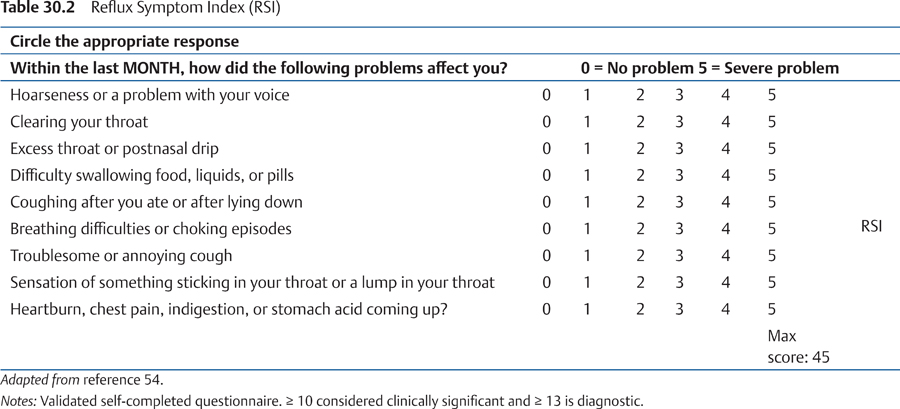
30 Laryngopharyngeal Reflux—Reflux beyond the Esophagus: Pathophysiology, Diagnosis, and Treatment Reflux of gastric contents not only causes the commonly presenting symptoms of heartburn and dyspepsia but is also responsible for a surprisingly wide range of extraesophageal symptoms and conditions. The reflux of gastric contents, including acid, pepsin, and bile, principally manifests as gastroesophageal reflux disease (GERD). However, reflux of gastric contents can also occur beyond the upper esophageal sphincter (UOS) and penetrate the upper aerodigestive tract. At this point, it can be responsible for a host of symptoms and conditions that are collectively known as atypical manifestations of GERD, also known as extraesophageal reflux (EOR) or laryngopharyngeal reflux (LPR). Awareness of EOR/LPR is relatively high within the ENT community and understanding of the condition is increasing within primary care.1 Gastroesophageal reflux (GOR) is a normal physiological phenomenon that occurs in most people, particularly after meals.2 This reflux, called physiological reflux, is characterized by a short duration of reflux episodes, infrequency during sleep, and lack of damage to the esophageal mucosa and does not normally cause symptoms.3 In contrast, GERD is a condition that develops when the reflux of stomach contents causes troublesome symptoms and/or complications. Exactly where GERD begins along the continuum, from physiological reflux at one end to complicated esophagitis at the other, may be problematic.4 According to the recent Montreal definition and classification of reflux disease, the manifestations of GERD are divided into esophageal and extraesophageal syndromes, with extraesophageal syndromes divided into established and proposed associations.5 The rationale for this terminology was that clinicians may need to define and classify patients based on differing amounts of information. GOR is very common. We all reflux and approximately 20% of the adult population has reflux symptoms at least once a week,6,7 with almost 10% of the adult population experiencing symptoms on a daily basis. Furthermore, it is estimated that up to 10% of patients visiting otolaryngology clinics have reflux-related disease and up to 55% of patients with hoarseness have reflux into the pharynx.8,9 Thus, reflux is considered one of the most important factors causing inflammation in the upper aerodigestive tract. In the literature, several different terms have been used to describe reflux that passes beyond the UOS. The term LPR was first introduced by Jamie Koufman in 19918 to describe the backflow of gastric contents that reaches pharyngeal and laryngeal areas. Subsequently, terms such as gastropharyngeal reflux, esophagopharyngeal reflux, and silent reflux have been used synonymously. All of these may be considered part of EOR, which is reflux anywhere beyond the UOS, including, for example, the sinus, oral cavity, and middle ear, the difference being that only symptoms or findings associated with the larynx and pharynx are considered when talking about LPR. Although the initial reports are from the beginning of the 20th century,10,11 the clinical importance of reflux for laryngeal lesions was first noticed in 1968 when Cherry and Margulies published their study on contact ulcer patients.12 In their study, reflux was diagnosed by barium swallow and cinefluoroscopy, methods that have since been superseded. Öhman et al13 reported the first series of laryngeal patients evaluated for reflux disease with modern diagnostic methods, that is, with esophageal manometry and 24-hour pH monitoring. Eventually, Wiener et al14 introduced the pioneering study on dual-probe pH monitoring, where the pharyngeal probe was “piggy-backed” onto the esophageal probe and positioned into the hypopharynx, enabling pH measurements to be taken in the upper aerodigestive tract. Since then, there have been several studies implicating acid injury as a contributing factor to upper and lower airway symptoms.15–18 GOR is necessary for LPR to occur, but not all episodes of GOR are associated with LPR. Owing to effective peristaltic motility and esophageal clearance mechanisms, salivary and esophageal gland secretions, as well as the tone of the UOS, the upper aerodigestive tract is well protected against reflux under physiological conditions.19,20 It has been speculated that the UOS function is defective in subjects with LPR. Some investigators have noted elevated UOS pressures in patients with reflux laryngitis, while others have found normal resting pressures. Shaker and his group21 have extensively studied the mechanisms of reflux above the UOS and found that it occurred in three different circumstances. A major mechanism of reflux into the pharynx was belching, which causes transient complete UOS relaxation, allowing gastric contents from the esophagus to reach the larynx and the pharynx. Additionally, spontaneous LPR could also be detected when the UOS pressure dropped transiently to approximately 10 to 25 mm Hg (low residual UOS pressure). Finally, when the esophagus contained residual acid in the supine position, swallowing could predispose to LPR. The results concerning esophageal motility in patients with LPR have been controversial. Some researchers have found ineffective peristaltic contractions with abnormal distal clearance times in patients with LPR, whereas others have found no significant difference in esophageal clearance times compared with patients with GERD. At least secondary peristalsis seems to be preserved in patients with posterior laryngitis (PL).22 Physiologically normal levels of GOR can lead to LPR in a subset of patients. In healthy individuals, these events would not be accompanied by classic symptoms of reflux, such as heartburn and regurgitation, and would therefore not be reported. It is the patient with LPR symptoms, in the absence of classic reflux symptoms, which makes the diagnosis sometimes counterintuitive and difficult to connect to the reflux of gastric content in the first place. The notion that reflux may be something other than a liquid bolus is a recent phenomenon and is still more theoretical than proven. It originates from the detection of acid in the pharynx and pepsin in the saliva as well as in the exhaled breath condensate of patients with suspected LPR. The presence of these substances (refluxate) in areas so distantly removed from the stomach is more conceivable if they were in an aerosol form rather than in a liquid bolus rising from the stomach. Refluxate as an aerosol has numerous implications. First, it more plausibly explains the occurrence of refluxate deep in the lungs23,24 and in the middle ear (in otitis media with effusion25 where bile acids have also been identified26). Second, liquid refluxate almost certainly has higher concentrations of acid and pepsin, but an aerosol would carry these injurious agents further into the upper aerodigestive tract. Third, their presence verifies that refluxate has reached these areas. When in excess and in the correct clinical circumstances, the findings are arguably diagnostic of LPR. Lastly, it highlights a key therapeutic need, namely the development of treatments to more successfully reduce pepsin in the refluxate. The esophageal defensive system preventing GOR will of course prevent LPR. The major elements of the antireflux mechanisms are the tone of the lower esophageal sphincter (LOS) and the diaphragm. The right crus of the diaphragm supports the LOS in its barrier function by physically encircling it and acting as a mechanical support, particularly during physical exercise.19 Four factors are known to contribute to esophageal luminal acid clearance; two of these, gravity and esophageal peristalsis, handle refluxate bolus clearance and, after effective bolus clearance, the other two, salivary and esophageal gland secretions, handle refluxate acid clearance.19 The third line of the defense mechanism consists of epithelial resistance. However, there are other “response mechanisms” that become activated after certain stimulation and may prevent reflux into the upper aerodigestive tract. According to Shaker and Hogan, distension of the esophagus or pressure stimulation of the pharyngeal wall may result either in fortification of the UOS barriers (esophago-UOS, pharyngo-UOS, and laryngo-UOS contractile reflexes) or closure of the glottis (esophagoglottal and pharyngoglottal closure reflexes).27 In addition, there are other reflexes included among the response mechanisms (such as pharyngeal swallow and secondary peristalsis induced by pharyngeal liquid stimulation and esophageal distension by refluxate) that result in pharyngeal and esophageal volume clearance. These further reduce the chance of refluxate contact with the tracheal, bronchial, and glottal structures. There are several theories for how reflux causes laryngeal pathology or pharyngeal and laryngeal symptoms. The microaspiration theory implies a direct acid–pepsin injury to the larynx and surrounding tissues.12 The stomach normally secretes acid at a pH of 1.5 to 2. This contrasts with the luminal pH of the pharynx and larynx, where pH is roughly neutral (pH 7).28 Consequently, pharyngeal pH decreases dramatically when LPR occurs. In addition to acidic pH levels, substances that can contribute to the noxious quality of the refluxate include pepsin, bile salts, pancreatic enzymes, bacteria, and bacterial products. Unlike the esophagus, the laryngeal structures are not rinsed with saliva, so small amounts of gastric contents are probably capable of producing injury to the respiratory epithelium. The microaspiration theory is supported by experimental studies, which show that minute amounts of acid and pepsin applied several times a week were capable of inducing subglottic lesions in dogs.8 Moreover, in vitro studies on laryngeal fibroblasts have shown that acid and pepsin together demonstrate considerable synergy, initiating the production of proteins involved in wound repair and angiogenesis.29 According to the trauma theory, the mere entry of gastric acid is not sufficient to produce or maintain injuries but that some additional factor is necessary for mucosal lesions to appear. This theory is supported by other animal studies, which found that the application of acid and pepsin was insufficient to break down the mucosal barrier on the vocal processes of the arytenoids.8 One may hypothesize that LPR only results in laryngeal injury as a result of comorbidity or when acting together with other risk factors for laryngitis, such as vocal abuse or concomitant viral infection.30 Finally, the esophageal–bronchial reflex theory suggests that acid in the distal esophagus stimulates vagally mediated reflexes, resulting in chronic repetitive throat clearing and coughing,31 which may lead to laryngeal symptoms and lesions. Furthermore, gastric contents in the pharynx irritate the mucosa locally, which may also alter laryngeal behavior. A combination of these mechanisms may be present in the same patient. Based on esophageal and laryngeal biopsies from patients with LPR compared with healthy individuals, Johnston et al made three key observations: pepsin adhered to epithelial cells, was endocytosed, and led to internal cell derangements.32–35 Pepsin was found on the surface of laryngeal epithelial cells in LPR patients but not in healthy individuals.32 The absence in healthy individuals is not surprising because significant reflux had previously been excluded by esophageal physiological measurements. In its active form, pepsin (a proteolytic enzyme) damages intercellular connective proteins and also intracellular proteins concerned with defense. Inactive pepsin is taken up within the cells by endocytosis via a competitive receptormediated mechanism and is apparent in vesicles situated in the Golgi system.33 This endocytosis is unanticipated as it seems unlikely that receptors specific for pepsin are present in laryngeal tissues. Apparently, such receptors provide some other function but when exposed to pepsin, they transport the enzyme into the cells. When cells were exposed to human pepsin 3B at pH 7.4, a level at which the enzyme is inactive, several major alterations happened, affecting the inner cell structure and function.34 The Golgi system has a pH of approximately 5.5 and together with its associated endosomes processes large molecules such as proteins and receptors through its mildly acidic environment. The supposition is that the changes result from reactivation of the inactive pepsin inside the cell. The cells distend and structural damage to the mitochondria and Golgi system became evident on electron microscopy within an hour, and damage was amplified by 12 hours. The early damage was accompanied by increased expression of seven genes concerned with cell stress and toxicity, including specific heat shock proteins. Late changes were accompanied by the diminished expression of 18 other stress genes. The evidence strongly argues for the following chain of events: inactive pepsin is endocytosed, is activated within the cells, and causes cell damage. This induces oxidative stress and the accumulation of free radicals, which damage mitochondria and may lead to cell death.36 In the assay used, the cells were only exposed once to pepsin, thereby modeling what might occur with a single episode of LPR. Although damaged, the cells were still viable at 12 hours, but with recurring exposure, as would be likely in persistent LPR, the damaged cells may not survive.34 The definition of pathological LPR is uncertain because pharyngeal reflux also occurs in healthy subjects and we are missing normative data from different age groups and do not know the impact of age on LPR. Esophageal symptoms and mucosal damage have traditionally been related to acid reflux episodes with pH less than 4.2,37 This limit is based on experimental studies that have shown a correlation between pain and the pH of infused material in the esophagus. Its clinical usefulness has also been verified in relation to the development of reflux esophagitis. Hence, the same limit of acid reflux has been applied to pharyngeal reflux disease. Pharyngeal reflux is typically quantified by counting the total number of events or by calculating the percentage time of acid exposure. Some consider even one single pharyngeal reflux episode abnormal,8 while others suggest that 4 to 18 acid exposure episodes to the pharynx may be normal.38,39 Nevertheless, simply counting the number of reflux episodes may be insufficient, owing to the varying duration of exposure. An average pharyngeal reflux episode in asymptomatic people lasts 6 seconds,40 whereas patients with PL have an average length of 30 seconds.15 In addition, according to Oelschlager et al,40 the longest pharyngeal acid exposure in healthy controls was 19 seconds, while exposure times as long as 16 minutes have been measured in PL patients.41 In recent meta-analyses, LPR events were demonstrated in 10 to 30% of asymptomatic normal adults,42,43 but acid exposure times (AETs) in normal subjects were very low (between 0.00 and 0.01%).42 It is nonetheless evident that there is an overlap in the occurrence of pharyngeal reflux between healthy controls and patients with LPR disease.43 One area of controversy is that pepsin has been shown to retain its activity at pH 5 to 6, suggesting that a threshold of pH 5 is also of importance when assessing the clinical presence of reflux.44 This pharyngeal, weak acidic reflux seems to be due mainly to regurgitation of more acidic material, which is then presumably buffered by saliva and secretions from the esophageal glands before reaching the hypopharynx. Another cause might be regurgitation of weakly acidic gastric contents. The frequent postprandial occurrence suggests this to be a combined effect of transient lower esophageal sphincter relaxation (TLESR) events triggered by gastric distension and the nonuniform intragastric buffering effect of food. Moreover, weakly acidic reflux may also be expected in patients treated with proton pump inhibitors (PPIs) since these drugs shift the gastric pH toward a less acidic mean value.45 Anderson et al have published normative data for pharyngeal reflux at pH 5.46 They found that pharyngeal pH 5 reflux episodes occurred in 91% of healthy controls with a median AET of 0.1%, and the upper limit of normality was 1.5%. Barium swallow is no longer routinely used to diagnose reflux disease, although it still has a significant function if structural changes, such as achalasia, are suspected. The Bernstein acid perfusion test has also fallen out of favor, but has been used recently in research into reflux-related cough. Upper gastrointestinal endoscopy is helpful in the identification of GERD but is regularly normal in patients with LPR. Esophageal manometry has not been routinely used in the diagnosis of LPR but is required to establish the position of UOS and LOS. This directs the accurate positioning and spacing of electrodes for pH monitoring and is valuable in the measurement of esophageal dysmotility, which may be contributing to symptoms. The 24-hour dual-channel pH monitoring, with electrodes placed at the distal esophagus and the UOS, has been the major basis for the diagnosis of LPR.47 Single-channel pH monitoring can help diagnose GERD but is not as useful in the diagnosis of LPR, as the damaging component may be aerosol or a nonacid composition. Many authors believe that any episode of reflux reaching the pharynx is abnormal, while others consider that more than four episodes in 24 hours are necessary to establish a diagnosis. More recently, multichannel intraluminal impedance measurement has been coupled with pH monitoring (MII-pH) and may improve diagnostic accuracy, particularly for weakly acidic or nonacidic reflux events.48 Both procedures are invasive, involving the transnasal insertion of a catheter, costly to carry out, and poorly tolerated by a large number of patients. The procedures require patients to reduce or stop their antireflux medication for a period of time preceding the investigations and therefore can result in an exacerbation of symptoms. However, for patients in whom surgery for LPR is indicated, physiological verification of the condition by pH monitoring or MII-pH is usually necessary. A noninvasive test that allows rapid results would be very helpful in patient management.49 One noninvasive procedure that has recently become available (Peptest, RD Biomed Limited, Hull, United Kingdom) uses a pepsin immunoassay applied within a lateral flow device for sampling pharyngeal secretions. If pepsin is detected, then the patient probably suffers from LPR.50 An additional minimally invasive procedure involves monitoring airway pH in the pharynx to detect aerosolized reflux (Restech, Respiratory Technology Corp., San Diego, California, United States).51 In ventilated patients, measurement of pH in exhaled breath condensate may also be helpful.52 One study has shown that in patients with cough related to LPR, which did not respond to standard medication, some patients were found to be positive for Helicobacter pylori and improved subsequent to eradication.53 Although compelling, it must be remembered that even though LPR is a potential cause of laryngopharyngeal inflammation, it is by no means the solitary cause. If there is any clinical suspicion whatsoever, then neoplasia must first be excluded. The diagnosis of LPR begins with the patient’s history. Symptoms reported to be related to LPR are tabulated in Table 30.1. The most common symptoms from the upper aerodigestive tract associated with LPR are hoarseness, globus sensation, throat clearing, and coughing.8,15,16 In addition, symptoms such as sore throat, laryngospasm, and choking sensation are related to LPR, but they are less studied. A diagnosis based purely on the history is challenging because all these symptoms are unspecific and common in several other laryngeal disorders. Belafsky et al54 developed the Reflux Symptom Index, a self-administered nine-item questionnaire to help categorize the severity of LPR (see Table 30.2). Heartburn and regurgitation, which are typical symptoms of GERD, are absent in 50% of patients with LPR15,55 for reasons previously described. The most frequent laryngeal finding associated with LPR is PL that occurs in up to 70% of LPR patients.8,15,17 It is characterized by edema or hypertrophy and sometimes erythema and hyperemia on the posterior aspect of the glottis. Sometimes the inflammation reaches up to the medial surface of the arytenoid cartilages. Some authors use the terms PL and reflux laryngitis interchangeably. However, reflux laryngitis encompasses wider changes in the mucosa, not only in the posterior glottis. Other changes often associated with LPR are vocal granuloma56 and pseudosulcus (subglottic edema producing a double-edged appearance).16 Of patients with pseudosulcus, 60 to 90% have LPR, while 65% of granuloma patients are LPR positive. The clinician must not forget that the most severe laryngeal diseases associated with reflux are laryngeal carcinoma and posterior glottic or subglottic stenosis. There is also some controversy regarding the sensitivity of the above-mentioned laryngeal findings. Some of this is certainly due to the problems with diagnostic tests in pharyngeal reflux. Despite these limitations, laryngoscopy continues to be an important tool in the evaluation of LPR. Moreover, a summary of these findings on fiberoptic examination of the larynx has been tabulated and ranked by Belafsky et al in the Reflux Finding Score (RFS) (see Table 30.3).57 However, the RFS has been criticized for its high levels of interobserver variability. Table 30.1 Symptoms Reported to Be Related to Laryngopharyngeal Reflux
History
Mechanisms of Laryngopharyngeal Reflux
Liquid, Gas, or Gas–Liquid Matrix?
Antireflux Mechanisms
Pathophysiology
Effect of Pepsin on Epithelial Cells
Investigations and Diagnosis
Symptoms
• Chronic cough • Chronic throat clearing • Excessive throat mucous • Chronic dysphonia/hoarseness • Intermittent dysphonia/hoarseness • Vocal fatigue • Globus • Voice breaks • Postnasal drip • Intermittent airway obstruction • Chronic airway obstruction • Wheezing |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


