Laryngeal Trauma
Randall J. Jordan
Byron K. Norris
Scott P. Stringer
Laryngeal trauma is a relatively uncommon event requiring timely, proper management of injury to preserve the patient’s life, airway, and voice (1). Each case of external laryngeal trauma presents a unique set of problems, but despite the diversity of injuries, specific management guidelines can be applied. Adhering to such an approach assists in attaining the best possible outcome after blunt or penetrating external laryngeal trauma. Severity of injury and delay in treatment correlate with poor outcome.
PATHOPHYSIOLOGY OF LARYNGEAL INJURIES
Blunt Trauma
Blunt trauma to the larynx is caused mainly by motor vehicle accidents including all-terrain vehicles, personal assaults, or sports injuries. Although the mandible and sternum normally protect the larynx, the neck can be hyperextended during the trauma, which allows the laryngeal skeleton to be crushed between the impinging object and the cervical vertebral column. With a moderate blow to the larynx, the momentum of the vocal folds causes a shearing effect between the vocalis muscle and the internal perichondrium. This results in injuries such as endolaryngeal mucosal tears, edema, or hematoma. More severe trauma produces fractures of the laryngeal cartilages and disruption of the laryngeal ligaments.
Subluxation or dislocation of the arytenoid cartilage can produce an immobile vocal fold. Unilateral injury to the recurrent laryngeal nerve often is associated with cricoarytenoid joint injuries owing to the proximity of the recurrent laryngeal nerve to the cricoid cartilage. Fractures of the cricoid cartilage can occur alone or with other injuries, especially after lower cervical trauma. As the only complete ring of the airway, structural integrity of the cricoid cartilage is essential in airway maintenance.
The so-called clothesline injury that occurs in association with blunt laryngeal trauma deserves special attention because of its severity. This injury typically occurs when the neck of an individual (typically an adolescent or young adult) riding a motorcycle, all-terrain vehicle, or snowmobile strikes a stationary object such as a wire fence or tree limb. The transfer of such a large amount of force confined to a relatively small area of the neck crushes the laryngeal cartilages and commonly causes cricotracheal separation. The airway is held together precariously by the intervening mucous membrane and pretracheal fascial sleeves. Bilateral injury to the recurrent laryngeal nerve often is associated with cricotracheal separation.
Associated structures also can be injured during blunt cervical trauma. Fractures of the hyoid bone and associated epiglottic injuries can cause airway obstruction. The greater or lesser cornu of the thyroid cartilage can lacerate the pharyngeal mucosa as it is pressed against the cervical vertebrae. Sex and age differences among adults have been hypothesized as leading to different types of injuries after blunt trauma. Women are considered more likely to incur supraglottic injuries than are men because they have long, thin necks. Elderly persons have been described as being at higher risk of sustaining comminuted laryngeal fractures than are younger adults because older persons have increased ossification of the laryngeal cartilage. Neither of these hypotheses has been verified with clinical observation (2).
Blunt trauma tends to affect the larynx of a child differently from that of an adult. The larynx in children is situated higher in the neck and is better protected by the mandible than it is in adults (3). While laryngeal fractures are less common in children, the incidence is increasing paralleling the incidence of motor vehicle collisions (4). Pediatric injuries tend to be less severe than adults due to the elasticity of the pediatric cartilaginous skeleton; however, the lack of extensive fibrous tissue support and the
relatively loose attachments of the mucous membranes increase the likelihood of soft tissue damage in children, and may account for the poorer prognosis of those with more severe injuries (5, 6). Additionally, relatively innocuous trauma may precipitate airway distress secondary to the small laryngotracheal diameter in children (6). Several cases of membranous rupture of the pediatric trachea due to seemingly minor blunt cervical injury have also been reported (7).
relatively loose attachments of the mucous membranes increase the likelihood of soft tissue damage in children, and may account for the poorer prognosis of those with more severe injuries (5, 6). Additionally, relatively innocuous trauma may precipitate airway distress secondary to the small laryngotracheal diameter in children (6). Several cases of membranous rupture of the pediatric trachea due to seemingly minor blunt cervical injury have also been reported (7).
Manual strangulation or hanging-type injuries produce different patterns of laryngeal injury because the applied force is fairly static and of low velocity. This can cause multiple cartilaginous fractures without immediate mucosal laceration, submucosal hematoma, or marked displacement of the fractures (8).
Penetrating Trauma
Knife and gunshot wounds are primarily responsible for penetrating trauma. Injuries vary from minor lacerations to severe disruption of the cartilage, mucosa, soft tissue, nerves, and adjacent structures. Gunshot wounds are more likely than knife wounds to be associated with severe tissue damage, and high-velocity projectiles cause greater tissue destruction and wound contamination than low-velocity projectiles (9). Knife wounds cause less peripheral soft tissue damage than gunshot wounds and are cleaner, but it is difficult to determine depth of penetration. Injuries to deep structures, such as the thoracic duct, cervical nerves, great vessels, and viscera, can occur well away from the entrance wound. Death from penetrating trauma may be caused by complete disruption of the larynx, massive soft tissue edema, or associated neurovascular injuries. Most injuries to civilians from penetrating trauma tend to be limited to the path of the missile because they are caused by lower-velocity bullets or stabbing (9).
DIAGNOSIS AND EVALUATION
History
Any patient with anterior neck trauma is considered to have an upper airway injury. The classic symptoms of laryngeal trauma include hoarseness, laryngeal pain, dyspnea, and dysphagia (Table 77.1). It is surprising that no single symptom seems to correlate well with the severity of injury (2). When the laryngeal lumen is severely compromised, aphonia and apnea occur, signifying the need for immediate establishment of an alternative airway.
Physical Examination
After trauma, a thorough physical examination of the neck is needed to identify associated neurovascular injuries. Cervical spinal injuries must be ruled out for all patients with neck trauma. Active bleeding, expanding hematoma, bruits, and the loss of pulses are signs of vascular injury. The usual signs of laryngeal trauma include stridor, hemoptysis, subcutaneous emphysema, and tenderness or deformity of the laryngeal skeleton. The presence of tenderness to palpation helps to differentiate an acute laryngeal fracture from an old deformity. The type of stridor can suggest the location of the lesion. Inspiratory stridor typically indicates partial supraglottic airway obstruction, as might occur from edema, hematoma, foreign body, soft tissue injury, or cartilaginous fractures. Expiratory stridor may portend a lower airway abnormality caused by a tracheal injury. Combined inspiratory and expiratory stridor suggests partial obstruction at the level of the glottis.
TABLE 77.1  DIAGNOSIS LARYNGEAL TRAUMA DIAGNOSIS LARYNGEAL TRAUMA | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
Cervical subcutaneous emphysema is associated with loss of the integrity of the upper aerodigestive tract and is thought to occur through shear forces of the laryngeal cartilage against the vertebral bodies (10). The amount of air can range from slight soft tissue emphysema to massive pneumomediastinum. Associated soft tissue derangements of the larynx can produce a ball-valve effect that forces massive amounts of air into the neck and chest as well. Further compromise of the airway can be caused by tracheal displacement or tension pneumothorax. Care should be taken to avoid excessive mask ventilation in patients with laryngeal trauma as this can worsen subcutaneous emphysema and potentially cause a pneumothorax (11).
Direct fiberoptic laryngoscopy is an integral component for evaluation of the patient with blunt laryngeal trauma. The larynx is examined for mobility of the vocal folds, position of the arytenoid cartilages, hematoma, lacerations, and airway patency. Rigid esophagoscopy is the best way to examine the hypopharynx and esophagus
when indicated, but should only be carried out after cervical spine injury has been excluded (12). In patients with minor laryngeal injuries, strobovideolaryngoscopy should be performed to better assess subtle intricacies of vocal fold function (13).
when indicated, but should only be carried out after cervical spine injury has been excluded (12). In patients with minor laryngeal injuries, strobovideolaryngoscopy should be performed to better assess subtle intricacies of vocal fold function (13).
Radiologic Evaluation
Computed tomography (CT) (Fig. 77.1A and B) has clearly become the most useful radiologic examination for evaluating laryngeal trauma (12, 14, 15, 16). CT is most useful when the results influence treatment, as opposed to documentation of an obvious injury when management will not be changed. Two groups of patients may not benefit from CT examination: (a) Patients with minimal anterior neck trauma and normal physical findings and (b) Patients with obvious fractures, large endolaryngeal lacerations, or severe penetrating injuries. While the latter patients will most often need tracheotomy, direct laryngoscopy, and open exploration, many authors now agree that CT can be of benefit even in this group in planning structural repair (15). The practical side of this is that most patients in this category will have been intubated and had a CT of the neck already performed by the time one is consulted. All patients in the intermediate group should undergo CT to assess the extent of laryngeal injury. When used, CT helps to confirm indirect or flexible laryngoscopic findings, to detect cartilage fractures that are not clinically apparent, to
assess poorly visualized areas, such as the subglottic and anterior commissure regions, and to identify associated cervical injuries (14).
assess poorly visualized areas, such as the subglottic and anterior commissure regions, and to identify associated cervical injuries (14).
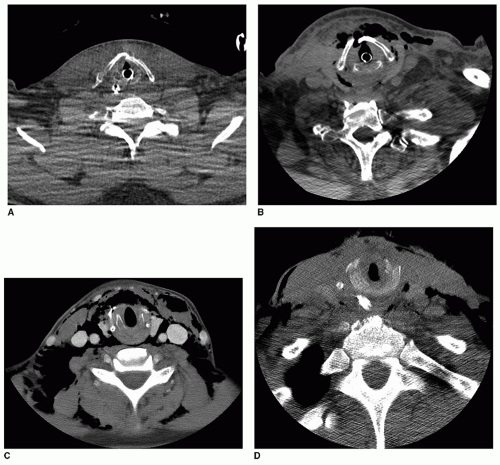 Figure 77.1 A: Minimally displaced laryngeal fracture. B: Moderately displaced laryngeal fracture. C: Severely displaced laryngeal fracture. D: Displaced cricoid fracture. |
Special radiographic studies can be useful in identifying injuries associated with laryngeal trauma, especially with penetrating trauma. Cervical or “arch” arteriography continues to be most commonly used to identify vascular injury, although helical CT, MR angiography, and color duplex ultrasonography are replacing this in some institutions (12, 17). Pharyngeal and esophageal mucosal penetration can be identified with the use of a Gastrografin followed by barium swallow examination, although this should be pursued with caution due to the risk of aspiration associated with laryngeal injury. Radiographs of the cervical spine are needed to rule out vertebral injury. Particular care is taken to visualize the entire cervical spine to avoid missing injuries of the lower cervical vertebrae. Ultrasonography has been considered as an adjunctive diagnostic aid in acute laryngeal trauma due to its mobility and easy handling; however, it is not widely utilized (18).
MANAGEMENT
Figure 77.2 shows a management protocol for acute injuries to the larynx. There are two primary goals in the management of acute laryngeal trauma—preserving life by maintaining the airway and restoring function as judged by lack of dependence on a tracheostomy and by voice quality. These goals are universally accepted, but the most appropriate methods to achieve them are controversial (19).
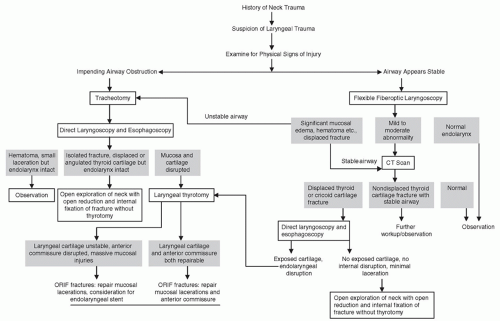 Figure 77.2 Management algorithm for suspected laryngeal injury. |
Emergency Care
The initial evaluation and treatment of a trauma patient consists of airway preservation, cardiac resuscitation, control of hemorrhage, stabilization of neural and spinal injuries, and a systematic investigation for injuries to other organ systems (Table 77.2). Controversy exists regarding the best way to establish an alternative airway in the presence of laryngeal trauma (19). If orotracheal intubation is performed in the setting of laryngeal trauma, it is best done under direct visualization by experienced personnel using a small endotracheal tube with a high-volume, lowpressure cuff with an otolaryngologist present (12). These requirements cannot always be met when laryngeal trauma is present. However, the attempted endotracheal intubation of a traumatized larynx can cause iatrogenic injury or the loss of an already precarious airway. For these reasons, some authors strongly recommend tracheotomy with local anesthesia rather than endotracheal intubation for persons who have sustained laryngeal trauma and need an alternative airway (2, 15, 20). Patients with minimal laryngeal
injury, documented with flexible laryngoscopy and CT, can safely undergo careful endotracheal intubation if it is needed to manage other injuries. Such intubation should be performed by a highly experienced physician to avoid further injury to the larynx.
injury, documented with flexible laryngoscopy and CT, can safely undergo careful endotracheal intubation if it is needed to manage other injuries. Such intubation should be performed by a highly experienced physician to avoid further injury to the larynx.
TABLE 77.2  EMERGENCY CARE LARYNGEAL TRAUMA EMERGENCY CARE LARYNGEAL TRAUMA | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||
A child with a traumatized larynx presents a special case because it usually is difficult to perform tracheotomy under local anesthesia in this situation. Inhaled anesthesia with spontaneous respirations is used to achieve bronchoscopic intubation, which allows direct visualization of laryngeal injuries and prevents additional iatrogenic injury (11, 21). Some authors recommend needle cricothyroidotomy and jet insufflation for patients younger than 12 years (22). However, obtaining a needle cricothyroidotomy may be difficult with loss of laryngeal landmarks, and jet insufflation may worsen subcutaneous emphysema or pneumomediastinum (22).
Treatment Decision Making
Management is divided into medical and surgical treatment according to the extent of injury as determined at physical examination and CT (Table 77.3). The decision to treat a patient medically or surgically is determined by the likelihood that the injury will resolve without surgical intervention. The following conditions are likely to resolve spontaneously without serious sequelae: edema, small hematoma with intact mucosal coverage, small glottic or supraglottic lacerations without exposed cartilage, and single nondisplaced thyroid cartilage fractures in a stable larynx (15, 16, 20). Some evidence, however, suggests that the repair of even single nondisplaced angulated fractures can prevent subtle vocal changes, as shown by acoustic impedance (23). Strobovideolaryngoscopy may be useful in determining which minor injuries may cause phonatory disorders (13




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
