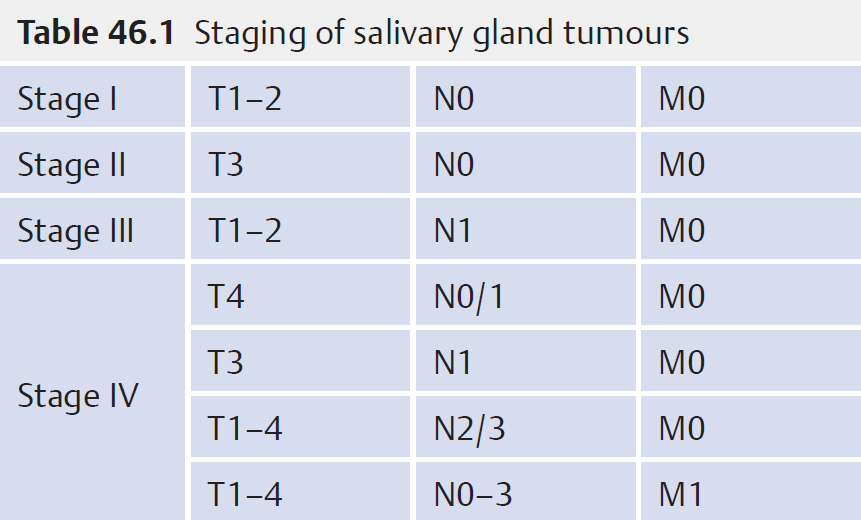
46 Major Salivary Gland Tumours • Pleomorphic adenoma—most common in parotid, 1% risk of malignant change per year after 10 years • Warthin (papillary cystadenoma lymphomatosum)—smoking risk factor, 10% bilateral, M:F 5:1 • Monomorphic adenoma—most common is basal cell adenoma • Oncocytomas—more common in elderly • 80% benign • Most common pleomorphic adenoma • Investigations – Pros—preop planning and patient counselling – Cons—most likely treatment is surgical so result does not change plans – Pros—deep lobe component can be identified, good for preop planning and counseling; lymph nodes not detected clinically may be identified therefore affecting treatment plan; infiltrative margins may raise possibility of malignancy – Cons—if no nodes palpable, unlikely to change treatment • 50% benign • Investigations – Pros—treatment planning – Cons—management of non-diagnostic samples; some laboratories require larger cellular volumes to diagnose lymphomas • 25% benign • Can occur within sinuses, nasal cavity, and larynx • Investigations • Epidemiology • Presentation • Mucoepidermoid carcinoma—most common malignant tumour, graded: low, medium, high • Adenoid cystic carcinoma—most common submandibular gland malignancy, increased risk perineural invasion, lung metastases more common than nodal • Acinic cell carcinoma—low-grade neoplasm, late recurrences even after 30 years • Adenocarcinoma—classified into low- and high-grade types • Squamous cell carcinoma—consider lymph node metastases from melanoma, skin • Carcinoma ex-pleomorphic adenoma—longstanding history of parotid swelling with rapid increase in size, aggressive, 5-year survival 40% • Salivary duct carcinoma—poor prognosis, 50% present with nodal metastases • Lymphoma—may require trucut biopsy to diagnose • See Table 46.1 • T1—≤2 cm • T2—2 to 4 cm • T3—extraparenchymal extension without VII n involvement and <6 cm • T4—invades skull base, VII n and/or >6 cm • Poorly differentiated carcinoma—23 to 26% • Adenoid cystic carcinoma—23 to 26% • Carcinoma ex-pleomorphic adenoma—9 to 14% • Acinic cell carcinoma 3% • Most common is surgery ± postoperative radiotherapy (PORT) • Operations include: – ± Excision skin with free flap or keystone repair – ± Neck dissection – ± Pinnectomy – ± Petrosectomy – ± Temporomandibular joint excision • Most common is surgery ± PORT • Dependent on site of tumour may require jaw split
46.1 Benign Tumours
46.2 Parotid Tumours
 Fine needle aspiration (FNA) ± US guided
Fine needle aspiration (FNA) ± US guided
 CT/MRI
CT/MRI
46.3 Submandibular Tumours
 FNA ± US guided
FNA ± US guided
46.4 Minor Salivary Gland Tumours
 Biopsy under local anaesthetic or general anaesthetic
Biopsy under local anaesthetic or general anaesthetic
 CT/MRI to evaluate the extent of tumour and nodal status
CT/MRI to evaluate the extent of tumour and nodal status
46.5 General Notes on Salivary Gland Malignancy
 1 to 2/100,000
1 to 2/100,000
 3 to 4% total head and neck malignancy
3 to 4% total head and neck malignancy
 25% parotid, 50% SM glands, 75% minor salivary glands
25% parotid, 50% SM glands, 75% minor salivary glands
 Risk factors include: RT exposure and occupational silica dust (blast furnaces, cement, glass, ceramic, and clay industries) and nitrosamine (rubber and tire industries)
Risk factors include: RT exposure and occupational silica dust (blast furnaces, cement, glass, ceramic, and clay industries) and nitrosamine (rubber and tire industries)
 Mucoepidermoid most common (inc. children)
Mucoepidermoid most common (inc. children)
 In children 65% tumours are benign, with haemangiomas being the most common
In children 65% tumours are benign, with haemangiomas being the most common
 Typically painless neck swelling
Typically painless neck swelling
 CN VII n weakness indicative of malignancy
CN VII n weakness indicative of malignancy
 Malignancy normally >6th decade
Malignancy normally >6th decade
 Benign tumours normally >4th decade
Benign tumours normally >4th decade
46.6 Malignant Tumours
46.6.1 Staging of Salivary Gland Malignancies
46.6.2 Presentation of Facial Nerve Paralysis in Malignant Tumours
46.6.3 Treatment for Parotid Malignancy
 Superficial parotidectomy + VII n preservation
Superficial parotidectomy + VII n preservation
 Total parotidectomy ± excision of VII n + grafting
Total parotidectomy ± excision of VII n + grafting
46.6.4 Treatment for Submandibular Malignancy
 Submandibular gland excision ± neck dissection
Submandibular gland excision ± neck dissection
46.6.5 Treatment for Minor Salivary Gland Malignancy
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


