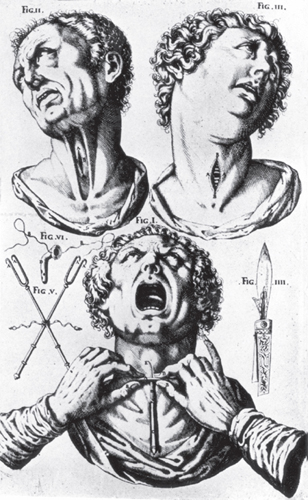
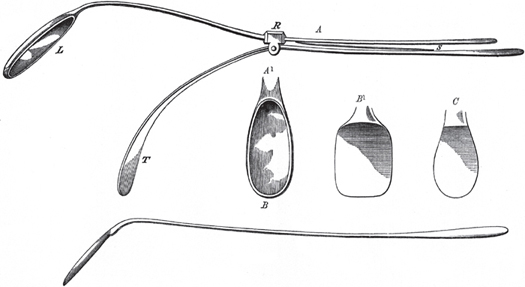
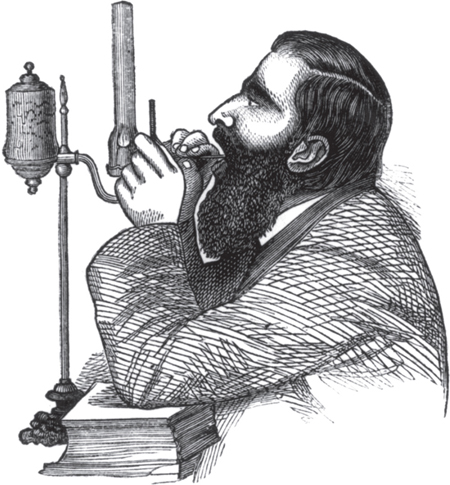
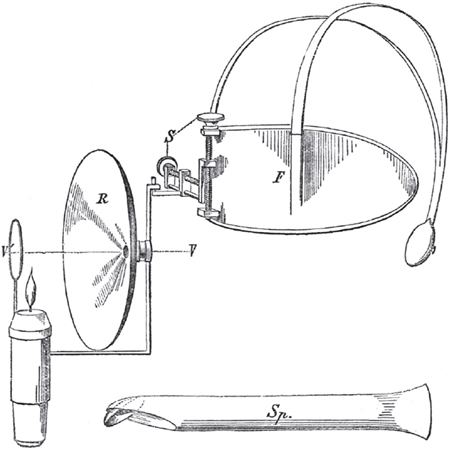
1 Laryngology—A Historical Perspective It is tempting to think that the specialty of laryngology was born with the invention of indirect laryngoscopy in the mid-1850s. This view, though, would not do justice to the understanding of the anatomy, physiology, and pathology of the larynx which had been accrued since the time of Hippocrates. By the mid-19th century, the management of throat diseases relied on intuition, extreme manual dexterity, and good fortune, as none of the practitioners were yet able to visualize lesions of the larynx despite many valiant attempts to do so. The stimulus given, however, to laryngology with the introduction of indirect laryngoscopy by Manuel Garcia in 1854 and its clinical application by Ludwig Türck in 1857 and Johann Czermak in 1858 was evidenced by the mass of literature on intralaryngeal lesions which abounded from the early 1860s. The application of the anesthetic and analgesic properties of cocaine to the mucous membrane of the pharynx and larynx demonstrated in 1884 by Edmund Jelinek and the replacement of the oxyhydrogen incandescent light by electric light invented in 1879 by Thomas Edison enabled mirror-guided surgical manipulation of the larynx to become commonplace. Laryngoscopy enabled visually controlled surgical intervention for airway obstruction secondary to infectious membranous laryngeal diseases, which were rife in the 19th and early 20th centuries, and transoral biopsy of laryngeal tumors. The unhappy case of the management of Crown Prince Frederick’s laryngeal cancer in the late 19th century, which in the earlier stages had necessitated repeated inconclusive biopsies, dissuaded many laryngologists and surgeons from performing biopsies of the larynx for fear of inducing infection, malignant transformation, or metastasis. Felix Semon in 1888–1889 demonstrated, in a large, elegant, and comparative series, that there was no significant difference in the development of cancer between a biopsied and a nonbiopsied group. Despite this work and the strong support for laryngeal biopsy from other leading laryngologists, these misconceptions continued well into the early 20th century. By this time, the technique of direct laryngoscopy promoted by Kirstein (1895), Killian (1898), Jackson (1907), and Brünings (1910) had become well established. Initially local anesthesia was used, but with the pioneering work on intubation by Ivan Magill (1921),1 there was a move toward the use of general endotracheal anesthesia with paralyzing agents. A greater understanding of the function of the larynx and voice production coupled with the use of the binocular operating microscope fitted with a 400-mm objective lens (Albrecht 1954, Kleinsasser 1962) opened the way to microlaryngoscopy, which enhanced the new discipline of phonosurgery, defined as any surgery designed primarily for the improvement or restoration of the voice. Although the term phonosurgery was first suggested by von Leden and Arnold in 1963, several functional procedures such as surgery for vocal fold paralysis had been described over 50 years before. Further improvements in lighting, produced by fiberoptic systems (Hopkins 1954, Hirschowitz 1958);2 magnification; stroboscopy (first invented by Oertel in 1878); and the introduction of lasers (light amplification by stimulated emission of radiation; Strong and Jako, 1972), together with new functional techniques aimed at altering the pitch, intensity, and quality of the voice, have advanced phonosurgery. Laryngeal malignant tumors have been traditionally treated by a combination of radical or conservative surgery, radiotherapy, and/or chemotherapy. The total removal of the larynx (laryngectomy), first performed for cancer by Theodor Billroth (1873), gave rise to a host of different voice reconstruction techniques from that of Gussenbauer (1874) to those of Singer and Blom (1980). The replacement of the whole larynx by transplantation was first performed by Paul Kluyskens in 1969, but the need for immune suppression presently precludes its use for laryngeal cancer patients postlaryngectomy. Techniques that use stem cell regeneration and are not reliant on immune suppression are showing early promise. In 1936, two slabs were discovered dating from the beginning of the first dynasty, one in Abydos relating to King Aha and the other, taken from the tomb of Hemaka at Saqqara, relating to King Dyer. Each slab depicts a seated person, presumably a physician, with a knife poised in an upheld arm in front of a patient whose head is extended backward. The signs above both operators and the heads of the patients indicate that life is being given from one to the other. Many scholars think this could be an illustration of an impending tracheotomy rather than a human sacrifice3 (Fig. 1.1). In the oldest known surgical treatise, the Edwin Smith Papyrus written ca. 1550 BC there is, in Case 28, a description of a crush injury to the neck which resulted in a pharyngeal fistula and loss of speech.4 Within the Corpus Hippocraticum or Hippocratic Collection, the writings of followers of Hippocrates (ca. 460–?377–359 BC), there is, apart from the epiglottis, no account of laryngeal anatomy, but the human voice is described as clear, hoarse, or shrill. Hippocrates speculated that the lungs and trachea played a role in voice production and that the lips and tongue were articulators.5 Aristotle (384–322 BC), recognizing that the cartilage tube in front of the neck was used for the passage of air, reasoned that the voice was produced within the trachea or windpipe by the impact of air against it—inspired by the soul that lay between the heart and the lungs (De Anima, II, viii). This observation has given rise to the expression that “the voice is the mirror of the soul.”6 Figure 1.1 King Dyer slab dating from the first dynasty depicting tracheotomy. Source: Pahor AL. Ear, nose and throat in Ancient Egypt. J Laryngol Otol 1992;106(9):773–779. Printed with permission. In India, various remedies for disorders of the voice were included in the medical knowledge compiled in the Sushruta Samhita (ca. 300 BC) and the Charaka (ca. 100 BC).7,8 From Greece, the seat of learning eventually passed to Alexandria where Herophilus (ca. 335–280 BC) and Erasistratus (ca. 350–250 BC) practiced as physicians and anatomists. Erasistratus by dissecting the human body studied the larynx and “trachea arteria” (to differentiate it from the adjacent “carotid arteria”) through which he believed air entered the lungs and then the heart, where it was changed into the “Vital Spirit” and then carried through the body by the arteries (the word “trachea” alone was not introduced until the 16th century). With the sacking of Alexandria, Greek medicine began to infiltrate Rome. The Roman period reached its climax with the appearance of a man whose teaching was to dominate medicine for the next 1200 years. Claudius Galen (ca. AD 129–200) regarded the body as the mere vehicle of the soul, a view which was warmly received by those of both Christian and Moslem faiths. Galen, in practice, followed the Hippocratic method and accepted the doctrine of the “humors.” His strength lay in his anatomical and physiological studies. The former had largely to be based on pigs and apes as the dissection of the human body had become illegal. It is said that his appointment as surgeon to the school of gladiators in Pergamon had given him an insight into the human anatomy. Thus by transferring his experimental discoveries to the human anatomy, he inevitably perpetuated many errors. Galen distinguished six pairs of intralaryngeal muscles and defined which ones opened and closed the larynx. Although he described three laryngeal cartilages (the thyroid, the cricoid, and the arytenoid), he assumed the arytenoid to be a single mass. Galen claimed to be the first to point out the ventricles of the larynx and reported the vocal folds as being of a membranous substance constituted so as to resist the impact of air and lubricated by mucus to prevent injury from vibrations of a dry surface. He taught that “the trachea-arteria prepares and prearranges the voice for the larynx … [The cartilages] increase it, and it is still further augmented by the vault of the throat, which acts like a sounding board” (De usu partium VII, 5).9 He demonstrated in pigs that section of the recurrent laryngeal nerve led to the loss of voice. Galen’s work was voluminous but many of his manuscripts, including those on the voice, were destroyed by fire. Galen did, however, cross-refer to these in other volumes. No one dared to dispute Galen, such was his authority, until the early 16th century, when Paracelsus (1493–1541) used to preface his lectures by burning Galen’s works and Andreas Vesalius (1514–1564), by dissecting the human body, disposed of many anatomical myths. With the awakening and renewal of culture implied in the Renaissance (late 14th century to 16th century) came an appreciation of the beauty of the human body. Those inspired artists, such as Michelangelo, Raphael, Dürer, and above all Leonardo da Vinci, turned to dissection of the human body. Despite correcting many of Galen’s anatomical errors, Vesalius in De Humanis Corporis Fabrica hesitated to confirm that the arytenoids were actually two cartilages and that there were two paired (internal and external) cricothyroid muscles.10 There was no doubt in the mind of Gabriel Fallopius (1523–1562) who confirmed that there were two arytenoid cartilages and only two complete cricothyroid muscles.11 Fabricius ab Acquapendente (1537–1619) in 1600 described branches of the recurrent laryngeal nerve and for the first time the thyrohyoid ligament.12 The knowledge of the anatomical structure of the larynx was completed by Giovanni Battista Morgagni (1682– 1771) who, in Epistolae Anatomicae (1740), noticed the oblique fibers of the thyroarytenoid muscle, described the ventricular folds (bands), and elaborated on the structure and function of the laryngeal ventricles which he observed acted as a reservoir of mucus for lubrication of the vocal folds.13 Morgagni demonstrated that the organ (in this case the larynx) is the site of disease, and with careful examination of the postmortem larynx he reported on a wide range of laryngeal pathologies including trauma from hanging, infections such as syphilis and small pox, and cancerous growths. The anatomist/physiologist Antoine Ferrein (1693–1769) of Paris was the first to make acoustic experiments on the natural larynx.14 He established that vibration of the vocal folds by a blast of air was the essential factor in the production of voice and that the intensity of the voice depended on the force of the blast of air. He proved that traction applied to the vocal folds produced variations in pitch and demonstrated the tensor function of the cricothyroid muscle. By likening the sound produced by the vibrating edge of the vocal folds to the effect of a bow on the strings of a violin (for which he originated the term vocal cords), he failed to appreciate the acoustic nature of the larynx as a reed instrument which was described later in 1806 by René Joachim Henri Dutrochet (1776–1847) who repeated Ferrein’s experiments. Coincidentally he and Jean Baptiste Biot (1774–1862), professor of physics at the Collège de France, determined that sound arose from a series of puffs of air caused by the reed (vocal folds) alternately opening and closing as a steam of air passed through them. François Magendie (1783–1855), professor of medicine at Paris, reinforced the previously held view that the concavities of the mouth and nose acted as resonators. By experimenting on dogs, he observed the protective sphincter mechanism of the larynx in swallowing. He believed that the muscles closing the glottis were supplied by the superior laryngeal nerves and the dilators by the recurrent laryngeal nerves.15 John Reid, professor of medicine at St Andrews, in 1838 showed conclusively that the internal branch of the superior laryngeal nerve supplies the larynx and the external branch supplies the cricothyroid muscle. All the remaining laryngeal muscles noted were activated by the recurrent (inferior) laryngeal nerve.16 During the late 18th and the early 19th centuries, the various kinds of ulceration of the larynx were differentiated. Hitherto the word “phthisis” was applied to almost any wasting condition and not specifically to tuberculosis of the lung or larynx. Because of the indecisive origin of “laryngeal phthisis,” the Academy of Medicine in Paris in 1836 offered a prize for the best essay on “The history of laryngeal phthisis.” It was won jointly by Armand Trousseau (1801–1867) and Hippolyte Belloc (1779–1853) with their essay “Traité Practique de la Phtisie Laryngée, de la Laryngite Chronique, et des Maladies de la Voix” (1837), in which they classified laryngeal phthisis into four types: (1) “simple” (severe or hypertrophic chronic laryngitis), (2) “syphilitic,” (3) “cancerous,” and (4) “tuberculous.”17 It was Karl Freiherr von Rokitansky (1804–1878), professor of pathology at Vienna, who in his Handbuch der Pathologschen Anatomie (1842) confirmed that laryngeal tuberculosis almost always follows lung tuberculosis.18 Dr. Francis Home (1719–1813) of Edinburgh, in An Enquiry into the Nature, Causes and Cure of the Croup (1765), was almost certainly describing diphtheria,19 but the term itself was not defined until 1826 when Pierre Fidèle Bretonneau (1778–1862) published Des Inflammations Spéciales du Tissu Muqueux et en Particulier de la Dipthérite, ou Inflammation Pelliculaire.20 The bacillus of diphtheria was discovered in 1883 by Edwin Klebs (1834–1913) of Zurich and was cultivated in the following year by Friedrich Loeffer (1852–1915). Horace Green (1802–1866) of New York is credited with the first attempt to remove a laryngeal growth (a pedunculated polyp) per viam naturales. He described a further eight cases in his book On the Surgical Treatment of Polypi of the Larynx and Oedema of the Glottis published in 1852.21 His innovative work on the direct treatment of laryngeal lesions in the prelaryngoscopic era was met with frank incredulity and savage attack. Eventually it was accepted that he was able to introduce instruments into the laryngeal inlet, but his more controversial treatment of lung disorders via the larynx was not accepted. Tracheotomy, or “laryngotomy” or “pharyngotomy” or “bronchotomy,” was a subject of much speculation from the time of Asclepiades of Bithynia (120–40 BC), who was the first to recommend incision of the windpipe (which he called laryngotomy)22 in cases of “angina,” to the great anatomist/surgeons of the late Renaissance. Antyllus (AD 3rd–4th century) recommended incision through the third and fourth rings of the trachea (which he called “pharyngotomy”) for relief of airway obstruction above the level of the larynx.23 Fabricius ab Acquapendente (1537–1619) extolled the advantages of the operation but criticized the transverse incision because of the potential danger of cutting the great blood vessels of the neck and because of the restricted view of the trachea. His pupil and successor Julius Casserius (1561–1616) published his De Vocis Auditusque Organis Historia Anatomicae (1600),24 which, apart from containing a wealth of comparative anatomy of the larynx, also illustrated the operation of tracheotomy with intubation with a curved silver tube (Figs. 1.2 and 1.3). Nicholas Habicot (1550–1624) performed four cases of “bronchotomy,” but the illustration in his short volume, with the long title Question Chirurgicale par Laquelle il est Démontré que le Chirurgien Doit Assurément Practiquer l’Opération de le Bronchotomie, vulgairement dicte Laryngotomie ou Perforation de la Fluste ou Tuyan du Poulmon, clearly showed a horizontal incision. The word “tracheotomy” had first appeared in Libri Chirurgiae XII, which was written in 1649 by Thomas Fienus (1567–1631), professor of medicine at Louvain, but its use was lost for nearly a century. It was reintroduced in later editions of Chirurgie (1743) by Lorenz Heister (1683–1758), professor of physic and surgery at the University of Helmstadt and fellow of the Royal Society, who unsuccessfully recommended abandoning other terms.25 Both Pierre Fidèle Bretonneau and Armand Trousseau used the term in relation to their work on diphtheria. Pierre Joseph Desault (1738–1795) clearly distinguished between “laryngotomy” and “bronchotomy.” He defined the former as cutting transversely through the cricothyroid membrane or vertically through the cricoid cartilage and the latter as cutting transversely between the rings of the trachea or vertically through them.26 For Desault it would seem that the terms bronchotomy and tracheotomy were still synonymous. In his important article “The story of tracheotomy,” published in the British Journal of Children’s Diseases in 1934, Goodall was able to find only 28 successful cases of tracheotomy recorded up to the time of Pierre Fidèle Bretonneau. The chief indications were acute inflammations of the pharynx and larynx and removal of foreign bodies.27 The earliest tracheotomy on a child was performed by Jean Charles Félix Caron (1745–1824) of Paris, who in 1776 removed an inhaled bean from a 7-year-old boy. Tracheotomy for children suffering from diphtheria did not become accepted until the mid-19th century, but interestingly a century earlier Dr. Francis Home had recommended the use of tracheotomy in cases of croup. Figure 1.3 The operation of tracheotomy, figures I–VI. Adapted from Casserius J. De Vocis Auditusque Organis Historia Anatomicae. Ferrara, Italy: Baldinus; 1600. The later part of the 19th century saw a huge increase in the numbers of tracheotomies performed. In 1884, Alois Monti (1839–1909) of Vienna perused the world literature and collected 12,736 cases of tracheotomy for diphtheria alone. By the end of the century, these figures had reduced significantly principally because of the discovery, in 1894, of diphtheria toxin by Emil von Behring (1854–1917). With the introduction of direct laryngoscopy and bronchoscopy, the need for tracheotomy in cases of foreign body inhalation diminished. But in the 1930s, a new indication for the operation was found in the treatment of removal of bronchial secretions in cases of bulbar poliomyelitis, myasthenia gravis, and tetanus. Tracheotomy, combined with positive pressure respiration in the management of poliomyelitis during the epidemics of the early 1950s, helped reduce the mortality from 80 to 40%.28 Prolonged use of polyvinyl chloride tubes with stiff cuffs tended to result in tracheal stenosis, but later soft cuffs solved this problem. Tracheotomy is still a life-saving operation, but in the emergency situation intubation or cricothyrotomy, if possible, is a preferable procedure. Many strides had been taken in the understanding of the anatomy and physiology of the larynx and the management of laryngeal diseases before the arrival of successful laryngoscopy in 1854. All the earlier workers shared a desire to see the glottis and many efforts were made. Philipp Bozzini (1773–1809), working in Frankfurt in 1807, invented his lichtleiter, which was a double cannula with two mirrors placed at 45 degrees at the end.29 Light from a wax candle was transmitted through one compartment and reflected onto the part to be examined. The image was received on the other mirror and reflected back to the eye through the second compartment. This instrument was used to inspect a variety of canals including the larynx. While it is doubtful whether Bozzini ever viewed the glottis, his concept of visualizing an interior organ using an external light source laid down the principle for all endoscopies. Benjamin Babington (1794–1866), a physician at Guy’s Hospital, London, presented his “glottiscope” (Fig. 1.4) to the Hunterian Society in 1829.30 It was a combined tongue depressor and oblong piece of mirror that was placed against the soft palate. Bright sunlight was required and the mirror needed to be dipped in water to prevent clouding by the patient’s breath. The epiglottis and the upper part of the larynx were visualized. A colleague at Guy’s, Thomas Hodgkin, coined the phrase “speculum laryngis or the laryngoscope.” John Avery (1807–1855), a surgeon at Charing Cross Hospital, London, came nearer than most to viewing the vocal folds. He used a head mirror illuminated by candlelight and a laryngeal mirror housed within a cumbersome speculum (Fig. 1.5). Avery never reported his work but after Garcia described his successful autolaryngoscopy in 1854 (reported on May 24, 1855, to the Royal Society on his behalf by the secretary and physiologist William Sharpey31), claims were made that Avery had anticipated his discovery in 1846.32 Manuel Patricio Rodriguez Garcia (1805–1906) of Spanish origin and a professor of singing at the Conservatoire de Paris and later at the Royal Academy of Music in London nursed one desire which was to see a “healthy glottis exposed in the very act of singing.” The inspiration for autolaryngoscopy came to him in 1854 while he was strolling in the gardens of the Palais Royal in Paris. He observed sunlight being reflected off window panes set in a quadrangle. He sought a hand mirror and a dental mirror. Having warmed the dental mirror and placed it against his uvula, he flashed a ray of sunlight onto this and to his excitement viewed his own glottis. His success was due to his own well-controlled capacious pharynx and his choice of a small simple mirror to introduce into his throat. Figure 1.4 Dr. Babington’s laryngeal mirrors. Adapted from Mackenzie M. The Use of the Laryngoscope in Diseases of the Throat. 3rd ed. London: Longmans, Green & Co.; 1871:14. Figure 1.5 Avery’s laryngoscope. Adapted from Mackenzie M. The Use of the Laryngoscope in Diseases of the Throat. 3rd ed. London: Longmans, Green & Co.; 1871:24. The first clinical application of indirect laryngoscopy was made by Ludwig Türck (1810–1868), a neurologist in Vienna. Initially unaware of Garcia’s discovery, he used small long-handled mirrors and sunlight to examine patients at the Allgemeine Krankenhaus in the summer of 1857. In the winter he put aside his mirrors and loaned them to Johann Czermak (1828–1873), a physician in Budapest. In a communication in April 1858, Türck stated that he was: “very far from having any exaggerated hopes about employment of the laryngeal mirror in practical medicine.”33 Johann Czermak modified Türck’s mirrors and developed his own technique of indirect laryngoscopy using a fenestrated head mirror and artificial light.34 He demonstrated this technique on himself (Fig. 1.6) and his patients throughout Europe and incurred the displeasure of Türck who claimed that he was the first to use the mirror for diagnostic purposes. The “Turckish War”, as the disagreement was called, successfully helped publicize laryngoscopy. In summary, it can be said that Manuel Garcia was the first to perform a successful mirror laryngoscopy, Johann Czermak developed and popularized the technique, and Ludwig Türck founded the specialty of laryngology. Figure 1.6 Autolaryngoscopy. The right hand holds the laryngeal mirror and the left hand holds the flat mirror, represented here in profile. Adapted from Czermak JN. On the Laryngoscope and Its Employment in Physiology and Medicine. Translated from French by Gibb GD. London: New Sydenham Society; 1861:18. The stimulus given to laryngology by the introduction of laryngoscopy is readily seen in the mass of literature on intralaryngeal lesions that abounded from the early 1860s. Georg Richard Lewin (1820–1896) in 1861 reported on 50 to 60 cases of laryngeal neoplasms, which represented only 5 or 6% of all cases of laryngeal disorders.35 He operated on his first case in July 1860 and used either cutting devices or caustics. Thomas J. Walker of Peterborough, England, reported a case to the Lancet in 1861 in which he described the removal of a polypoidal growth from the larynx of a 14-year-old boy using a twisted loop wire snare under laryngoscopic guidance.36 He had visited Vienna and had observed the technique of indirect laryngoscopy. He published The Laryngoscope and its Clinical Application in 1864.37 Carl Stoerk (1832–1899) became the first full-time lecturer in laryngology and rhinology in Vienna in 1864. He developed many laryngeal instruments and possessed a skillful technique, which enabled him to successfully operate on the larynx in the era before the discovery in 1884 of the application of cocaine as a local anesthetic by Edmund Jelinek (1852–1928) who worked in the Clinic of Laryngoscopy, founded in 1870 as the first of its kind in the world, at the Allgemeine Krankenhaus with Leopold Schrötter von Kristelli (1837–1908) as its head. Edmund Jelinek remarked on the high cost of cocaine at the end of his article entitled “Cocaine as an anesthesia and analgesia for the mucous membrane of the pharynx.”38 In the United States, Louis Elsberg (1837–1885) of New York had been influenced by Johann Czermak who had sent him his book On the Laryngoscope and Its Employment in Physiology and in Medicine published in German in 1859 and in English in 1861.39 Louis Elsberg published his essay “Laryngoscopal surgery, illustrated in the treatment of morbid growths within the larynx” in 1866 for which he was awarded the gold medal of the American Medical Association.40 Jacob da Silva Solis-Cohen (1838–1927) of Philadelphia reported on the intralaryngeal removal of polyps in 1867. Four years later, the number of published cases of laryngeal polyps had reached 189 to which Morell Mackenzie (1837–1892) of London added a further 100 cases of his own.41 In Paris, Charles Henri Fauvel (1830– 1885) reported a personal series of 100 cases in his book Traité Pratique des Maladies du Larynx (1876).42 Among these cases were ones of early vocal fold cancer. The principles for their removal were laid down by Bernhard Fraenkel (1836–1911) of Berlin, who in 1886 noted that early vocal fold cancer is likely to arise on the superior surface of the vocal fold, to be of small volume, to present with hoarseness, and to be amenable to transoral resection.43 In those cases where the tumor had extended anteriorly or posteriorly along the vocal fold or below the glottis, consideration was given to the much more risky operations of thyrotomy or laryngofissure. Quoted in Albers,44 the credit for the first thyrotomy or laryngofissure is normally given to Brauers of Louvain who performed the operation in 1833 without a preliminary tracheotomy to cauterize a papillomatous growth of the larynx.44 Laryngofissure was first performed in the United States in 1851 by Gordon Buck (1807–1876), who, 2 days before the operation, performed a tracheotomy,45 and in England in 1865 by Sir George Duncan Gibb (1821–1876) who used chloroform anesthesia.46 The operation was not a bounding success. Morell Mackenzie on the strength of 28 published cases concluded that: “Thyrotomy does not even affect such complete evulsion as laryngoscopic treatment.”47 Perhaps these remarks were tainted by the fact that, as a physician, he did not perform the external operation but entrusted it to a surgeon. From his observations, the space in which to operate was limited by the need for and the restrictions of retraction of the two halves of the larynx. In his view this made surgical removal of lesions of the larynx more difficult than via the transoral route for which he was an acknowledged master. Even the eminent surgeon Sir Henry Trentham Butlin (1843–1912) in 1883 was disenchanted: “The disease is evidently far too deeply seated to admit of removal by so slight an operation”.48 He worked closely with Felix Semon (1849–1921) who agreed that: “Thyrotomy yields very bad results in cases of malignant growths and should not be attempted”.49 Their view started to change at the end of the 19th century as their results improved with better patient selection.50 By 1930, Sir St Clair Thomson (1859–1943) was able to report only two operative deaths and a 76% 3-year survival rate in a series of 74 patients.51 The operation of total laryngectomy for cancer was one which was held in awe. The general surgeon Professor Theodor Billroth (1829–1894), head of the Second Surgical University Clinic at the Allgemeine Krankenhaus, Vienna, was presented with a 36-year-old theology teacher who had been found by the laryngologist Carl Stoerk to have a histologically proven left-sided subglottic epithelioma. Theodor Billroth (Fig. 1.7) elected to remove the tumor by laryngofissure after a preliminary tracheotomy. The tumor was excised with preservation of the right vocal fold. A month later, as the patient became increasingly breathless, the tracheotomy track was reopened and a cannula was inserted. At a further laryngofissure, it was found that the tumor had spread into the perichondrium of the thyroid cartilage. The anesthetic was lightened and the patient was woken to be told that a total laryngectomy was the only option open to him. He consented and Theodor Billroth removed the larynx above the third tracheal ring and below the epiglottis. He sutured the edges of the hypopharynx and the trachea to the skin. The open pharynx initially leaked liquid and food but gradually diminished in size such that more and more food went down the esophagus, and by 18 days he was able to swallow solid food. Theodor Billroth’s assistant Carl Gussenbauer (1842–1903), who reported the case, designed an “artificial larynx”, which was a T-shaped tube with one limb being placed in the trachea and the other passing through the fistula into the pharynx (Fig. 1.8). Both limbs had one-way valves such that the expiratory stream was forced into the pharynx but food did not enter the trachea.52 Figure 1.7 Theodore Billroth (1829–1894). From a hologravure of a drawing by Lenbach (1884).
Ancient History
The Roman Period
The Renaissance
Anatomy of the Larynx
Physiology of the Larynx
Pathology of the Larynx
The History of Tracheotomy
The Laryngoscope
Prelaryngoscopic Era
Postlaryngoscopic Era
Early Laryngeal Surgery after the Introduction of the Laryngoscope
Intralaryngeal Surgery
Thyrotomy or Laryngofissure
First Laryngectomy



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


