General Considerations
Malignant salivary gland neoplasms represent 3–4% of head and neck malignancies and <0.5% of all cancers diagnosed yearly in the United States, with an incidence of only 1–2 per 100,000 individuals. Unlike the more common mucosal head and neck cancers, which, in general, are attributed to excessive tobacco and alcohol use, specific carcinogenic factors for malignant salivary gland growths have not been as clearly identified. Viral infections, radiation, environmental exposure, and genetic factors have been hypothesized as causes. Malignant salivary gland tumors are classified by the World Health Organization as carcinomas, nonepithelial tumors, lymphomas, metastatic or secondary tumors, and unclassified tumors (Table 19–1).
| Carcinomas |
|
| Other Tumors |
| Sarcoma |
| Malignant Lymphomas |
| Secondary Tumors |
|
| Unclassified Tumors |
Only 20–25% of parotid gland neoplasms, approximately 45–50% of submandibular gland neoplasms, and > 70% of sublingual and minor salivary gland neoplasms are malignant. However, because 75–80% of salivary gland neoplasms are located in the parotid gland, this gland is still the most common salivary gland to be affected with a malignant neoplasm; a ratio of 40:10:1 is cited for malignant tumors of the parotid, submandibular, and sublingual glands, respectively.
Table 19–2 shows the histologic types of malignant salivary gland disease in order of frequency. The disease site also is important for predicting the histology. Mucoepidermoid carcinoma is most common in the parotid gland. Approximately half of malignant submandibular gland neoplasms are adenoid cystic carcinomas. Minor salivary gland malignant neoplasms are most often adenoid cystic carcinomas and adenocarcinomas. Prognosis varies according to histologic type, stage, and primary site.
| Histologic Type | Frequency of Occurrence (%) |
|---|---|
| Mucoepidermoid carcinoma | 34 |
| Adenoid cystic carcinoma | 22 |
| Adenocarcinoma | 18 |
| Malignant mixed tumor | 13 |
| Acinic cell carcinoma | 7 |
| Squamous cell carcinoma | 4 |
| Other | <3 |
Anatomy
The salivary gland unit is depicted in Figure 19–1. The acinus is located at the distal end of a salivary unit. It consists of pyramidal saliva-forming cells arranged around a central lumen, with myoepithelial cells interposed between the basal side of these cells and the basement membrane. Acinar cells may be serous, mucinous, or seromucinous, which explains the different chemical compositions of the saliva of each gland.
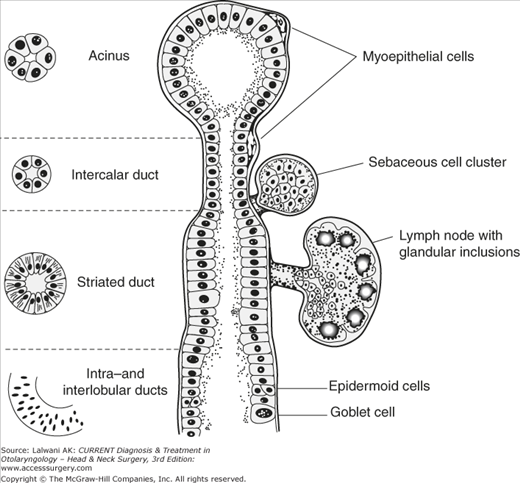
Serous cells predominate in the parotid glands. The submandibular glands have mixed populations of serous and mucinous acinar cells. The sublingual glands have mixed populations of mucinous and seromucinous cells. The minor salivary glands have mostly seromucinous cells. The acinus empties into an intercalated duct, composed of cuboidal cells similarly lined by myoepithelial cells between the basal side and the basal lamina. Intercalated ducts empty into striated ducts composed of columnar cells with fine striations. Lastly, the striated ducts empty into excretory ducts, which are composed of two layers of epithelial cells ranging in shape from cuboidal to squamous. Undifferentiated reserve cells associated with the intercalated ducts differentiate into acinar cells, intercalated duct cells, striated duct cells, and myoepithelial cells. Reserve cells associated with the excretory ducts give rise to excretory duct columnar and squamous cells.
Histologically, the salivary glands are arranged into lobules separated by connective tissue septa and encased in a connective tissue capsule; the salivary unit ducts converge in a treelike fashion into a central draining duct. Salivary gland lobules are made up of the acini, intercalated ducts, and small striated ducts. Larger striated ducts and excretory ducts are located within the connective tissue septa.
The major salivary glands are the paired parotid, submandibular, and sublingual glands. In addition, 600–1000 minor salivary glands are distributed throughout the rest of the upper aerodigestive tract.
The parotid gland is located anteroinferior to the ear, overlying the mandibular ramus and masseter muscle, extending medially between the mandibular ramus and the temporal bone to occupy the parapharyngeal space. The facial nerve travels through the substance of the parotid gland, dividing the gland into superficial and deep lobes, though this distinction is a convenience of surgical dissection and does not reflect an embryologic fusion plane or separate fascial layer. Malignant involvement of the facial nerve can result in facial weakness or paralysis and can provide an avenue for the intracranial extension of tumor. In addition, the facial nerve is at risk for injury during parotid surgery. The lymphatic drainage of the parotid gland is to both intraparotid and periparotid lymph nodes, and locally and regionally to the submandibular and deep jugular chain of nodes (levels I and II).
The submandibular glands are located in the submandibular triangle along with lymph nodes and branches of the facial artery and facial vein. The lingual, hypoglossal, and marginal mandibular nerves are all intimately associated with the submandibular gland. As with malignant disorders of the facial nerve and parotid gland, these nerves can be invaded by the cancer, resulting in paresis, paralysis, or numbness, as well as the intracranial extension of tumor. These nerves also are at risk for injury at the time of surgery. Submandibular gland lymphatics drain to the submandibular and deep jugular chain of nodes.
The sublingual glands are located deep in the anterior floor of mouth mucosa, adjacent to the submandibular glands. The sublingual gland lymphatics also drain to the submandibular and to the jugular chain of nodes.
Pathogenesis
The Reserve Cell Theory (currently favored) of salivary gland neoplasia states that salivary neoplasms arise from reserve (or stem) cells of the salivary duct system. The type of neoplasm depends on the stage of differentiation of the reserve cell at the time at which the neoplastic transformation occurs; it also depends on the type of reserve cell. The intercalated duct reserve cells give rise to adenoid cystic and acinic cell carcinoma. The excretory duct reserve cells give rise to mucoepidermoid, squamous cell, and salivary duct carcinoma.
The Multicellular Theory of salivary gland neoplasia states that salivary neoplasms arise from differentiated cells along the salivary gland unit. For example, squamous cell carcinoma arises from the excretory duct epithelium and acinic cell carcinoma arises from the acinar cells.
Staging
Table 19–3 lists the American Joint Committee on Cancer (AJCC) 2010 TNM (tumor, node, metastasis) Staging system used for malignant disorders of the major salivary glands. Malignant diseases of the minor salivary glands are staged according to the staging system for the primary site (oral cavity, pharynx, larynx, nasal cavity, and paranasal sinuses). T4 tumors are divided into moderately advanced (T4a) and very advanced (T4b) tumors, and, accordingly, Stage IV is divided into IVA, IVB, and IVC (distant metastases present).
| Stage | T | N | M |
|---|---|---|---|
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
| III | T3 | N0 | M0 |
| T1–3 | N1 | M0 | |
| IVA | T1–3 | N2 | M0 |
| T4a | N0–2 | M0 | |
| IVB | T4b | Any N | M0 |
| Any T | N3 | M0 | |
| IVC | Any T | Any N | M1 |
| TX | Primary tumor cannot be assessed | ||
| T0 | No evidence of primary tumor | ||
| T1 | Tumor ≤2 cm, no extraparenchymal extension | ||
| T2 | Tumor >2 cm, ≤4 cm, no extraparenchymal extension | ||
| T3 | Tumor >4 cm or extraparenchymal extension (or both) | ||
| T4a | Tumor invades skin, mandible, ear canal, facial nerve, or any of these structures | ||
| T4b | Tumor invades skull base or pterygoid plates, or encases carotid artery | ||
| NX | Regional lymph node cannot be assessed | ||
| N0 | No cervical lymph node metastasis | ||
| N1 | Single ipsilateral lymph node <3 cm | ||
| N2a | Single ipsilateral lymph node metastases >3 cm ≤6 cm | ||
| N2b | Multiple ipsilateral lymph node metastases, each ≤6 cm | ||
| N2c | Bilateral or contralateral lymph node metastases, each ≤6 cm | ||
| N3 | Single or multiple lymph node metastases >6 cm | ||
| MX | Distant metastasis cannot be assessed | ||
| M0 | No distant metastasis | ||
| M1 | Distant metastasis present |
Clinical Findings
Patients with malignant disease of the salivary glands most often present with an incidentally noted mass. Pain, facial nerve palsy (although lingual and hypoglossal nerves can be affected by submandibular and sublingual tumors), and cervical adenopathy portend locally advanced disease and a poor prognosis. In the parotid gland, the superficial lobe refers to the parotid tissue lateral to the facial nerve and encompasses about two thirds of the gland parenchyma; the deep lobe refers to that which is medial, although there is no embryologic fascial plane between these two locations. Parotid gland tumors involving the deep lobe can have parapharyngeal space extension and present as a symptomatic or asymptomatic (usual) oropharyngeal mass with no palpable external abnormality. In the submandibular triangle, it can be difficult to distinguish between a mass in the submandibular gland itself and an enlarged submandibular lymph node. Malignant disease of the minor salivary glands is often submucosal and can be located anywhere throughout the upper aerodigestive tract.



