Lens
Alex V. Levin
Thomas W. Wilson
David Rootman
The lens of the eye is derived from surface ectoderm, which invaginates into the optic vesicle during embryogenesis. This newly formed lens vesicle contains an outer capsule and is lined with primary lens epithelium. The posterior fibers elongate anteriorly to fill the vesicle. Secondary lens fibers emanate from the equatorial lens and migrate anteriorly and posteriorly to form the Y sutures. The primary lens fibers that are encircled by these secondary fibers are compacted to form the embryonic nucleus. The secondary fibers interior to the Y sutures make up the fetal nucleus. Additional fibers are laid down exterior to the Y sutures, forming the cortex. This complicated process is regulated by a variety of genes with differential expression in terms of location and time of development. The morphology of pediatric cataracts often reflects these stages of differentiation. Significant amblyopia and subsequent vision loss can occur from these opacities. Early surgery with optical correction is crucial for visual development.
Cataracts can be isolated genetic or nongenetic conditions or the result of systemic disease and systemic medications, in particular steroids. Cataracts may also be part of congenital syndromes. Heritable cataracts may be unilateral or bilateral. Attention must be paid to cataract morphology as this will provide information on cause, heritability, and management strategies. Some small cataracts may be managed medically, whereas more significant visual axis obstruction will require surgery.
The lens is suspended on the anterior vitreous face behind the pupil by the zonules (suspensory ligaments). A wide variety of systemic disorders, covered elsewhere in this atlas, may be associated with zonular weakness or dehiscence resulting in ectopia lentis. This chapter will focus on the causes of isolated ectopia lentis due to ocular malformation. Buphthalmos (Chapter 10: Glaucoma, Fig. 10.1) can also cause ectopia lentis. Isolated autosomal dominant and autosomal recessive forms may also be observed.
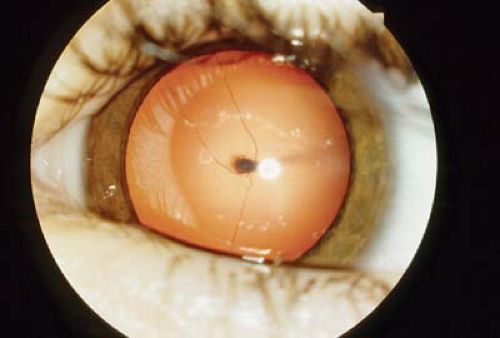 Figure 7.1 Mittendorf Dot Mittendorf dot is a small, gray or white opacity on the posterior capsule of the lens. It is the area where the hyaloid artery system attaches to the lens during ocular development. The opacity is not vision threatening and typically does not progress. A hyaloid remnant is seen here with some radiating persistent fetal circulation on the posterior surface of the lens. |
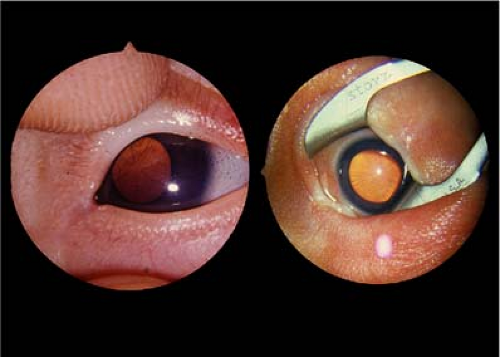 Figure 7.2 Tunica Vasculosa Lentis Tunica vasculosa lentis is the primitive vasculature that envelops the developing lens of the fetus as the forward extension of the hyaloid system. This fine network of vessels regresses starting at 28 to 30 weeks of gestation, but regression may be delayed by systemic illness. It clears centrally first and can be an accurate marker of gestational age. It is not visually significant. The left image is taken in a premature baby that is younger than the child on the right. |
 Figure 7.3 Anterior Subcapsular Cataract Anterior subcapsular cataract is an opacity that lies on the posterior surface of the anterior lens capsule. It is often traumatic in cause but may be an isolated heritable opacity or associated with Alport syndrome (often in the anterior lenticonus, not shown here) or atopic dermatitis. There may be a central focal white opacification of the anterior capsule, shown here, with the gray base of posterior subcapsular opacity. The latter may enlarge and become visually significant. However, if the opacity remains small (<3 mm), medical management with pharmacologic dilation of the pupil and patching of the other eye may result in good vision outcomes. |
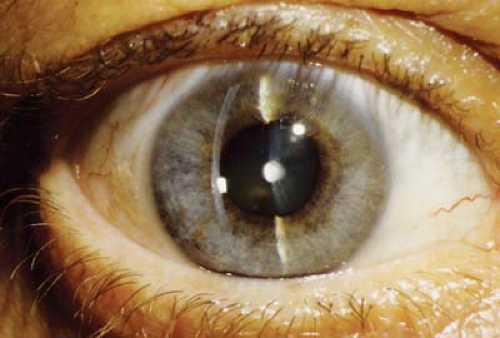 Figure 7.4 Anterior Dot Polar Cataract Anterior dot polar cataracts are small white opacities located centrally on the anterior lens capsule. Two thirds are unilateral. Although usually visually insignificant, other ocular findings may include amblyopia, anisometropia, persistent pupillary membrane, and strabismus. Progression is uncommon but patients should be examined at regular intervals, especially in the first year of life. Autosomal inheritance may be observed. |
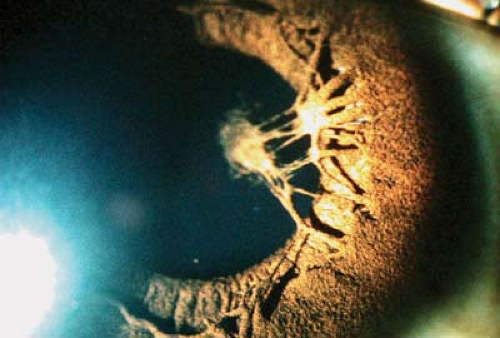 Figure 7.5 Anterior “Tractional” Cataract This lens opacity is always associated with a persistent pupillary membrane strand to which it is attached. This is a remnant of the neural crest–derived iris stroma network that covers the pupil during ocular development. The opacity in the lens capsule, with or without an underlying anterior subcapsular opacity, is usually eccentric to the visual axis and therefore visually insignificant. Enlargement of the subcapsular component is rare but follow-up is recommended, especially in the first year of life. The pupillary membrane strand often lyses spontaneously over time. This is a nongenetic unilateral lens opacity. |
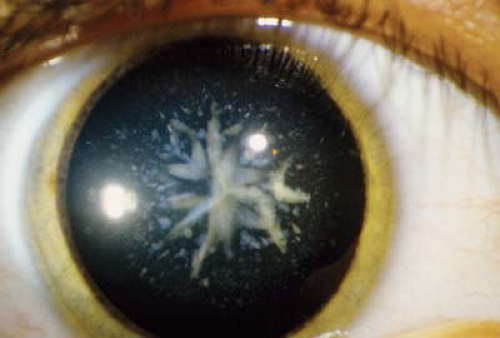 Figure 7.6 Cerulean Cataract Cerulean cataract, also known as “blue dot” cataract, may be an isolated heritable cataract or associated with systemic disorders such as Down syndrome. The multiple opacities appear as small, bluish-white amorphous dots located in the cortical material of the lens. More coalescence of the opacity may be seen in the nucleus, at the sutures, or in the posterior cortex. Crystallin gene mutations (CRYBB2, CRYGD) have been associated with autosomal dominant forms of cerulean cataract. |
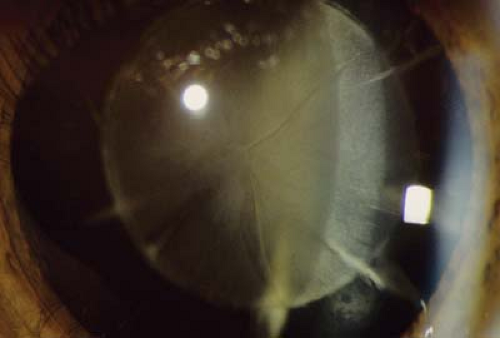 Figure 7.7 Lamellar Cataract
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|