16 Lasers in Laryngology LASER is an acronym for light amplification by the stimulated emission of radiation. •Light: Light beam has four fundamental characteristics, namely intensity, coherence, high collimation, and monochromaticity. Depending on the hydration, temperature, color, and thickness of the human tissue, lights of different wavelength are absorbed. •Amplification: The medium of laser has more stable than unstable atoms. During amplification this produces a tremendous source of energy. The electromagnetic emission released by stimulated emission is amplified by an external power source to produce an intense beam that will excite the atoms. The resultant excited state permits the emission of photons from the atoms. Thus, this creates a chain reaction in the laser. •Stimulated emission of radiation: Radiation emitted from a laser consists of a spectrum of wavelengths ranging from 200 (ultraviolet) to 10,000 nm (infrared). The most common types of lasers used in surgery are listed below with their corresponding wavelengths: ○500 nm: Argon laser ○532 nm: Potassium-titanyl-phosphate (KTP) laser ○585 nm: Dye laser ○1060 nm: Neodymium yttrium-aluminum-garnet (Nd-YAG) laser ○10,600 nm: Carbon dioxide (CO2) laser There are three components of surgical laser: 1.Active medium of laser 2.A power source to pump energy 3.Optical chamber Four possible interactions may occur when a laser beam makes a contact with tissue. A single reaction or multiple reactions may occur upon contact with tissue. 1.Reflection: The laser beam is neither absorbed nor does it pass through the tissue. 2.Transmission: The laser beam is not absorbed and it passes directly through the tissue. 3.Absorption: The laser beam is fully absorbed by the tissue. 4.Scatter/dispersion: The laser beam is partially absorbed, transmitted, and scattered by the tissue. Each type of laser has a specific mechanism by which it reacts with tissue in a specific way producing characteristic patterns of heat conduction, coagulation, ablation, and charring. Knowledge of laser physics and typical tissue interactions allows the surgeon to select the best laser for the respective pathology in the larynx. The CO2 laser produces a cone-shaped impact that has three characteristic levels from the center of impact to the outer layer; these are areas of charring, a region of tissue desiccation, and an outer layer of edema. Besides wavelength, laser tissue interaction depends on the mode of impact of the CO2 laser. The CO2 laser operates in either a continuous firing or pulsed mode. •Continuous mode: Photons are emitted in a constant and stable manner, enabling the stable delivery of energy and intensity. A constant power source to keep the active medium in an excited state, which is essential to maintain stimulated emission. •Repeat mode: An intermittent power source such as flash lamp is used to provide short bursts of energy to the active medium. A pulsed-mode laser delivers high energy in a very short time frame which produces deeper tissue cutting with less associated thermal damage. Lasers are named according to the lasing material within them that can be solid, gas, liquid, or semiconductors. NdYAG is a solid-state laser that has a yttrium-aluminum-garnet crystal acting as host for neodymium ions. Gas lasers use either a single gas or a combination of gases. The CO2, argon, and krypton lasers are examples of gas-based lasers. Semiconductor lasers have two layers of a semiconducting medium. Though they are of a low power, they provide sufficient power for clinical use. The diode laser is an example of a semiconductor laser. The CO2 laser was the first laser to be used in otolaryngology and remains the workhorse laser to this day.1 It can be used for incision, excision, and vaporization of tissue. It was first used in laryngology by Strong and Jako.2 Its wavelength of 10.6 μm is best suited for absorption by water. This characteristic is of importance because absorption of this wavelength into soft tissue (90% water content) will concentrate the energy, permitting little heat to dissipate to adjacent tissues. The laser light is transformed within the tissue to thermal energy, raising the tissue temperature to 100°C and hence vaporizes the tissue’s water content. This wavelength makes the CO2 laser a precise cutting tool, ideal for excision of small lesions located on delicate structures, such as the vocal cords. It also gives depth of penetration with minimal damage to adjacent tissue. The rapid thermal drop of laser energy in the tissue surrounding an incision results in shallow and predictable tissue penetration with minimal edema. It has good hemostatic capability, but this is limited to blood vessels not larger than capillaries (0.5 mm). Its beam can be focused to create a precise cut and also defocused to coagulate small blood vessels. A traditional CO2 laser has the disadvantage that it cannot be transmitted through flexible fibers but requires an articulated mirror system though the newer ones can deliver CO2 laser by a flexible fiberoptic cable. The Nd:YAG laser has a wavelength of 1.06 μm that is poorly absorbed by water, and, therefore, penetrates tissue deeply. The energy is not dissipated at the surface but scatters within the tissue dependent on the degree of tissue pigmentation. The Nd:YAG laser can be transmitted through flexible fibers, thus it can be used in the tracheobronchial tree. The wavelength is well absorbed by pigmented and vascular tissue, which along with its deep penetration into most tissues gives it good coagulation properties. Care must be taken while using the Nd:YAG laser to apply it to tissues in brief exposures of 1 second or less at a power setting below 50 W. Continuous application of this laser at high power settings may result in explosion of the tissue caused by the concentration of high energy below the tissue surface causing an expanding cavity. The thermal effect of the Nd:YAG laser goes beyond its immediate area of visible impact. The diode laser is a semiconductor laser. It is a sturdy and compact laser that requires minimal maintenance. The energy is transmitted through an optical fiber and can be used in contact mode and noncontact mode. The 532-nm KTP and 585-nm pulse dye laser are both hemoangiolytic lasers which are best absorbed by oxyhemoglobin. Due to this property, these fiber delivery laser systems are useful in vascular lesions such as papillomas and dysplasias. Both these lasers are noncontact laser systems. They can be used via the working channel of the flexible bronchoscope as an office procedure. Clinical Pearls •All clinicians using lasers must undergo laser safety training. •Each department using lasers must have a named laser protection supervisor. •The laser unit must remain switched off and locked with an identifiable key when not in use. •Lasers must be used in an appropriate theater, with clear notification when in use and an audible alarm if the notification is not heeded. •All personnel in theater must wear designated eye protection when the laser is in use. •When the laser is in use, but not actively firing, it must be kept in standby mode. •The surrounding tissues such as subglottic mucosa should be protected with wet cottonoid from inadvertent damage by the laser beam. •Wet swabs are placed over the eyes and around the field of use of the laser, for example, around the mouth and face. •A jug of water should be kept close by to quench an inadvertent airway fire. Laryngology is one of the specialty areas in which lasers are most often used. As a result of its precise cutting, superficial well-delineated effect with minimal lateral thermal damage, the CO2 is widely used in laryngology. The endoscopic use of the CO2 laser with a micromanipulator permits excellent precision and good hemostasis. This may not be possible with cold instruments. With the advancement of technology and a refinement of surgical techniques, good functional results have followed. The development of a microspot micromanipulator, as described by Shapshay et al, facilitated tissue excision with precise cutting and minimal damage to the surrounding mucosa and underlying vocalis muscle.3 The CO2 laser has been used to excise benign laryngeal lesions and is especially effective for excising vascular polyps, large sessile nodules, cysts, and the evacuation of polyps. The technique of excising benign laryngeal lesions by the CO2 laser is simple and is well described in the literature.4 The key to successful laryngoscopic excision is good exposure. A Kleinsasser anterior commissure laryngoscope with or without suspension system can be used for this purpose. Some benign conditions in which the laser may be used effectively are discussed below (Table 16.1). These are commonly located at the junction of anterior third and posterior two-thirds of the vocal cords which is the site of maximum mucosal vibration. These are generally superior to the free margin of vocal cords. Surgical excision with the CO2 laser scanning technology (Acublade, Lumenis, Israel) and the high-power pulsed mode (super or ultrapulse) in single pulse mode is the treatment for hard organized nodules (line of 1.5 mm, depth of incision of 200 μm—two passes, power of 10 to 12 W). Voice rest for 10 days followed by voice therapy is advised after excision. Table 16.1 Classification of Airway Lesions
Components of Surgical Laser
Laser and Interaction with Tissue
Lasers Used in Otolaryngology
Carbon Dioxide Laser
Neodymium:Yttrium-Aluminum-Garnet Laser
Diode Laser
Hemoangiolytic Lasers
Benign Lesions
Vocal Cord Nodules
| Congenital | Acquired |
Supraglottis | Laryngomalacia Vallecular cysts | Chemical trauma Vallecular cyst Epiglottic neoplasm Aryepiglottic fold cyst Ventricular fold fibrosis Laryngopharyngeal angioma |
Glottis | Glottic web | Glottic web: Anterior, midglottic, posterior |
| Bilateral vocal cord palsy | Neoplasm |
|
| Bilateral fixed vocal cord |
Subglottic and tracheal | Stenosis | Stenosis |
| Hemangioma | Granulomatous lesion |
|
| Hemangioma |
Cysts
A large variety of cystic lesions occur in the larynx. In the newborn it can form from an epithelial rest, in adults it may be a retention cyst of salivary gland and rarely can be associated with neoplasm. Intracordal cysts appear as small spheres on the margin of the vocal fold. The CO2 laser is a good tool for managing these lesions as achieving complete excision with cold instruments may be difficult.
The CO2 laser is a useful tool to surgically treat vocal fold cysts. It is important that cysts are completely excised to prevent any chance of recurrence. CO2 laser provides a better precision in dealing with such delicate lesion and the Acublade is a better alternative.5
Vocal Cord Polyps
These are pedunculated or broad-based lesions developing on the vocal fold. They present in a variety of shapes and sizes. Microsurgery and CO2 laser excision is, in the surgeon’s view, the appropriate treatment for the same. Fig. 16.1A, B shows the pre- and postoperative photographs of a vocal fold polyp excised using CO laser. Voice rest for 10 days after the surgery is advised, followed by a course of voice therapy.
Granuloma
These are benign lesions induced by healing granulomatous tissue secondarily epithelialized overlying the vocal process and medial aspect of arytenoids. If a granuloma persists, excision with a CO2 laser, especially the base of the granuloma, at low wattage with minimum lateral damage, should be the treatment. Recurrence is common while healing and many studies have shown a remarkable decrease in postoperative recurrence rates following injection of botulinum toxin in the thyroarytenoid muscle to prevent the slamming together of both the vocal processes, thus permitting perichondrial healing over the vocal process of the arytenoids.
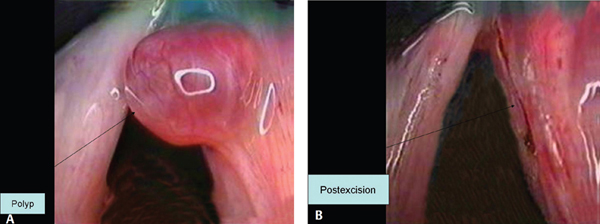
Figure 16.1 (A) Preoperative photograph of vocal fold polyp. (B) Postoperative photograph of vocal fold polyp following laser excision.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


