Facal paralysis can lead to a variety of troubling symptoms for the patient, including ocular problems, speech difficulties, drooling, and nasal obstruction (Table 23-1). Facial paralysis can be devastating for patients because of the emotional impact from the facial disfigurement as well as difficulties with communication, eating, and drinking in a social setting. Numerous options are available for rehabilitation of prolonged facial paralysis (Table 23-2). The rehabilitation procedures can be divided into dynamic and nondynamic reanimation procedures; the latter include static slings, ocular protective procedures, and adjunctive cosmetic procedures. When assessing which procedure(s) to perform, one should not simply look at the problem as dynamic versus static reanimation of the entire face. Rather, it is best to approach the analysis by dividing the regions of the face to be reanimated into upper third, middle third, and lower lip and then to determine the functional deficits, cosmetic deformity in each region, and the patient’s desires. Furthermore, one must determine the feasibility of performing the procedures for achieving the desired goals.
Three basic questions need to be answered in the decision tree:
- What are the patient’s functional and aesthetic needs?
- What is the potential for spontaneous recovery?
- Is the patient medically fit to undergo a long operative procedure?
| Problems | Reasons |
| Eye irritation | Inadequate eye closure and corneal protection |
| Epiphora | Inability to effectively “pump” tears into the lacrimal drainage system |
| Visual-field defect | Ptosis of brow and soft tissues of the forehead |
| Speech difficulties | Lip incompetence, resulting in difficulty pronouncing consonents such as P and B |
| Drooling and difficulties eating/drinking | Lip incompetence and frequent biting on buccal mucosa, which protrudes into the oral cavity |
| Nasal obstruction | Collapse of nasal alar rim from flattened nasolabial fold |
* In addition to lack of facial motion.
Figure 23-1 presents a suggested algorithm based on the answer to these questions. This logical and rational approach to facial analysis for rehabilitation of the paralyzed face takes into consideration the aesthetic units that need to be restored, specific functional deficits and patient’s desires, duration of paralysis, patient’s medical condition, and the status of the distal facial nerve fibers and motor end plates.
Rehabilitation of the Upper Third of the Face
The main problems to be addressed in this region are improvement of eye closure and correction of laxity of the lower eyelid. Although dynamic muscle procedures have been described to restore eyelid function, most surgeons today rehabilitate the eye with static procedures because they are simple and effective. Inadequate eye closure can be improved by placement of a gold weight in the upper eyelid or insertion of an eyelid spring. Most surgeons prefer gold weight insertion over springs because the procedure is simple and easier to perform. The disadvantage of gold weight is that it requires gravity on the weight of the gold to pull the eyelid down and thus does not work effectively when the patient is supine. The advantage of a spring over gold weight is that its function is not dependent on gravity; therefore, it automatically protects the cornea during sleep. However, it is much more complicated and difficult to place a spring, and the potential for complications is greater. Paralytic ectropion of the lower lid can be corrected by performing wedge excision of the lateral lower eyelid and lateral canthopexy. Severe paralytic ectropion may also require medial canthopexy. The second, and often overlooked, problem in the upper third of the face is ptosis of the eyebrow, which aside from the obvious asymmetry may result in obstruction of peripheral vision due to lateral hooding. Brow ptosis is corrected with a forehead and brow lift, which can be performed through a forehead incision if the patient has a prominent wrinkle; otherwise, it can be performed endoscopically or through a coronal incision.
Rehabilitation of the Middle Third of the Face
Management options for correction of the mid-face disfigurement are much more varied, as shown in Figure 23-1. They range from simple procedures to restore symmetry at rest, such as a static sling or face lift, to complex dynamic rehabilitation with microneurovascular free flaps. Selection of procedure(s)for this region depends on both the patient’s desires and underlying medical condition as well as the potential for spontaneous recovery.
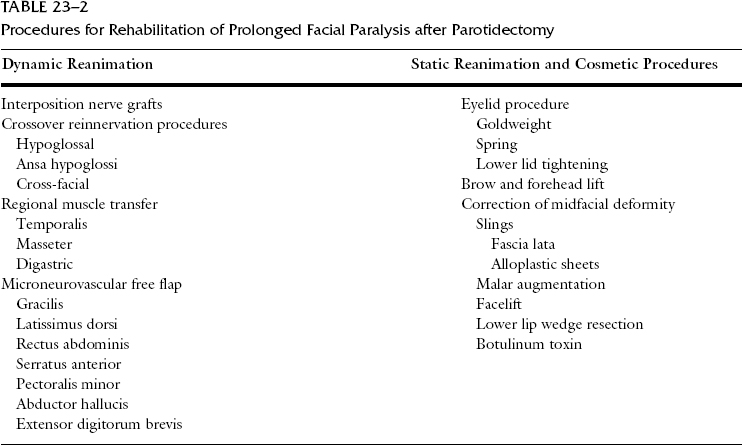
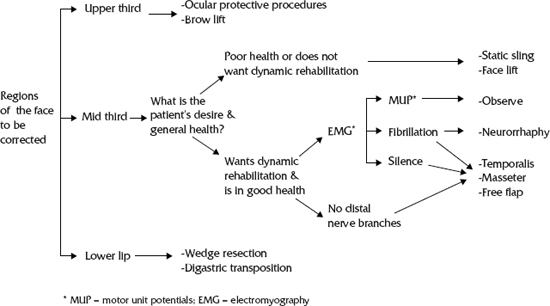
Figure 23-1 Rehabilitation of chronic facial paralysis.
When the facial paralysis is deemed permanent, such as when the facial nerve was not grafted at the time of resection(i.e., radical parotidectomy, acoustic neuroma surgery), any of the static or dynamic procedures listed in Table 23-2 can be offered to the patient at any time. By contrast, if the facial paralysis is thought to be a result of contusion such as after temporal bone fracture, or of surgery such as mastoidectomy, acoustic neuroma surgery, or parotidectomy, where the surgeon is confident that the nerve was left intact, reinnervation procedures should be delayed. The patient should be allowed to recover for approximately 1 year; reanimation procedures for the mid-face can then be considered if the patient does not demonstrate any clinical evidence of reinnervation. Selection of the rehabilitation procedure depends on the availability of the distal nerve fibers, associated soft tissue defect, the patient–s desires, and the operative risks. The algorithm in Figure 23-1 outlines a proposed decision tree based on these factors. The next step in deciding what to offer the patient is to determine the patient–s goals or wishes and to assess the patient–s underlying medical problems. If the patient simply wants to restore facial symmetry at rest to improve speech and mastication functions, or is a very high operative risk, static procedures such as an alloplastic sling or face lift under local anesthesia would be most appropriate. By contrast, if the patient is in fairly good health and would also like to restore facial motion, dynamic reanimation procedures should be offered. The choice of the dynamic procedure depends on the status of the distal facial nerve fibers and motor endplates. If distal facial nerve fibers are available for neurorrhaphy, reinnervation can be achieved with neurorrhaphy procedures such as interposition grafts or crossover reinnervation. Before performing these neural reanastomosis procedures, the status of the motor endplates should be evaluated with electromyography (EMG) of the facial musculature. Spontaneous recovery is expected if the EMG demonstrates polyphasic motor unit potentials; neurorrhaphy procedures should not be performed. Fibrillation potentials on EMG indicate persistent denervation, in which case neurorrhaphy procedures are appropriate. Lack of electrical activity on EMG implies that the motor endplates are no longer viable due to longstanding denervation, indicating that neurorrhaphy procedures are not likely to be successful. If the distal nerve fibers are not available for neurorrhaphy, or EMG shows electrical silence, innervated muscle flaps such as temporalis transposition, masseter transposition, or gracilis free flap are required for dynamic rehabilitation.
Neural Reinnervation Procedures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


