Lip cancer is one of the most common malignant tumors of the head and neck. The typical patient is a white male smoker with a fair complexion in his sixth to seventh decade of life who presents with a squamous cell carcinoma (SCCA) involving the lower lip. As the lips are in a prominent position on the face, appropriate management of this malignancy should have as its goals maximizing survival while minimizing the functional and cosmetic morbidity associated with treatment. This requires a thorough understanding of the functional anatomy of the lips, the biologic behavior of the disease, treatment options, and reconstructive considerations.
FUNCTIONAL ANATOMY
The lips form the anterior boundary of the oral cavity and function as a mobile oral sphincter that prevents dribbling of fluids and assists in mastication, deglutition, and articulation. The lips are also important aesthetically, contributing to appearance and facial expression. The anatomic extent of the lips includes only the vermilion, or that portion of the lip mucosa that contacts the opposing lip. Anteriorly, the lip ends at the vermilion border, which is the junction of the vermilion with the skin. The lower lip vermilion in repose is more everted than the upper lip. The transverse length of the upper lip is slightly longer: about 8.0 cm compared with 7.5 cm for the lower lip.
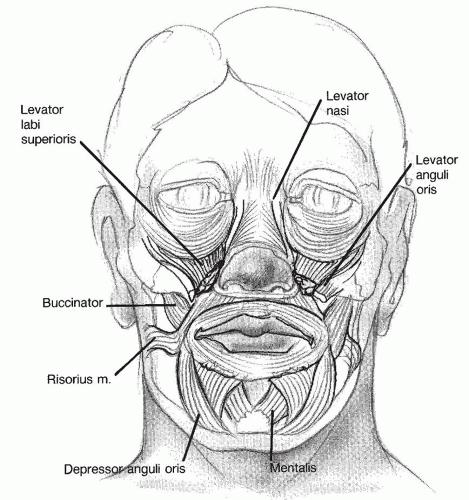
The orbicularis oris muscle is the sphincter that lies within the lip and encircles the oral aperture. Superiorly, it extends almost to the columella and attaches to the anterior nasal spine. Inferiorly, it interdigitates with the mentalis muscles to form the mental crease. Numerous paired muscles of facial expression insert on its lateral deep surface and contribute to oral competence and the diversity of lip movement (Fig. 116.1). The deep surface of the orbicularis oris is covered by loosely attached mucous membranes containing numerous minor salivary glands. Superficially, it is loosely attached to overlying skin.
The sensory and motor innervations of the lips are separate. The infraorbital branch of the maxillary division of the trigeminal nerve (V2) provides the major sensory supply to the skin and mucous membrane of the upper lip. The oral commissure area is supplied by the buccal branch of the mandibular division of the trigeminal nerve (V3), whereas sensation of the lower lip skin and mucosa is derived from the mental branch of the mandibular division. The seventh cranial nerve (facial nerve) provides the motor innervation of the lip. The upper lip musculature is supplied by the buccal branch of the facial nerve, whereas the marginal mandibular branch innervates the lower lip musculature.
The main blood supply to the lips consists of the superior and inferior labial arteries, which travel between the submucosa of the lip and the orbicularis at the level of the vermilion cutaneous junction. The vessels branch from the facial artery just lateral to the oral commissure. These paired vessels create a circumoral vascular arcade that provides the anatomic basis for the classic lip-switch procedures and other local myocutaneous flaps. Efforts should therefore be made to preserve the facial vessels when performing concomitant neck dissections. The arteries have accompanying veins that drain to the anterior facial veins.
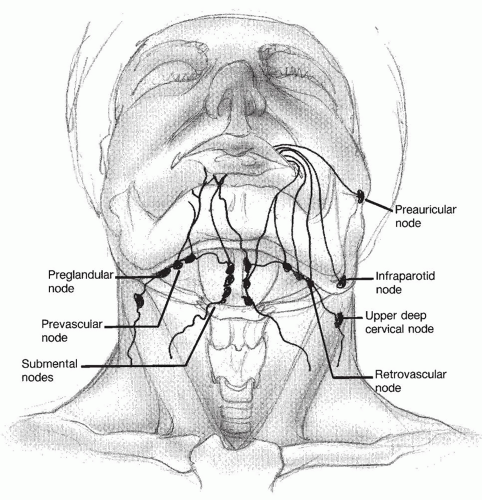
The lymphatics of the lips (Fig. 116.2) begin as a fine capillary network in the vermilion border and combine to form collecting trunks. The trunks from the upper lip and commissure drain first to the ipsilateral preauricular, infraparotid, submandibular, and submental lymph nodes. No contralateral drainage occurs because the embryonic fusion plane of the central frontonasal process separates the lateral maxillary processes and their associated neurovascular and lymphatic connections. The lower lip lymphatics drain first to the submental and submandibular nodes. Because the mandibular processes fuse in the midline, numerous anastomoses cross the midline to drain bilaterally. Lower lip lymphatics also enter the mental foramen in 22% of patients. The second nodal station for both upper and lower lips is the upper deep jugular nodes (level II) or occasionally the middle deep jugular nodes (level III).
Figure 116.1 Musculature of the lips. The orbicularis oris muscle is the sphincter lying within the lip and encircles the oral aperture. Numerous paired muscles of facial expression insert on its lateral deep surface to contribute to oral competence and the diversity of lip movement.
Figure 116.2 Lymphatic drainage of the lips. Lymphatic channels of the upper lip and commissure drain to the ipsilateral preauricular, infraparotid, submandibular, and submental lymph nodes. The lower lip lymphatics drain to both ipsilateral and contralateral submental and submandibular lymph nodes. The second nodal station for both lips is the upper deep jugular nodes and occasionally the middle deep jugular nodes.
BIOLOGIC BEHAVIOR
The age-standardized rate (ASR) of lip cancer varies according to gender, race, and geography. Around the world, lip cancer rates are highest in white males (1). In the United States, the ASR for white males is 2.5/100,000 per year compared to 0.3/100,000 per year for white females (2). South Australia has the highest ASR of lip cancer in the world: over 15/100,000 per year in men and 4/100,000 per year in women (3). Lip cancer is rare in Asia and in blacks (1,4,5). In the United States, for example, the ASR for both black males and females is 0.1/100,000 per year (2). The most common type of lip cancer is SCCA that is usually found on the lower lip in men. Basal cell carcinoma (BCCA) is the second most common malignancy and is found most frequently on the upper lip in women (6,7). Most cancers are found in individuals in their sixth to seventh decade of life (6,7,8).
The etiology is multifactorial and includes prolonged exposure to ultraviolet radiation, use of tobacco, consumption of alcohol, poor dental hygiene, and low socioeconomic status (6,7,8,9). Actinic cheilitis, or actinic keratosis of the lip, is considered to be a premalignant condition that doubles the risk of lip SCCA (10,11). Immunosuppression also significantly increases the risk of lip cancer as evidenced by higher rates in organ transplant patients. Unfortunately, both SCCA and BCCA arising in this setting are more aggressive in their behavior. Interestingly, failure of a transplanted kidney with its attendant cessation of immunosuppression decreases the risk of lip cancer to baseline (12).
Lip cancer is one of the most readily curable malignancies of the head and neck. When diagnosed at an early stage, 10-year cause-specific survival is as high as 98%, with a recurrence-free survival of 92.5% (13). The prominent location of the lips typically allows for early detection and treatment of this lesion. Characteristically, a history of crusting that bleeds on removal and a nonhealing blister for several months to years has been noted. When left untreated, the tumor progresses to involve skin of the mentum and alveolar mucosa. In advanced cases, mandibular bone, floor of the mouth, and tongue can be involved, which renders the patient an oral cripple. Metastasis to cervical nodes develops with advanced lesions, and ultimately distant metastasis occurs. In a retrospective study of 1,036 patients with lip cancer (14), multivariate analysis yielded several prognostic factors predictive for significantly decreased determinate survival: patients with primary tumors larger than 3 cm, presence of cervical metastasis, poorly differentiated or undifferentiated histology, and involved surgical margins. The risk of cervical metastases is increased in large primary tumors (greater than 3 cm), particularly if the oral commissure is involved; locally recurrent tumors; tumors thicker than 5 mm; poorly differentiated histology; or if perineural invasion is present (15,16,17,18).
CLINICAL EVALUATION
Lip carcinoma should be readily recognized and diagnosed (see Table 116.2). Its early stages can be indolent and protracted. As previously mentioned, the patient may present with a history of lower lip crusting that bleeds on removal or a nonhealing blister present for several months to years. Physical examination typically reveals an area of crusting with surrounding induration in an area of leukoplakia of the lower lip. In more advanced stages, a large bleeding mass may be present that can involve chin skin, the oral commissure, the upper lip, or the mandible. The integrity of the mental nerve must be evaluated even in early lesions, because tumor may track along the mental nerve and involve the mandible by direct extension, perineural invasion, or lymphatic spread into the mental foramen.
The diagnosis is established by incisional biopsy, which should include part of the deep or lateral tumor margin. This allows the pathologist to determine the pattern of invasion and the presence of perineural invasion. Prophylactic antibiotics are not necessary for simple biopsies (19). Ancillary radiographic studies such as a Panorex, computerized tomography (CT), and magnetic resonance imaging (MRI) are indicated when tumor is attached to the mandible or extends over the gingiva into a tooth root, when dentition is loose, or when hypesthesia of the mental nerve is present. Positron emission tomography (PET) resolution is too imprecise to correctly define the extent of the tumor compared to CT or MRI. Ipsilateral enlargement of the mental nerve foramen is a sign of mandibular invasion via the mental nerve, and obliteration of fat in the masticator space, in the pterygopalatine fossa, or along the mandibular canal must be regarded as suspicious for tumor spread, even in the absence of gross osteolytic changes (20). An aggressive metastatic workup is not indicated in previously untreated lip carcinomas, because fewer than 2% of patients have distant metastases at the time of initial evaluation (21). The staging of SCCA of the lip, as defined by the American Joint Committee on Cancer, is outlined in Table 116.1.
Although 90% of lower lip malignancies are SCCA (22), it is important to keep in mind the differential diagnosis of other nonhealing or ulcerative lesions of the lips, particularly when the clinical presentation is atypical for squamous cell cancer. BCCA is the second most common malignancy of the perioral region. Cancers of the upper lip are nearly always BCCA (6,14). It rarely arises on lip mucosa; rather, it involves the lip by direct extension of a perioral skin lesion. This is most commonly seen with sclerosing BCCAs. These tumors usually have a distinct clinical appearance of a pearly white nodule with central dimpling, although larger tumors may appear similar to squamous cell tumors. They grow very slowly, rarely metastasize to cervical lymph nodes, and when located near embryonic fusion planes tend to track deeply into the soft tissues along these planes.
TABLE 116.1 STAGING OF SCCA OF THE LIP: PRIMARY TUMOR (T)
TX
Primary tumor cannot be assessed.
T0
No evidence of primary tumor
Tis
Carcinoma in situ
T1
Tumor ≤2 cm in greatest dimension
T2
Tumor >2 cm but ≤4 cm in greatest dimension
T3
Tumor >4 cm in greatest dimension
T4a
Moderately advanced local disease: Tumor invades through cortical bone, inferior alveolar nerve, floor of mouth, or skin of face (e.g., chin or nose).
T4b
Very advanced local disease: Tumor invades masticator space, pterygoid plates, or skull base and/or encases internal carotid artery.
Overall, minor salivary gland tumors (MSGT) comprise less than 3% of all head and neck neoplasms, but the lips are the second most common site after the hard palate for the occurrence of MSGT (23). A neoplasm arising from the minor salivary glands typically presents as a smooth, firm, nonulcerated mass, very often involving the upper lip. However, when a MSGT presents on the lower lip, it is far more likely to be malignant. Overall, MSGT have about a 25/75 distribution between benign and malignant, but on the lip, they are more likely to be benign due to the great preponderance of pleomorphic adenomas. The most common malignant MSGT are mucoepidermoid and adenoid cystic carcinoma (23,24). Other rare malignant lesions of the lips include melanoma, microcystic adnexal carcinoma, Merkel cell carcinoma, malignant fibrous histiocytoma, and malignant granular cell tumors. Keratoacanthoma is a benign self-limiting epithelial neoplasm that can mimic SCCA. It is commonly seen in patients aged 60 to 80 years. It has an initial rapid growth phase (over several weeks) to 1 to 2 cm in diameter and then stabilizes and spontaneously regresses after several weeks to months. It occurs on the lips in 8.1% of cases, appearing as an ulcerated circumscribed lesion with elevated or rolled margins, a keratinized central region, and an indurated base. It is firm in consistency, and the central keratin core can desquamate, leaving an ulcer. Diagnosis is established by incisional biopsy, which is reported to accelerate its involution (25) (Table 116.2). Excisional biopsy, sparing as much normal tissue as possible, is indicated for persistent or enlarging lesions over several months, when SCCA cannot be excluded after previous incisional biopsies.
TABLE 116.2 DIAGNOSIS LIP CANCER
Diagnosis
Symptoms and Signs
Tests
Squamous cell cancer
Nonhealing blister or recurrent crusting, lip induration, ulcer or mass for months to years, mental nerve numbness
Panorex
CT/MRI
Biopsy
BCCA
Pearly nodule with central dimpling, upper lip, or perioral skin
Biopsy
Minor salivary gland tumor
Submucosal mass, usually upper lip
Biopsy
Keratoacanthoma
Rapid growth then spontaneous regression, may mimic SCCA in appearance
Incisional biopsy
CT, computed tomography; MRI, magnetic resonance imaging. From Baker SR, Krause CJ. Pedicled flaps in reconstruction of the lip. Facial Plast Surg 1983;1:68-69, with permission.
Again, a high index of suspicion for tumor should prompt a biopsy in the face of an abnormal physical exam of the lip. Common signs and symptoms of actinic cheilitis include dryness, atrophy, scaliness, swelling, erythema, ulceration, loss of distinction of the vermilion border, and the formation of transverse fissures (11). When any of these changes or leukoplakia or hyperkeratosis is seen, either as an isolated lesion or if the lesion progresses in size, biopsy is indicated. Other ulcerative inflammatory lesions involving the lips, including viral stomatitis and the primary chancre of syphilis, can mimic lip carcinoma but are acute in onset, and the lip lesion heals spontaneously.
MANAGEMENT
The most efficacious treatment modality for lip carcinoma is one that allows adequate treatment of the primary tumor, appropriate management of cervical lymph nodes, and successful reconstruction. The treatment plan should have the following goals:
Extirpate all tissue involved with cancer, both at the primary site and regional lymph nodes
Maintain oral competence in terms of speech, mastication, and retention of saliva
Maintain satisfactory lip cosmesis
Permit early rehabilitation and return to daily activities
Surgery and radiation therapy are equally effective in controlling T1, T2, and T3 lesions, while T4 lesions require combined modality treatment (26,27,28). In a series of 323 patients, of which 91% were T1 or Tcis treated primarily by surgery, cause-specific survival at 10 years was 98% (29). In a series of 158 stage I and II patients, 108 (68%) of whom were treated with surgery, and 50 (32%) of whom were treated with XRT; determinate survival rates were 95% for stage I and 90% for stage II without any difference between the treatment received (30). Another group reported on their 228 patients of whom 197 (86%) were treated only with surgery and 205 (90%) of whom were stage I and II. Their actuarial disease-specific survival for all stages was 92% at 5 years (22). A study of 256 stage I patients treated either with surgery (n = 90) or XRT (n = 166) found no difference between the two groups in local control or overall survival rates; however, disease-free survival rates were higher for those treated with surgery (31). A very large European study of 1,870 patients looking at the effectiveness of brachytherapy showed 5-year local control rates of 98% for T1, 97% for T2, and 90% for T3 lesions (27). In another set of 85 N0 patients treated primarily with XRT, the actuarial 5-year survival rate was 97% with a locoregional control rate of 93% in patients who had T1-T3 disease (26).
Patients with higher overall stages, and especially those with higher nodal stages, have a worse prognosis. In the series mentioned earlier with 5-year determinate survival rates of 95% for stage I and 90% for stage II, patients with stage III and IV lip cancers had a 37% 5-year determinate survival rate (30). In one series of 118 patients treated with surgery and post-op XRT as indicated, determinate 5-year survival rates were 100% for stage I, 94% for stage II, 67% for stage III, and 49% for stage IV. Not surprisingly, patients in stage IV also had the highest rate of recurrence (32).
Radiation therapy is a low-risk noninvasive technique that avoids the potential complications associated with general anesthesia and surgical morbidity (Table 116.3). However, the treatment time is prolonged (as much as 5 to 6 weeks for external beam XRT, 1 week for brachytherapy), a whistle deformity may result from tissue loss and wound contracture with very large tumors, osteoradionecrosis of the mandible may develop, and future reconstructive options may be limited. It is contraindicated as primary therapy in patients with definite bony involvement. Studies looking at the sequelae of XRT have found that the majority of patients have good aesthetic and functional outcomes, especially with smaller or intermediate tumors (26,27), but the great difficulty with XRT as primary therapy (especially for larger tumors) is that when complications occur, surgical reconstruction becomes more difficult. Primary radiation therapy may be most useful in the treatment of commissure lesions due to aesthetic and reconstructive considerations in this setting (27).
TABLE 116.3 COMPLICATIONS LIP CANCER
Surgical
Wound infection and dehiscence
Incompetent oral sphincter
Microstomia
Poor cosmetic result
Radiation
Whistle deformity
Osteoradionecrosis
In the United States, surgical management is recommended for most patients. The oncologic, functional, and cosmetic outcome is usually excellent in early T stage disease, and the oncologic outcome is poor with primary radiation of advanced tumors, particularly when it is close to or involves the mandible. We prefer a combination of surgery and postoperative radiotherapy for stage III disease with high-risk features, stage IV disease, and for recurrent disease after primary surgical treatment.
Vermilionectomy is indicated in Tcis, superficial carcinoma limited to mucosa, or multicentric or premalignant lesions such as actinic cheilitis (10). The standard approach to surgical resection of the primary lip lesion is full-thickness excision and careful intraoperative frozensection evaluation of the surgical margins. The appropriate margin around a T1 primary lip tumor is controversial. A study of 72 stage I and II patients reported a 2.8% local recurrence rate when a 3-mm margin of normal tissue was obtained and frozen-section margins were negative (33). When tumor margins were 2 mm or less, local recurrence was seen in 13% of patients, half of whom had received postoperative radiation therapy (34
Only gold members can continue reading. Log In or Register to continue
 DIAGNOSIS LIP CANCER
DIAGNOSIS LIP CANCER COMPLICATIONS LIP CANCER
COMPLICATIONS LIP CANCER


