Lacrimal Gland Tumors
Brent Hayek
Bita Esmaeli
Masses of different types can develop in the lacrimal gland and lacrimal gland fossa (Table 1). Lacrimal gland tumors can be categorized as infectious lesions, inflammatory lesions, lymphoproliferative lesions, benign epithelial tumors, and malignant epithelial tumors. Overlapping clinical presentations of mass lesions in this region are common, but findings on history, and specific findings on examination and imaging can help distinguish between different types of lesions.1,2,3,4,5,6 Radiographic modalities, particularly computed tomography (CT) and magnetic resonance imaging (MRI), are useful in delineating the type of lacrimal gland process.7,8,9
 |
This chapter will outline the clinical presentation and management of the various types of tumors that affect the lacrimal gland. The chapter will also briefly review the anatomy of this orbital region and the American Joint Committee on Cancer (AJCC) staging system for lacrimal gland tumors.
Anatomy of the Lacrimal Gland
The lacrimal gland is an almond-shaped structure in the superolateral orbit. It measures approximately 2 cm × 1.2 cm × 0.5 cm. It is related both morphologically and histologically to the minor salivary gland.10 The lacrimal gland consists of 2 lobes, the anterior palpebral lobe and the larger, deeper orbital lobe. The palpebral lobe is half to one-third the size of the orbital lobe. The lobes are separated by the lateral horn of the levator aponeurosis. The main function of the lacrimal gland is aqueous tear production; however, recent findings indicate that lacrimal acinar cells are also able to secrete mucin.11
Presentation of Lacrimal Gland Lesions
Lacrimal gland lesions typically present with fullness of the lateral-orbital soft tissue structures. If the lesion is large enough, the eye may be displaced medially and inferiorly. The eyelid may have an S-shaped appearance like that seen in plexiform neurofibroma. The globe, eyelid, and other soft tissues may appear quiet or erythematous and edematous, depending on the degree of associated inflammation. Inflammatory lesions are painful, are tender, and are often acute processes. Lymphoproliferative lesions, like lymphoma, also present with upper lid fullness but are clinically softer masses than epithelial tumors. Lymphoproliferative lesions mold around orbital structures and are usually associated with no inflammatory signs. Epithelial tumors, like benign pleomorphic adenomas and adenoid cystic carcinomas (ACC), are slow to develop and are less likely to be associated with acute inflammation.
Duration of symptoms is an important factor to consider in the evaluation of mass lesions of the lacrimal gland. Pleomorphic adenomas tend to be symptomatic for more than a year before diagnosis, and displacement of the globe is a common finding (Fig. 1) without pain or signs of inflammation. Malignant tumors, such as adenoid cystic carcinoma, are typically diagnosed less than 1 year after symptoms develop, although there are exceptions to this rule. Malignant tumors are also more often associated with orbital pain and/or supraorbital dysesthesia than are benign tumors. Pain is attributed to perineural invasion or direct extension of the tumor into the orbital roof and/or lateral wall(s).
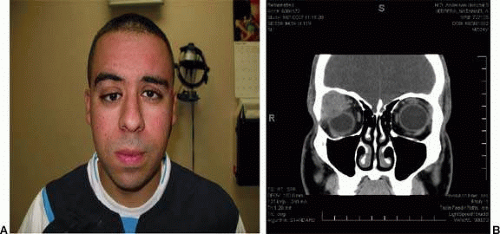 Figure 1. A. 26-year-old man with downward displacement of the right globe and motility restriction from a pleomorphic adenoma of the lacrimal gland. His symptoms developed over an approximately 2-year period prior to presentation. B. Computed tomography in the same patient shows a large lacrimal gland mass with remodeling of the bony lacrimal gland fossa suggesting slow growth of the mass. |
Patient age is another factor that may offer clues to the type of lesion. Acute inflammations such as idiopathic dacryoadenitis and pseudotumor-type lesions involving the lacrimal gland most often present in younger individuals.12 In studying idiopathic orbital inflammation, Yuen and Ruben found that isolated dacryoadenitis was the most common cause and that the mean age of all patients with orbital inflammatory syndrome was 45 years.13 However, idiopathic and systemic-associated lacrimal gland inflammations can occur at any age.
Lymphoproliferative lesions more commonly affect elderly individuals; they are most often seen in the seventh and eighth decades of life.
Epithelial tumors, such as adenoid cystic carcinoma, have a bimodal distribution of age at presentation. The less aggressive, cribriform variety is most often seen in teenagers and young adults, whereas the more aggressive, solid (basaloid) variety is most often seen in people 40 to 60 years of age.
Evaluation of Lacrimal Gland Lesions
A complete clinical history, examination, and imaging are necessary to evaluate lacrimal gland lesions and establish a working differential diagnosis.
The evaluation should begin with a review of the patient’s complaint(s) and past medical history. It is important to look for systemic conditions associated with lacrimal gland lesions, such as sarcoidosis, Wegener’s granulomatosis, Graves’ orbitopathy, and Sjögren syndrome. The patient’s age and the duration of symptoms should be noted. The patient should be asked specifically about pain and supraorbital dysesthesia.
A thorough ophthalmic examination is required since lacrimal gland mass lesions are sometimes difficult to clinically differentiate from other orbital tumors. Extraocular motility dysfunction and compressive optic neuropathy may be present. There may be signs of asymmetry, proptosis, periorbital erythema, conjunctival injection, or edema on adnexal examination.
Palpation of the upper lid complex is important. One should feel for the superior orbital rim and note the consistency of any mass inferior and within the lacrimal fossa. Such a mass may be soft and rubbery, as in lymphoma, or firm and fixed, as in adenoid cystic carcinoma. Sensation in the V1-V2 distribution should be checked. Exophthalmometry should be performed, and best-corrected visual acuity, findings on pupillary examination, ocular motility, visual fields, intraocular pressures, and findings on anterior segment and funduscopic examination should be noted. Finally, it is important to palpate for adenopathy in the preauricular, submandibular, and cervical chains. This may reveal regional spread in cases of lymphoma or epithelial carcinoma.
CT is considered the initial modality of choice. Thin axial and coronal cuts delineate the borders of the lacrimal gland well and depict the surrounding bone better than MRI.7 In evaluating lacrimal gland lesions, internal tissue features on T1- and T2-weighted images may be helpful in categorizing unilateral lacrimal gland lesions.9 Certain types of lesions have distinguishing characteristics that, combined with clinical information, allow the physician to form a more accurate diagnosis. For example, benign pleomorphic adenomas are typically well-circumscribed, encapsulated, heterogeneous masses that may show some bone remodeling and excavation of surrounding bone (Figure 1B).7 Smaller adenomas are usually more cellular and thus may appear more homogeneous. By comparison, adenoid cystic carcinomas are aggressive tumors that can invade bone and periorbital structures (Fig. 2) and have a propensity for early perineural spread. Adenoid cystic carcinomas do not contain a capsule, and on imaging, surrounding bone may appear eroded, as lesions invade adjacent structures.7
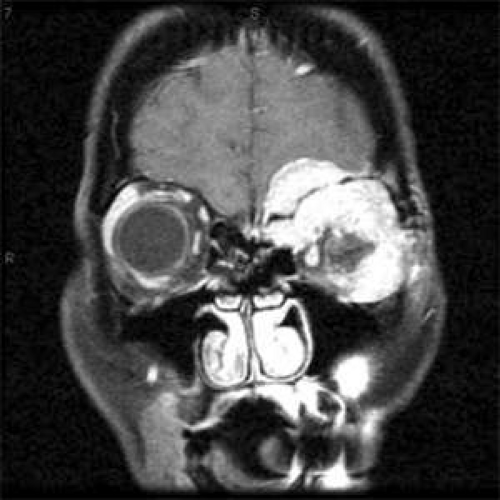 Figure 2. A. Magnetic resonance imaging in a patient with adenoid cystic carcinoma of the lacrimal gland highlights the aggressive nature of this cancer with expansion into the brain parenchyma due to previous incomplete excision. (Reproduced from Esmaeli B, Golio D, Kies M, DeMnte F: Surgical management of locally advanced adenoid cystic carcinoma of the lacrimal gland. Opthal Plastic Reconstr Surg 22:366–370, 2006 with permission). |
Inflammatory Lesions of the Lacrimal Gland
Acute dacryoadenitis is mostly idiopathic and can be thought of as a subset of orbital inflammatory syndrome.13 Acute dacryoadenitis may also be related to infections, more commonly in children, or systemic autoimmune diseases in adults. It presents as erythematous swelling of the upper lid in the superolateral aspect of the orbit. It usually is painful, unlike lymphoproliferative disease. Acute dacryoadenitis is often unilateral; bilateral disease usually occurs in children or is indicative of a systemic process. In the pediatric population, there are frequently systemic symptoms and signs of fever, nausea, vomiting, and malaise. There may also be an increased erythrocyte sedimentation rate, eosinophilia, and pleomorphic cerebrospinal fluid. Other adnexal structures may also be involved, including extraocular muscles, Tenon’s capsule, the sclera, orbital fat, and the optic nerve. CT is warranted to help with the diagnosis. CT findings include an ill-defined mass, marked contrast enhancement of the lesion and surrounding tissue with fat stranding and associated inflammation of orbital structures.
A biopsy is needed to confirm the diagnosis unless there is rapid response to a short course of antibiotics. In the case of specific inflammatory lesions of the lacrimal gland, such as sarcoidosis, once the diagnosis is confirmed on biopsy, a systemic workup is needed to rule out systemic pulmonary sarcoidosis and other organ involvement.
The management of inflammatory lesions of the lacrimal gland depends on the underlying etiology. Once infection is ruled out, systemic steroids on a slow taper may be considered. In the case of nonresponsive or recurrent or refractory disease, radiation therapy or other systemic cytotoxic therapy can be considered.
Lymphoproliferative Lesions of the Lacrimal Gland
Lymphomas are the most common primary cancers in the orbit in adults, representing 20% of orbital masses.4,14,15,16 Almost all lymphomas of the orbit, lacrimal gland, or conjunctiva are of the non-Hodgkin’s B cell types; the lacrimal gland is a frequent site of involvement and is estimated to be involved in about 50% of all cases of orbital lymphoma (Fig. 3A).17 Extranodal marginal zone B cell lymphoma (low grade B cell lymphoma of MALT type) is the most common histologic subtype seen in the orbit (Fig. 3B);4,5,14,17,18 the next most common subtypes, in decreasing order of frequency, are follicular lymphoma, diffuse large cell lymphoma, and mantle cell lymphoma.
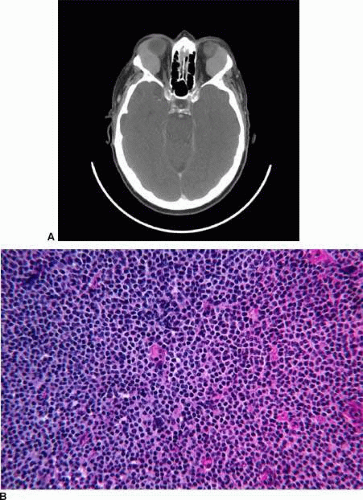 Figure 3. A. Computed tomography in a 65-year-old patient with bilateral lacrimal gland lymphoma. B. Histologic findings of low-grade Non-Hodgkin’s B cell lymphoma. |
Clinically, both primary and secondary lymphoproliferative lesions of the lacrimal gland tend to grow slowly and be associated with minimal or no pain or acute swelling.5,6 Most patients have unilateral disease, are elderly, and present with symptoms of less than 1 year’s duration. The overall rate of systemic involvement associated with orbital lymphoma is reported to be 30% to 50%.19 After the diagnosis of lymphoma of the lacrimal gland is established via a biopsy, a thorough systemic workup is warranted to look for systemic sites of involvement. A total-body positron emission tomography scan is a way to rule out areas of hypermetabolic activity throughout the body and serves as a complement to conventional imaging for staging of lymphomas.19 Positron emission tomography scans can also be used to evaluate response to therapy.20
Benign Epithelial Tumors of the Lacrimal Gland
Pleomorphic adenoma
The most common epithelial tumor of the lacrimal gland is pleomorphic adenoma (benign mixed cell tumor),22,23 which accounts for approximately 50% of all epithelial lacrimal gland tumors.5 Pleomorphic adenoma most commonly presents in the fourth to fifth decades of life and is rare in children.5,23,24,25 Actuarial estimates indicate that the risk of transformation to malignancy if pleomorphic adenoma is left untreated is 10% in 20 years and 20% in 30 years.23
Pleomorphic adenoma commonly presents as a slowly progressive, painless mass in the lacrimal gland fossa. Most pleomorphic adenomas affect the orbital lobe, so the more common finding is axial proptosis with downward and medial displacement. However, it may present solely with eyelid ptosis.3 Patients may complain of diplopia from globe dystopia and restricted eye movement. Other signs, such as choroidal striae may also be evident. This tumor affects males slightly more frequently than females and is usually symptomatic for more than a year before diagnosis.5,23,24,25 Though the orbital lobe is affected in almost all patients, benign pleomorphic adenomas of the palpebral lobe have also been described.10,22 Patients with such tumors do not have proptosis, since tumor growth is exterior to the orbit. In Rose and Wright’s series of 78 patients with pleomorphic adenoma, the tumor was confined to the palpebral lobe in eight patients (10%).1 The authors found that on average, patients in this subgroup presented with symptoms present for less than 1 year. However, others report that palpebral-lobe tumors may have a longer duration of symptoms before diagnosis, up to 21 years.22,26,27,28,29 Examination typically demonstrates a firm, mobile mass just inferior to the superolateral orbital rim. CT and MRI often show a roundish mass of varying homogeneity, with evidence of bony excavation and remodeling correlating with the slow growth of this lesion. Bony excavation and remodeling is the classic finding on imaging but is not always present. In their review of patients with lacrimal gland pleomorphic adenomas, Garrity et al. found that only 44% of patients had bony abnormalities.3 Also, they reported one patient with a 1-cm defect in the orbital roof.3,25,30 Atypical presentations of this tumor are not rare. Recently, Vagefi et al reported on three different patients with pleomorphic adenoma, one with signs imitating orbital cellulitis, another with a painful subcutaneous nodule, and one with calcifications and bone erosion on CT.31 Others have reported presentations mimicking chalazion or dacryoadenitis.32,33,34
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


