Chapter 62 Local Anesthesia for Thyroid and Parathyroid Surgery
Regional Anesthesia for Thyroid Surgery
Anesthesia for thyroid surgery was first described in 1849 by the St. Petersburg surgeon Nicolai Pirogoff, who used ether-based general anesthesia to facilitate removal of a large goiter causing tracheal compression in a 17-year-old girl.1 Prior to this seminal operation, indescribable patient suffering during thyroid surgery was the norm and, as a result, precise thyroid resections under controlled conditions were not feasible. The application of general anesthesia to thyroid surgery provided surgeons with physical and temporal control of their operations, thus allowing complete anatomic definition and exposure of the thyroid gland. The consequent dramatic refinement in surgical technique, combined with an evolving understanding of antisepsis, resulted in a marked improvement in operative mortality, which declined from 41% in 1850 to approximately 10% in 1910.2
Having clearly improved surgical outcomes, general anesthesia for thyroid surgery remained standard until the early 1900s, when Emil Theodor Kocher, having suffered the death of a patient during a thyroidectomy he was performing under general anesthesia, began popularizing cocaine-based local anesthetics for thyroid surgery.2 Nonetheless, general anesthesia gradually gained favor as anesthetic techniques were progressively refined and, up until the mid-1980s, the majority of thyroid surgeries were performed using general anesthesia.
With the subsequent blossoming of interest in minimally invasive techniques, high-volume endocrine surgery centers began reexploring local and regional anesthesia as a means of minimizing operative and hospitalization times associated with thyroid surgery. This resulted in resurgence of regional anesthesia for thyroid surgery, with associated improvement in selected operative and postoperative outcomes. Actual total hospital costs associated with general anesthesia for both total thyroidectomy and thyroid lobectomy were shown to exceed those of regional anesthesia by 30% to 56%.3–5 The duration of postoperative care monitoring represented the most significant component of this disparity, with the postoperative care unit monitoring time among general anesthesia patients exceeding that of patients managed under regional anesthesia by up to 95%.6
Postoperative pain control was also shown to improve with the use of regional anesthesia in patients undergoing total thyroidectomy or thyroid lobectomy. The incidence of moderate to severe pain in these cases was reduced by up to 26% in some series.7–9 Moreover, this effect was found to be independent of the timing of nerve block administration, being observed both when the block was performed prior to incision and after gland excision in patients receiving general anesthesia. Endotracheal intubation has been linked to postoperative pharyngitis and, although no formal studies comparing the incidence of postoperative throat pain among patients undergoing regional versus general anesthesia during thyroid surgery have been reported, the avoidance of endotracheal intubation during regional anesthesia for thyroid surgery likely minimizes postoperative throat pain.10 Numerous studies have associated regional anesthesia using propofol sedation with a reduction in postoperative nausea and vomiting, relative to isoflurane and sevoflurane-based general anesthesia. This disparity appears to be particularly significant among female thyroid surgery patients.11–13 Finally, regional anesthesia allows for a real-time, direct assessment of voice quality, and thus recurrent laryngeal nerve (RLN) function, which may facilitate the intraoperative detection of RLN injuries (see Chapter 33, Surgical Anatomy and Monitoring of the Recurrent Laryngeal Nerve).14
Regional Anesthesia for Parathyroid Surgery
The first successful parathyroidectomy was performed by Dr. Felix Mandel in 1925.15 This groundbreaking operation was performed under local anesthesia and the patient, Albert J, initially experienced resolution of his hyperparathyroid symptoms. Nonetheless, as the study of parathyroid pathophysiology evolved to include an understanding of multigland disease, requiring bilateral surgical exploration, local anesthetic procedures for parathyroid surgery were abandoned in favor of safer and more practical general anesthesia techniques. General anesthesia for parathyroid surgery thus remained standard from the 1940s until the mid-1980s. Subsequently, advancement in parathyroid imaging, intraoperative parathyroid hormone (PTH) detection and intraoperative parathyroid gland localization allowed for improved identification of aberrant parathyroid tissue, and focused resection under regional anesthesia became feasible.16–18
When performed using regional anesthesia, this focused procedure, pioneered by Dr. Paul Logerfo and termed minimally invasive parathyroidectomy (MIP), has been shown to afford similar advantages to those seen following thyroid surgery under regional anesthesia. Operating room time, hospitalization duration, and postoperative pain are minimized.19 Regional anesthesia is also associated with less postoperative nausea following MIP.20 Finally, voice quality may be directly assessed intraoperatively in MIP patients receiving regional anesthesia, which can facilitate the detection of intraoperative RLN injuries.
Contraindications for Regional Anesthesia in Patients Undergoing Thyroid or Parathyroid Surgery
Despite the advantages associated with regional anesthesia, a subset of patients requiring parathyroid or thyroid surgery will be optimally managed using general anesthesia techniques (Table 62-1). Patients with known histories of adverse reactions to local anesthetics should receive general anesthesia. Because excessive movement may impair operative safety, patients incapable of following instructions are best managed under general anesthesia. Similarly, significant anxiety or claustrophobia that cannot be adequately controlled in an awake patient should mandate general anesthesia. General anesthesia is also most appropriate for patients unable to comfortably tolerate the physical positioning required for cervical surgery or in whom airway maintenance is in question. Preoperative anatomic features that are likely to necessitate extensive or otherwise time-consuming dissection/exploration are also best managed using general anesthesia and include multifocal or invasive disease, reoperative surgical fields, and multigland parathyroid involvement. Finally, all parathyroid and thyroid surgical patients for whom regional anesthesia is planned should be prepped and draped in such a manner so as to facilitate general anesthesia, as intraoperative events may ultimately favor conversion to general anesthetics.
Table 62-1 Relative Contraindications for Regional Anesthesia in Thyroid and Parathyroid Surgery
Regional Anesthesia for Parathyroid and Thyroid Surgery: Technique
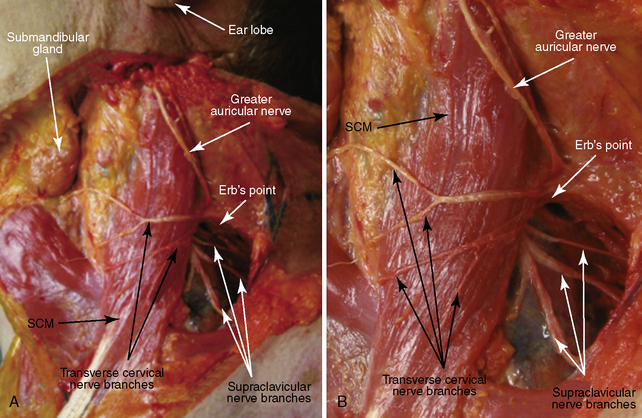
Sensory innervation to the lateral and anterior neck is supplied by the four major branches of the superficial cervical nerve plexus: the lesser occipital, greater auricular, transverse cervical, and supraclavicular nerves (Figure 62-1). These four exclusively sensory nerves exit the deep cervical space in close proximity to one another just posterior to the sternocleidomastoid muscle (SCM) at Erb’s point, approximately halfway along the length of the SCM. The lesser occipital nerve (not shown in Figure 62-1), arising from the C2 nerve root, angles sharply and superiorly from its origin, traveling just posterior and parallel to the SCM to supply sensation to the posterior neck below the occiput. The greater auricular nerve, deriving from cervical nerve roots C2 and C3, travels superiorly from its origin, superficial and parallel to the SCM, providing sensory innervation in the region of the superior SCM as well as the area immediately inferior and posterior to the ear. The transverse cervical nerve (derived from the C2 and C3 spinal nerve roots) courses anteriorly and perpendicular to the SCM, innervating the anterolateral neck. Finally, the supraclavicular nerve (a C3 and C4 cervical root derivative) branches near its origin, splaying out both anteriorly and posteriorly to innervate the lower posterior and anterior neck, the superior anterior shoulder, and the upper chest.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


