15 Laryngeal Framework Surgery Payr,1 a German surgeon, is credited with the first description of a laryngoplasty via a transthyroidal approach, but it was Isshiki in 1974,2 who first classified the main techniques that alter the skeleton of the larynx (and therefore the vibrational properties of the vocal folds) rather than operating directly on the vocal folds themselves. His research and elegant classification prompted others to adopt this approach, and several surgeons, including Koufman,3 published case series of patients who had undergone successful vocal fold implantation. Until this time, intracordal injection was the cornerstone of surgical therapy for symptomatic vocal fold paralysis (VFP), but laryngoplasty has many advantages over this as shown in Table 15.1. In 2001, the Phonosurgery Committee of the European Laryngological Society (ELS)4 proposed the collective term “laryngeal framework surgery” as synonymous with laryngoplasty or glottoplasty. For ease of use and syntax, the term laryngoplasty will be used throughout in this chapter. These procedures are performed open, as opposed to the majority of operations performed on the vocal folds that are performed either perorally or transcutaneously. They involve an external approach to the laryngeal skeleton and a change in its shape or position. This causes vocal fold repositioning and subsequent vocal alteration. They are used to change the quality of the voice rather than for removal of disease. Table 15.2 shows the classification of laryngoplasty, but it is mainly the approximation type that is performed and that will be described in detail in this chapter. Expansion and relaxation laryngoplasty are rarely performed, many centers preferring the use of repeated Botulinum injections, and tension laryngoplasty has a role not only for the transsexual voice, but also for patients with superior laryngeal nerve paralysis.5 The primary aim of this procedure is to approximate the vocal folds, so that glottic closure is achieved and voice restored. In addition, this will ensure competence of the larynx and allow protection of the lower respiratory tree. A unilateral VFP, with the fold in the lateralized position, results in a breathy, quiet voice due to the inability of the vocal folds to meet. As well as VFP, vocal fold immobility caused by scars, atrophy, and Grade III sulcus can also be treated with approximation.6 As well as symptoms of the voice, glottal insufficiency may lead to aspiration and dysphagia that can also be an indication for approximation of a paralyzed vocal fold.7 In these cases, it is usually a high vagal lesion affecting both superior and recurrent laryngeal nerves and having both sensory and motor laryngeal deficits. Most patients with unilateral VFP have a synkinetic cord where there has been some reinnervation but this has been nonselective, resulting in uncoordinated movement but they do have muscle tone.8 Reinnervation procedures now focus on selective neural anastomosis, identifying the adductor and abductor branches separately with theoretically better functional outcomes.9,10 Table 15.1 Comparison of Closed (Injection) versus Open (Laryngoplasty) Medialization Thyroplasty
History
Definition
Approximation Laryngoplasty
Indications
Technique | Injection | Laryngoplasty |
Anesthetic | Local and/or general | Local and/or general |
Glottic closure | Small to medium—can straighten small irregularities in medial edge | Small, medium, and large—not good for small irregularities in medial edge |
Mucosal wave | Can be reduced if there is migration or placement too superficial | Lies lateral to muscle and does not reduce mucosal wave |
Time for procedure | Around 30 min | Around 60 min |
Alters tension | No | Yes |
Alters position | Yes | Yes |
Alters vibrational mass | Yes | No |
Morbidity | Minimum with endoscopic or transcutaneous approach | Open wound |
Level of skill required | Moderate | Moderate to high |
Table 15.2 European Laryngological Society Classification of Laryngoplasty
Approximation laryngoplasty | ||
Medialization thyroplasty | Thyroplasty I | |
Arytenoid adduction | Rotation techniques | Isshiki et al16 |
| LCA pull technique | Iwamura22 |
| Fixation techniques | Morrison23 Maragos24 |
| Adduction arytenopexy | Zeitels et al17 |
Expansion laryngoplasty | ||
Lateralization thyroplasty | Lateral approach |
|
| Thyroplasty IIa | |
| Medial approach |
|
| Thyroplasty IIb | |
Vocal fold abduction | Suture technique | Isshiki25 |
| Resection technique | Woo and Genack27 |
Relaxation laryngoplasty | ||
Shortening thyroplasty | Lateral approach |
|
| Thyroplasty III | Isshiki25 |
| Medial approach |
|
| Anterior commissure retrusion | |
Tensioning laryngoplasty | ||
Cricothyroid approximation | Thyroplasty IVa | Isshiki et al2 |
| Cricothyroid subluxation | Zeitels et al31 |
Elongation thyroplasty | Lateral approach |
|
| Thyroplasty IVb | |
| Medial approach |
|
| Springboard advancement | LeJeune et al34 |
| Anterior commissure advancement | Tucker35 |
LCA, lateral cricoarytenoid muscle.
Less than 10% of cases have complete denervation and atrophic muscles, but these are important to identify preoperatively as there is an increased risk of perforating the laryngeal mucosa when forming the pocket for the implant.
Patient Selection
The investigations of a patient with a unilateral immobile vocal cord will not be discussed in this chapter, but thorough assessment and investigations are important and must be performed for every case preoperatively.11
Symptomatic glottic insufficiency can be due to numerous causes, but approximation laryngoplasty (medialization thyroplasty) is our operation of choice for:
•Unilateral vocal cord immobility with a small-to-medium glottic gap.
•Severe presbylaryngeal changes with bilateral bowing and a glottic gap greater than 2 mm.
Perhaps, more importantly, it is useful to know who is NOT a good candidate and why?
•Patients who have had laser resection of the vocal cords and are left with mainly scar tissue lying on the inner surface of the cartilage. Although medialization of this tissue is possible, the implant needed is usually large, and pitfalls include implant extrusion through the thin tissue into the airway and poor vibration of the medialized tissue. Inserting a local muscle flap to lie between the implant and the scar tissue can be done but this can shrink with time, and long-term results are variable.
•Large glottic gaps, especially posteriorly, will need the addition of an arytenoid adduction procedure and are unlikely to get good closure with laryngoplasty alone.
•Patients with neuromuscular diseases such as multiple sclerosis do not do well as although glottic closure can be achieved, there is a lack of power to achieve this regularly as well as the secondary effect of poor respiratory function.
•Patients with widespread malignancy and a short life expectancy can be treated quickly and efficiently with a transcutaneous injection under local anesthesia in the clinic. Although the long-term results in our hands are not as good as with laryngoplasty, the priority here is a competent larynx for voice and swallowing, and this can be achieved immediately in clinic rather than waiting for theater time, etc.
Technique
All laryngeal framework surgical procedures must be performed in theater under aseptic conditions and ideally local anesthesia with sedation.
Anesthesia
Always try to do this under local anesthesia. The main advantages are auditory feedback from the patient to fine-tune the size and placement of the implant and to prevent over medialization and airway compromise. Reported cases of airway compromise are usually performed under general anesthesia, and the problem is only identified in recovery as the patient awakes. It is essential to work with the same anesthetist regularly and to develop a team approach. Levels of consciousness need to be fairly low during the exposure phase of the procedure, but then higher when the patient is asked to speak.
A variety of agents have been used to sedate patients, including benzodiazepine/opioid combinations, with flumazenil administered when patient cooperation is required. However, with the availability of the short-acting opioid remifentanil, this has become the preferred agent, often in combination with a target-controlled infusion of propofol. Bispectral Index (Bis) monitoring can be used to aid the anesthetist in ensuring the patient remains comfortable and relatively motionless without suppressing respiratory drive, and avoid dramatic fluctuations in conscious level during the procedure. In certain instances, the patient may not be able to tolerate local and general anesthesia may be required. An endotracheal tube can alter the endolaryngeal anatomy, so it is suggested that a laryngeal mask airway is used. This will also allow a fiberscope to be passed through it to visualize the glottis intraoperatively, but there will not be any auditory feedback hence the superiority of using local anesthesia.
Positioning
Use a headlight and magnifying loupes. Initially, stand on the opposite side of the table to the side of surgery. It is easier to get under the strap muscles and onto the thyroid cartilage from the opposite side. Current trials are looking at the role of preserving the strap muscles, including the cricothyroid muscle on postoperative voice results but it often comes down to access and the deeper lying, less acutely angled thyroid cartilages may need more extensive dissection for adequate exposure. When the cartilage has been exposed, it can be easier to be on the same side of the table especially if using a drill. Leave the patient’s head completely exposed—this allows access for the anesthetist and for insertion of the flexible nasoendoscope later.
Placement of the Window
The technique is well described12 but essentially involves removing a cartilaginous window from the thyroid alar on the affected side overlying the vocal fold (Fig 15.1). In contrast to absolute measurements, the relative proportions are more constant,13,14 and one should start by identifying the superior and inferior thyroid cartilage notches and the midpoint in the midline. This is the point of insertion of Broyles tendon and is at the horizontal level of the vocal folds. From this point, the vocal fold, within the endolarynx, runs posteriorly and inferiorly at an angle of approximately 15 degree. Due to the variability of laryngeal rotation and anterior projection, it is easier to think of the vocal fold running parallel to the inferior border of the thyroid cartilage.14
With this in mind, the rectangular window excised from the thyroid cartilage must run also run parallel to the inferior border of the thyroid cartilage so as to have the body of the implant running in the same axis as the vocal fold. There is debate as to where the most anteriorly based vertical incision should be made; Isshiki suggested 5 to 7 mm from the midline, however, Friedrich has postulated that it should be made in the area of the oblique line.13 The authors prefer to make their anterior incision approximately 7 mm (female) or 9 mm (male) from the midline but this does vary with the size of the thyroid cartilage. We remove a 12 × 5 mm window for men (10 × 4 mm for women) but one size does not fit all, and the size of the window needs to be tailored to the patient’s dimensions.
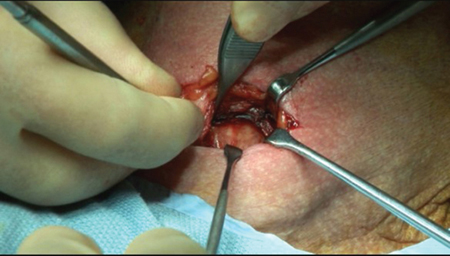
Figure 15.1 Exposing left thyroid lamina.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


