynx with vocal folds (VF) fixation and/or invades: postcricoid/pre-epiglottic/tongue base tissues
 T4—invades through thyroid cartilage and/or invades into soft tissues of neck/thyroid/oesophagus
T4—invades through thyroid cartilage and/or invades into soft tissues of neck/thyroid/oesophagus
 Arytenoid
Arytenoid
 Aryepiglottic folds
Aryepiglottic folds
 False cords
False cords
 T1/T2: 16%
T1/T2: 16%
 T3/4 up to 62%
T3/4 up to 62%
43.4 Glottic Carcinoma (50%)
 T1—limited to VF (± ant./post. commissures) with normal mobility
T1—limited to VF (± ant./post. commissures) with normal mobility
 T2—extends to supraglottis and/or subglottis and/or with impaired VF mobility
T2—extends to supraglottis and/or subglottis and/or with impaired VF mobility
 T3—limited to larynx with VF fixation
T3—limited to larynx with VF fixation
 T4—invades through thyroid cartilage and/or extends to other tissues beyond the larynx
T4—invades through thyroid cartilage and/or extends to other tissues beyond the larynx
 Deep invasion with involvement of at least the thyroarytenoid muscle
Deep invasion with involvement of at least the thyroarytenoid muscle
 If posterior part of VF involved, fixation due to involvement of cricoarytenoid joint/cricoid cartilage/arytenoid
If posterior part of VF involved, fixation due to involvement of cricoarytenoid joint/cricoid cartilage/arytenoid
 Perineural invasion of recurrent laryngeal nerve
Perineural invasion of recurrent laryngeal nerve
 <10% T1/2
<10% T1/2
 10–37% T3/4
10–37% T3/4
43.5 Subglottic Carcinoma (5%)
 T1—limited to subglottis
T1—limited to subglottis
 T2—extends to VF(s) with normal or impaired mobility
T2—extends to VF(s) with normal or impaired mobility
 T3—limited to larynx with VF fixation
T3—limited to larynx with VF fixation
 T4—invades through thyroid/cricoid cartilage and/or extends to other tissues beyond larynx
T4—invades through thyroid/cricoid cartilage and/or extends to other tissues beyond larynx
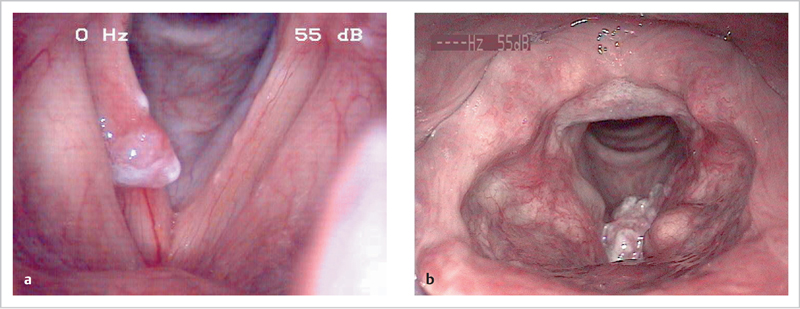
43.6 Overall Staging Grouping for Laryngeal Cancer
43.7 Unusual Tumours
 Consists of unusually well-differentiated keratinizing squamous epithelium arranged in compressed invaginating folds
Consists of unusually well-differentiated keratinizing squamous epithelium arranged in compressed invaginating folds
 Warty papillary surface
Warty papillary surface
 Clefts between adjacent capillary folds can be traced to depths of the tumour
Clefts between adjacent capillary folds can be traced to depths of the tumour
 Infiltration is on a broad base with pushing margins against a stroma containing a prominent inflammatory reaction
Infiltration is on a broad base with pushing margins against a stroma containing a prominent inflammatory reaction
 Usual cytological and infiltrating growth pattern of squamous carcinoma is absent
Usual cytological and infiltrating growth pattern of squamous carcinoma is absent
 Non-aggressive; seldom metastasizes
Non-aggressive; seldom metastasizes
43.8 Treatment of Laryngeal Carcinoma
43.8.1 Factors to Consider
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


