27 Laryngeal Trauma The larynx protects the airway from aspiration, acts as the respiratory gateway to the lungs, and is the primary organ of phonation.1 Laryngeal trauma can disrupt one or all of these function and, in the context of airway compromise, is acutely life-threatening.2–4 If not promptly recognized and adequately treated, it can also cause significant long-term morbidity.4–6 Laryngeal trauma often co-occurs with cervical and intracranial injuries and frequently forms part of polytrauma.4 It is therefore important that all patients with suspected laryngeal injury be managed by a multidisciplinary trauma team according to Advanced Trauma Life Support (ATLS) guidelines. Laryngeal trauma can be broadly divided into external trauma, which can be blunt or penetrating, and internal trauma, which can be caused by iatrogenic, thermal, caustic, or foreign body injuries. External laryngeal trauma has a population incidence of 1 in 137,000 in adults4 and accounts for 0.5% of trauma admissions in children.7 The larynx—which is superiorly, inferiorly, posteriorly, and laterally well protected by the mandible, sternum, the cervical spine, and strap muscles of the neck—is susceptible to crushing anterior cervical trauma. Rapid motor vehicle deceleration can thrust the neck against the steering wheel or dashboard if driving without a seat belt. Another important mechanism of injury is the clothesline injury, in which a rider encounters a fixed horizontal object at neck level. Suicidal or homicidal strangulations can also cause laryngeal trauma. Clothesline injuries are often associated with major neck trauma, which may not be initially apparent.8,9 Homicidal strangulation is more likely to cause laryngotracheal separation and neurovascular trauma when compared with suicidal strangulation.10 All strangulation injuries can cause loss of airway due to laryngeal edema some time after the event, despite minimal initial findings.11–13 Laryngeal injury can be confounded by the process of laryngeal calcification, which begins during the third decade of life and can lead to creation of stress risers leading to laryngeal comminution.14 Over the past decades, however, with improvements in public education, reductions in speed limits, and mandatory use of seat belts, the number of blunt laryngeal trauma cases has declined, and penetrating laryngeal trauma, which is due predominantly to interpersonal violence or war, has become the predominant form of laryngeal trauma.2,3,6,15–23 Penetrating trauma is more likely to damage additional cervical structures, with the extent of injury being proportional to both the weight and velocity of the penetrating projectile (E = ½ mv2). Clinical presentation of laryngeal trauma ranges from cardiopulmonary arrest due to airway obstruction to subtle changes in voice quality. The most common presenting feature of laryngeal trauma is hoarseness (85%), followed by dysphagia (52%), anterior cervical pain (42%), breathlessness (21%), and hemoptysis (18%).5 Examination and initial management of laryngeal trauma should follow ATLS guidelines to ensure that concomitant injuries are not missed (Table 27.1).4 The overriding priority is to establish a safe airway with cervical spine protection and this may, and often does, necessitate performing an emergent tracheotomy under local anesthesia. Endotracheal intubation is not favored in this situation, as it can exacerbate a laryngeal injury24 and precipitate total airway obstruction. If endotracheal intubation has been performed, it is converted at the earliest opportunity to a tracheotomy to prevent long-term laryngeal injury. No manipulation of the neck is permissible until the cervical spine has been cleared. Table 27.1 Concomitant Primary Diagnoses Recorded along with Laryngeal Trauma4
Mechanisms of Injury
External Laryngeal Trauma
Diagnosis
Management
Injury | (%) |
Open neck injury | 18 |
Maxillofacial fractures | 18 |
Intracranial injuries | 17 |
Cervical spine fracture | 13 |
Chest injury | 13 |
Other facial injury | 10 |
Skull fracture | 7 |
Open pharyngeal injury | 4 |
In our practice, multislice computed tomography (CT) (Fig. 27.1) is performed in all patients presenting with “impending airway obstruction” once the airway has been secured, and in those patients with a “stable airway” who are found, on flexible nasoendoscopy, to have endolaryngeal abnormalities, since imaging may reveal further laryngeal injuries and most importantly clear the cervical spine. This is particularly pertinent consideration, as up to 13% of patients with laryngeal trauma can have an associated cervical spine injury and that the spinal injury may be masked by the presence of a distracting laryngeal injury.4,25 CT scanning can be deferred only in those patients with unalarming history and minor physical findings. Laryngeal trauma can be classified according the Schaefer-Fuhrman24,26 (Table 27.2) or the Lee-Eliashar systems.27
Managing Laryngeal Trauma
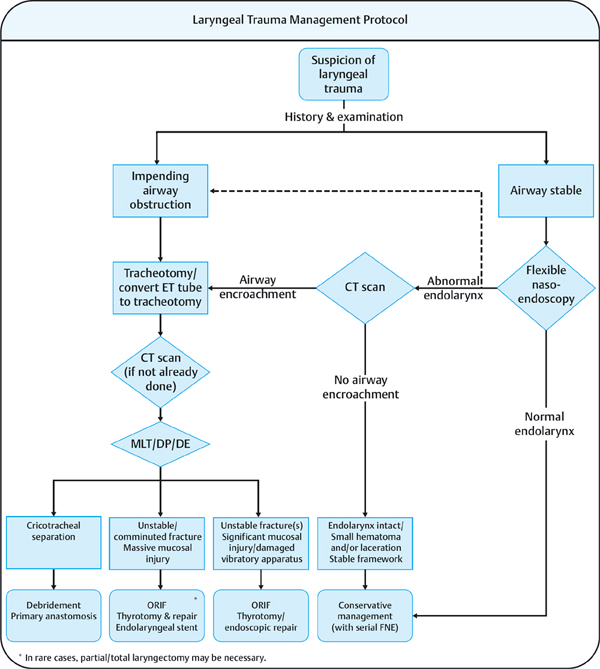
The first priority in managing laryngeal trauma is to assess and secure the airway while protecting the cervical spine. We take a stepwise approach to securing the airway based on information available at the different stages of clinical assessment (Fig. 27.2). A stridulous patient with respiratory distress at presentation should immediately proceed to have a tracheotomy under local anesthesia. If the airway is judged to be stable following initial history and examination, the patient has a flexible nasoendoscopy. In a small number of cases, unexpected airway-encroaching injuries are identified at this stage and the patient proceeds to have a tracheotomy. More subtle endolaryngeal injuries are further assessed with CT and again, if airway-encroaching injuries are identified, the patient proceeds to have a tracheotomy.
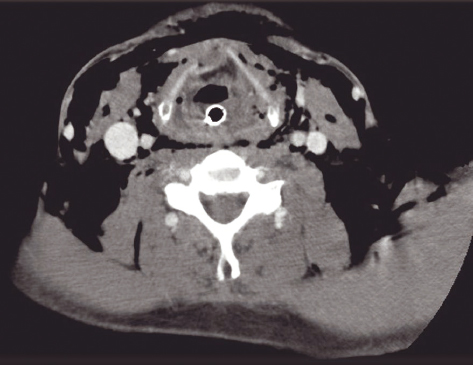
Figure 27.1 Computed tomographic appearance of a patient with acute external laryngeal trauma.
The decision on the most appropriate therapy for laryngeal trauma rests on assessing the stability of, and the extent of injury to, the laryngeal framework, the extent of mucosal injuries, the presence or otherwise of injury to the vibratory apparatus, and the integrity of the laryngotracheal junction. Jewett et al showed that 37% of patients with laryngeal trauma could be managed with no airway intervention and a further one-sixth of patients required only a tracheotomy.4
Table 27.2 Schaefer-Fuhrman Classification of Laryngeal Trauma
Group 1 | Minor endolaryngeal hematomas or lacerations No detectable fracture |
Group 2 | Edema, hematoma, minor mucosal disruption without exposed cartilage Nondisplaced fracture Varying degrees of airway compromise |
Group 3 | Massive edema, large mucosal lacerations, exposed cartilage Displaced fracture(s) Vocal cord immobility |
Group 4 | Same as Group 3 but more severe with: Severe mucosal disruption Disruption of the anterior commissure Unstable fracture, two or more fracture lines |
Group 5 | Complete laryngotracheal separation |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


