Lacrimal Drainage Surgery
James A. Katowitz
Scott M. Goldstein
Femida Kherani
Joanne E. Low
Epiphora is a sign of an imbalance between tear production and drainage. Examination of the patient with epiphora reveals either an overproduction of tears or decreased drainage through the nasolacrimal system. Obstruction of the tear drainage system can be congenital or acquired and may occur at any level along the system. Patients may present with epiphora as well as other problems such as dacryocystitis. Congenital obstructions are typically caused by imperforate lacrimal systems. Acquired obstruction may be secondary to previous surgery, radiation, chronic inflammation or trauma. Involutional and medication-induced changes may also contribute to nasolacrimal duct obstruction. Regardless of the etiology, the principles of surgical repair are the same. This chapter reviews the common problems of lacrimal drainage and their current evaluation and management modalities, emphasizing surgical treatment.
EVALUATION OF EPIPHORA
When a patient presents with epiphora, it is important to determine the etiology of tearing. The tearing may be a result of external disease including tear film, corneal, lid, or lash anomalies, or the result of nasolacrimal obstruction. It is convenient to divide lacrimal obstruction problems into congenital versus acquired problems and to distinguish upper system (proximal) from lower system (distal) obstruction (Fig. 1). The upper system is defined as the area extending from the external puncta through the canaliculi, to the common internal punctum in the lacrimal sac. The lower system includes the lacrimal sac through the valve of Hasner.
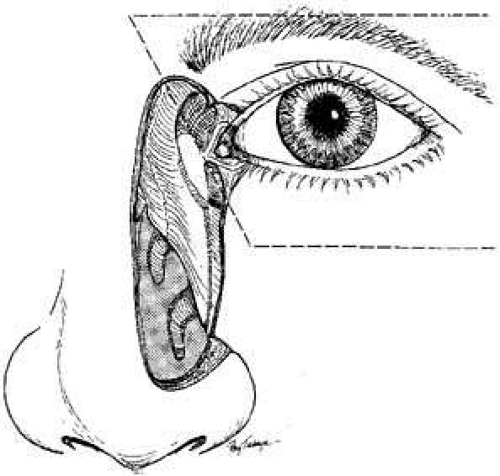 Fig. 1 Normal anatomy of nasolacrimal apparatus showing potential sites for obstruction. An obstruction occurring anywhere from the external puncta, canaliculi, or through the common opening (internal punctum) constitutes an upper system block (enclosed area). Any obstruction from the lacrimal sac through the nasolacrimal duct into the nose constitutes a lower system block. |
Information regarding the nature of tearing—amount, frequency, associated mucopurolent discharge—and presence of a periocular mass is useful. Examination of the medial canthal area is necessary. Any redness, swelling, discharge, or skin changes should be noted. Because two thirds of the lacrimal sac lies below the medial canthal tendon, a mass that is located above this tendon may indicate an anterior ethmoidal mucocele, intraorbital tumor, or nasofrontal encephalocele. Expression of mucoid material retrograde through the puncta with pressure on the lacrimal sac may confirm the presence of nasolacrimal obstruction or stenosis. Several clinical tests, including the dye disappearance test (DDT) are useful tools. These tests are outlined later in this chapter.
Most adults who report epiphora do not have an obvious overflow of tears. More frequently, there is an increase in the height of the tear meniscus between the lower lid and the cornea. Obstruction to the flow of tears can lead to secondary blepharoconjunctivitis at any age. Canaliculitis occurs more commonly in adults, and is usually related to dacryoliths or casts obstructing flow which can result in infection. Severe cellulitis caused by infection of the lacrimal sac (dacryocystitis) also can occur.
Lid margin abnormalities can produce epiphora, especially as an involutional phenomenon. Ectropion, particularly of the lower punctum, obviously can lead to overflow of tears. Lid laxity alone, however, may interfere with the lacrimal pump mechanism or produce exposure with secondary reflex tearing. In adults, use of the Jones dye tests may also be helpful. In our experience, the combination of the DDT, lacrimal irrigation, and inspection of lid anatomy provides the necessary information in most instances. If there is any suspicion of tumor in the sac or drainage pathways, a dacryocystogram (DCG), magnetic resonance imaging (MRI) or computed tomography (CT) scan should be performed. Entropion can stimulate reflex tearing through irritation of the globe by the lashes. Similarly, trichiasis and distichiasis may produce epiphora.
One of the most common sources of confusion is evaluating adult tearing given an apparently open lacrimal drainage system. This tearing is typically a reflex response resulting from a dry-eye or sicca problem. For this reason, it is especially important to evaluate baseline tear production properly. Observation of the tear meniscus, tear breakup time, and Schirmer’s testing are important in assessing the adult lacrimal system because aggressive opening of drainage in the face of a dry eye can lead to more significant problems. The DDT is especially helpful in children.1,2 The traditional Jones dye tests are more useful in adults.3,4,5 Dacryocystography and lacrimal scintigraphy also are of value, especially in excluding functional blocks when the nasolacrimal system is open to irrigation. All of these tests are described in detail elsewhere,6 but a brief review may be useful as an introduction to the surgical management of acquired lacrimal drainage problems.
OBSERVATION
Observation is the most basic tool available to the clinician. The level of tears should be noted. In addition, the position of the lids and the apparent functioning of the lacrimal pump mechanism should be assessed. Pressure on the lacrimal sac may provide additional information indicating a mucocele or true infection of the lacrimal sac. Material expressed in this fashion can be sent for smears and appropriate cultures and sensitivities although this is not a necessity.
EVALUATION OF BASELINE TEAR PRODUCTION
In addition to observation of the tear meniscus, the basal tear secretion test (BTST) with the use of a topical anesthetic is essential.7 Less then 10 mm of wetting of filter paper (Schirmer, Whatman number 41, 35-mm long, 5-mm wide) over a 5-minute period indicates a potential problem in baseline tear production. Evaluation of the tear film can be useful in assessing the role that decreased baseline tear secretion or changes in the tear film may play in stimulating reflex tearing. A tear break-up time (TBUT) below 10 seconds indicates tear film instability.
IRRIGATION AND PROBING
Probing in the adult should be limited to the puncta, canaliculi, and proximal lacrimal sac. Gentle dilation of the external puncta should be done and the lacrimal cannula should be passed carefully in each canaliculus. Initial passage should be in a vertical direction, entering the ampulla for 2 mm, and then moving medially with the eyelid on lateral traction. Attention should be given to veils or strictures, especially at the internal common opening. Once inside the lacrimal sac a hard stop is felt against the bony medial wall. Irrigation of the system should then be undertaken. Regurgitation from the opposite canaliculus not only indicates the relative patency of the opposite canalicular system but also indicates a lower system block in either the lacrimal sac or the nasolacrimal duct. Probing of the nasolacrimal duct in an adult should be avoided because it often is painful, even with use of a local anesthetic injected through the sac and duct. More importantly, it rarely yields more than temporary relief of symptoms. Examination of the nose should be done to exclude impaction of the inferior turbinate, a deviated septum, or the presence of an intranasal neoplasm that obstructs the exit of tears from the nasolacrimal duct. Examination may be facilitated by endoscopic instrumentation.
DYE DISAPPEARANCE TEST
The DDT is a simple test in which a single drop of 2% fluorescein is instilled into the anesthetized cul-de-sac of each eye.3,8,9 Excess fluid or overflow is wiped away, and the tear meniscus observed over a 5-minute period. In a normal eye, the tear meniscus will become relatively unstained within 5 minutes. In patients with lacrimal obstruction, the stained meniscus will either increase in height or be diluted only slightly (Fig. 2). Retained dye in the tear meniscus can be graded from trace to 4+. This is an excellent quantitative test to measure lacrimal drain function, especially in children. As children sit on their parent’s lap, the DDT can be measured via the cobalt blue filter of the slit lamp opened wide and held at a distance of 2 or 3 feet from the child. Children are typically fascinated by the light and this less-threatening distance will permit observation.
 Fig. 2 Dye disappearance test with 3+ positive result in left eye. |
JONES DYE TESTS
Jones dye tests have traditionally been the most accepted method for the office evaluation of lacrimal function. However, they are tedious to perform and have a high false-negative rate. Furthermore, similar information is obtained from the DDT and irrigation of the nasolacrimal system. For the primary Jones test, a drop of 2% fluorescein is placed into the conjunctival cul-de-sac on one side.5 The inferior turbinate near the lateral floor of the nose is then sprayed with a topical anesthetic and decongestant, such as 4% cocaine. A small wire with cotton wrapped around the end or a cotton-tipped applicator (Calgiswab, Biomedical Division, Inolex, Glenwood, IL) is placed under the anterior half of the inferior turbinate. In 5 minutes, the cotton is removed and examined for staining, which indicates that flow through the lacrimal system is normal. If the dye does not stain the cotton, a functional nasolacrimal block may be present. The secondary dye test (Jones II) is performed by irrigating in the inferior canaliculus with saline and collecting the used solution in a small basin. The patient holds the basin in front of the appropriate nostril, with the head tilted forward. If the irrigated fluid is not stained with fluorescein, the dye has not passed into the canaliculus. This finding confirms the presence of a functional block.
DACRYOCYSTOGRAPHY
The DCG is a diagnostic radiologic test that uses radiopaque material that is injected with a syringe through a lacrimal cannula and into each lower canaliculus.10,11 Baseline anterior-posterior and lateral films are taken of the orbit. The dye is then injected on each side. A repeat anterior-posterior film and an oblique film are taken and then repeated at 15 and 30 minutes. The oblique position is used so that the lateral views of each nasolacrimal system are not superimposed after injection of the dye. This test can outline fistulae, diverticulae, mucoceles, neoplasms, and casts of the sac. In addition, slow clearance of the dye at 30 minutes can be helpful in confirming the presence of a functional block. In the pediatric age group, this test must be performed under general anesthesia, and the anesthesia combined with the supine position of the patient produces a nonphysiologic study in these cases. Modifications of the original DCG technique have been developed as macrodacryocystography (MDCG), subtraction MDCG, and digital subtraction MDCG.12,13 The original technique clearly shows only the lacrimal sac. The modifications include intubation of the canaliculi, macrography (enlargement of image size), and subtraction (to allow better visualization of structures); these modifications enable visualization of the entire system. Standard x-ray subtraction can involve problems with tube positioning, inadequate filling with contrast, and delay in development and subtraction. Digital subtraction, which uses angiographic equipment with fluoroscopy, eliminates these above problems. Most recently, CT scans have been used to perform DCG and can also be useful in identifying lacrimal pathology.
LACRIMAL SCINTIGRAPHY
Lacrimal scintigraphy (or dacryoscintigraphy) uses a radioactive tracer to evaluate nasolacrimal drainage. It was first described by Rossomondo and associates in 1972,14 and since that time, many studies have shown its clinical usefulness in the evaluation of nasolacrimal disorders in both pediatric and adult patients.15,16,17 Placing a controlled drop of radiologic tracer in the tear film (100 μC of sodium pertechnetate) allows the tear flow to be observed and measured with a gamma counter.11,14,18 The flow is visualized on an oscilloscope. Lacrimal scintigraphy is helpful in identifying the site of obstruction, confirming decreased transit time in functional blocks, and quantifying tear drainage. Dacryoscintigraphy has the advantages of being noninvasive and physiologic.
CONGENITAL ABNORMALITIES
The most common congenital lacrimal problems involve disturbances to tear flow through the nasolacrimal duct, and the most common presentation is epiphora, with or without mucopurulent discharge. Other congenital lacrimal problems may manifest as abnormalities of the puncta or canaliculi, external fistulae (supernumerary or anlage ducts), mucoceles (amniotoceles), and less commonly, acute neonatal dacryocystitis.
DACRYOSTENOSIS AND OTHER LOWER SYSTEM BLOCKS
Dacryostenosis may be defined as a partial or complete block in the nasolacrimal duct. The most common cause of this problem is the failure of canalization of the duct at the mucosal entrance to the inferior meatus of the nose, the valve of Hasner. Although, complete osseous obstruction can occur, especially in association with anomalous passages, relative narrowing causing decreased tear flow is a more common occurrence.19,20,21,22 Abnormalities within the nasal passages, such as deviation of the nasal septum or impaction of the inferior turbinate on the valve of Hasner, also may contribute to the obstruction of the duct.23 Examination of the nasal anatomy and a working association with an otolaryngologist are both useful.
Dacryostenosis should be managed conservatively whenever possible.24,25 The traditional approach has been to combine massage of the nasolacrimal sac and duct with topical instillation of an antibiotic.20,26 Parents must be carefully instructed as to how to perform lacrimal sac massage properly.22,27 The parent should be shown how to slide the fingertip in an inferior direction, placing moderate pressure over the sac and duct, and using the antibiotic ointment as a lubricant. This motion should be demonstrated on the parent’s own face as well as on the child. Some physicians prefer using the antibiotic drop because there is some thought that slowly dissolving ointment bases in the nasolacrimal duct may in fact contribute to obstruction. However, the ointment form can be used if it is more acceptable to the infant. We usually recommend an antibiotic ointment for massage, which also can act as a lubricant. If crusting and discharge are present, the antibiotic ointment can be applied several times daily to the conjunctival cul-de-sac.
Medical management is utilized until age 1 at which point surgical intervention is undertaken. Probing and irrigation is the main treatment. When this fails, Silastic intubation or balloon dacyroplasty may be used. If this fails, a dacryocystorhinostomy is the ultimate management. These procedures are discussed further later in this chapter.
PUNCTAL VEILS AND ATRESIA
Children with congenital epiphora may lack a patent opening into the lacrimal system. An astute physician may be able to discover the lack of a punctum in the office. However, it is more common in children to discover punctal veil or atresia at the time of probing surgery. When approaching these cases, careful inspection of the puncta using magnification is most helpful. In the setting of a veil, the punctum grossly appears normal, a punctal dilator or probe will not enter the system because a membrane covers this opening. A safety pin or sharp dilator can be used to “pop” into the system. In punctal atresia, the subtle elevation of the puncta on the lid margin is absent. On close inspection, there is no obvious opening to be found. Absence of a punctum often indicates absence of the canaliculus as well. Thus, a cut-down may or may not be helpful. If one punctum is patent it is best to leave the system alone. If both puncta on a given side are missing, a cut-down procedure in the area of the canaliculus or retrograde dissection from the lacrimal sac can be attempted. A conjunctivodacryocystorhinostomy may ultimately be required.
CONGENITAL LACRIMAL FISTULAS
A congenital lacrimal fistula is most likely the result of canalization of a portion of epithelial cord that extends from the lacrimal sac to the surface of the skin. Most fistulae originate from the lacrimal sac, but some originate from the common canaliculus or nasolacrimal duct. Simple excision of the fistulous tract has been successful in most cases.28 Other authors have recommended cautery of the fistula and excision of the fistula with dacryocystorhinostomy (DCR). Recommendations have also included DCR with common canalicular dissection, fistula excision, and canalicular intubation in certain situations.29,30
MUCOCELES (AMNIOTOCELES)
Most of the time it is not necessary to perform probing surgery before 1 year of age. One exception is a congenital mucocele, or amniotocele.31 This term refers to a sterile accumulation of mucus or possibly amniotic fluid trapped in the nasolacrimal sac due to a one-way valve effect at the end of the nasolacrimal duct. Fluid can enter the sac, but with poor exit of accumulated fluid, the dilated sac is seen as a bluish mass inferior to the medial canthal tendon. This swelling frequently is misdiagnosed as a hemangioma.19 In cases of congenital dacryocele without signs of infection, one approach is to massage the lacrimal sac in an attempt to open the obstruction. Massaging too vigorously, however, may rupture the dilated lacrimal sac and may consequently cause an orbital cellulitis. Parenteral antibiotic therapy and management similar to an acute dacryocystitis may ultimately be required.
NEONATAL DACRYOCYSTITIS
Acute dacryocystitis of the newborn is an indication for office or bedside probing of the nasolacrimal duct (Fig. 3).19,26,32 In this instance, there are other signs of inflammation, and there also may be associated fever and an elevated white blood cell count. The lacrimal sac can be tapped with a turberculin needle and syringe (Fig. 4)33 to create a fine opening that will not fistulize, as can occur with a knife incision, and allows smears to be taken immediately for early diagnosis. Likewise, material for culture and sensitivity can be obtained so that specific antibiotics can be identified. Decompression of the sac is achieved immediately, which gives relief of symptoms. Furthermore, with the needle in position, the syringe can be changed to instill 0.5 mL of a bactericidal antibiotic drop. A broad-spectrum antibiotic is given intravenously until a more specific antibiotic can be identified by the cultures and sensitivities obtained from the tap. After several days, when the acute inflammation subsides, bedside probing is valuable in most cases because it usually opens the duct and allows tear drainage so that repeat dacryocystitis will not occur. Probing must be done gently, using a small probing instrument, such as a number 000 or 0000 size Bowman probe. However, if dacryocystitis recurs after such probing, a DCR may be required to avoid further infection. DCR is usually performed early if the dacryocystitis is refractory to medical management (Figs. 5 and 6).
 Fig. 3 Neonatal dacryocystitis. |
 Fig. 4 Tuberculin syringe tap of the lacrimal sac for neonatal dacryocystitis. |
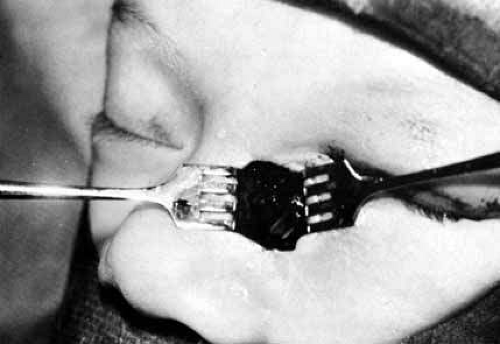 Fig. 5 Dacryocystorhinostomy (DCR) with Silastic tubing in the patient shown in Figure 2, now aged 6½ weeks. The procedure was done for medically uncontrollable dacryocystitis that was unresponsive to bedside probings. If too much methylene blue is irrigated into the lacrimal sac preoperatively as a label for the mucosal lining, when the sac is opened, it will stain the surrounding soft tissues as shown here. |
 Fig. 6 The patient shown in Figure 4, 6 months after surgery. |
Several studies have demonstrated a high success rate of DCR in the pediatric age group, equaling that of the adult population.34,35 Another consideration in DCR surgery at a young age is the potential for disruption of nasal bone growth. The surgery does not disturb any growth plates, and we have not seen any effect on facial symmetry after DCR, even when performed bilaterally at a very early age.
ACQUIRED LACRIMAL PROBLEMS
Involutional changes can cause stenosis of any part of the lacrimal drainage system. There appears to be a balance between a decrease in tear production and a decreased capacity for the nasolacrimal system to drain tears. Problems occur when these changes are out of balance. Thus it is always necessary to evaluate both the tear production and drainage in adult patients with epiphora. Punctal stenosis is one of the more obvious involutional changes and it is easily visible. Similar changes are likely occurring throughout the lacrimal system. Stenosis or complete obstruction in the nasolacrimal duct is also a common cause of epiphora. A functional block secondary to lid laxity and pump dysfunction can also occur in older patients.
PUNCTAL AND CANALICULAR STENOSIS
Adult patients with punctal stenosis will present with complaints of tearing. Close inspection will reveal stenosis that becomes more obvious during diagnostic probing and irrigation of the proximal lacrimal system. Wide dilation may suffice for acquired punctal and canalicular stenosis, but more frequently, some form of punctoplasty may be required. Several procedures are advocated. The punctal and canalicular portion of the lacrimal pump mechanism should be preserved, if possible. A variety of snip procedures have been advocated. The two-snip procedure works well to provide sufficient opening while preserving enough capillarity to allow the pump mechanism to function (Fig. 7).
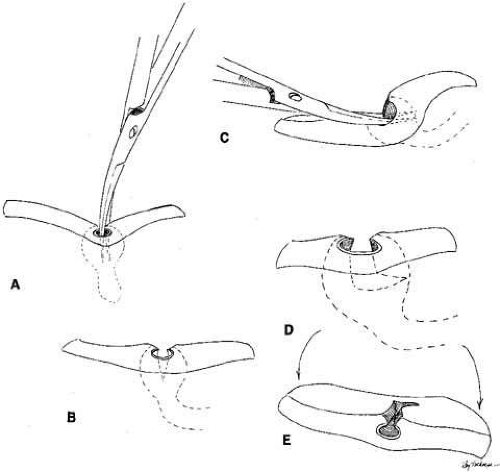 Fig. 7 The two-snip procedure. A and B. A vertical cut is made to the base of the ampulla. C–E. The scissor is passed horizontally into the canaliculis and a 3- to 4-mm cut is made. |
Stenosis can occur from involutional causes as well as from viral infections, such as herpes and varicella. Stenosis may also be the result of the toxic effects of certain topical medications. These include epinephrine-based products or long-acting anticholenergic agents used in the treatment of glaucoma.36,37 Systemic chemotherapy can also induce canalicular stenosis,38,39 which can be preemptively treated with Silastic intubation prior to starting therapy.
Canalicular stenosis is a much more serious surgical problem. For generalized but mild stenosis, Silastic intubation may suffice. If the obstruction is severe, however, a bypass procedure with the insertion of a Jones-type Pyrex tube combined with a DCR, will likely be required. Localized canalicular obstruction in the lateral half of the canaliculus may respond to Silastic intubation combined with a DCR. Anastomosis of the common internal punctum or canaliculi with the use of microsurgical techniques has been recommended. In severe cases, however, the bypass tube may be the only successful method for curing this problem.
Interestingly, some patients with dry-eye syndrome benefit from punctal or canalicular stenosis. This condition prevents the inadequate tear film from draining, increases the corneal surface tear contact time, and can improve symptoms of dry eye, including the secondary hypersecretion of tears. Correspondingly, several methods of punctal occlusion have been devised for patients with dry eye that is not relieved by lubricants who do not have anatomic stenosis. We prefer to begin with temporary collagen plugs placed in the puncta.40 These plugs dissolve over 1 to 2 weeks. If these plugs improve the symptoms, removable punctal plugs (Eagle Vision, Memphis, TN, and FCI, Marshfield, MA) can be placed. Occasionally, these plugs cause local discomfort or extrude, but in most cases, they are successful in relieving symptoms. Alternatively, cautery or Nd:YAG laser can be used to seal the inferior puncta. Of course, this treatment is not easily reversible.
CANALICULITIS
Localized painful swelling of one canaliculus can occur (Fig. 8A). Typically, as the canaliculitis worsens, the puncta becomes involved and is often referred to as a pouting puncta (Fig. 8B). Frequently, the infection is related to an acute actinomyces israelii infection.41 Smears and cultures will help in the selection of specific topical and systemic antibiotics. Surgical therapy is typically necessary. Simple irrigation and probing of the canaliculus is usually ineffective. A small curette can be used to break up concretions and the typical sulfur granules, however, the curette should not be passed through the punctum as further scarring may ensue (Fig. 8C). A better approach is to dissect directly into the affected area of the canaliculus horizontally.42 The surgeon places a probe in the punctum and canaliculus and carefully cuts down onto the metal, allowing a careful curetting if stones are present (Fig. 9). The sinus of Maier at the internal common punctum also can be examined, lavaged, or curetted. A specimen should be sent for bacterial and fungal examiniation. Silastic tubing can be used as a stent after this type of procedure, and the canaliculus and overlying tissues should be closed with interrupted 7–0 absorbable sutures. Either a posterior approach or an anterior approach can be used, but the Silastic material should remain in place for at least 3 months if there is no significant irritation or recurrent infection.
 Fig. 8 A–C. Acute canaliculitis with a pouting puncta. A posterior cutdown of the canaliculus and curettage of the granules from the system. |
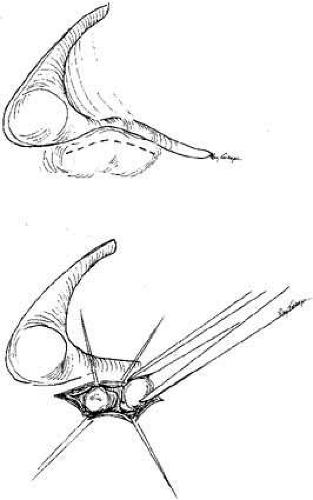 Fig. 9 Surgical approach for draining canaliculitis and removing stones. |
Stones in the lacrimal sac usually are not of fungal etiology.43 Older women are affected more frequently than their male counterparts. The concretions frequently produce intermittent obstruction. Consequently, a good history is essential. A probing and irrigation may indicate patency, despite the presence of epiphora. Lacrimal sac stones can function like a ball valve and further confuse the clinical evaluation with the intermittent epiphora. DCG is one of the most helpful tools in diagnosing this problem. A DCR may be required before a cure can be achieved. In addition to stones, always consider the possibility of a foreign body such as a punctual plug blocking the system (Fig. 10A and 10B).
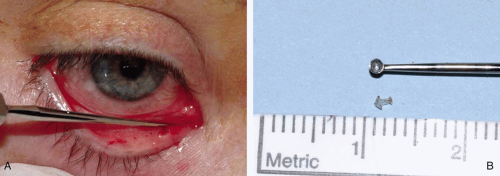 Fig. 10 A and B. Canaliculitis caused by a retained punctual plug that migrated deep into the canaliculus. A small posterior incision into canaliculus allowed for the passage of a curette (A) that retrieved the plug (B). |
STENOSIS OF THE NASOLACRIMAL DUCT
Generalized or localized stenosis of the nasolacrimal duct can result from involutional changes or secondary to bouts of infection, stones, topical medications, or other sources of inflammation. DCR is the obvious cure for lower system block in the absence of any disturbances to the punctum, canaliculus, common internal punctum and sac. The role of Silastic intubation of the nasolacrimal duct for adult dacryostenosis is controversial. Although it may work in some patients with partial stenosis, it can produce dacryocystitis by causing complete obstruction to tear outflow. In contrast to children, the adult mucosal lining and surrounding bony duct are not in a dynamic state of growth. Therefore, the tubing can act as an irritant in a fixed system. More recently balloon dacryoplasty has been suggested as a treatment for partial obstruction of the nasolacrimal duct.44 DCR is still the preferred procedure for this type of problem.
LID MARGIN ABNORMALITIES
A variety of mechanical problems of the lid margin and its fascial supports can produce tearing.
Lid Laxity
Punctal eversion alone can occur (Fig. 11) and in milder forms may respond well to vertical cautery on the conjunctival side of the lid. An alternative is excision of an ellipse or diamond of the conjunctiva and tarsus. When the margins are brought together with several interrupted absorbable sutures, the everted punctum rotates into position. True medial canthal ectropion requires a more extensive repair, such as the lazy-T procedure advocated by Smith and Cherubuni.45 Another method is actual plication of the medial canthal tendon.46 Involutional ectropion involving the entire lid interferes with the lacrimal pump mechanism and can also stimulate reflex tearing through exposure. Standard ectropion repairs cure the epiphora problems in most instances. All of these lid procedures are well reviewed in other references.6,46,47,48,49
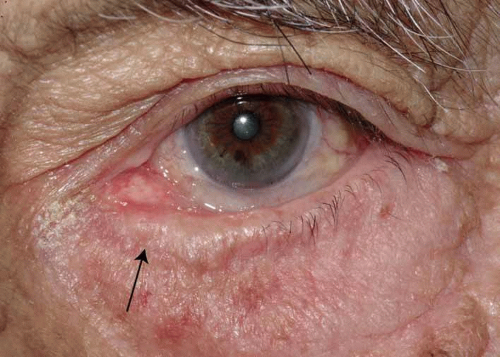 Fig. 11 Horizontal lid laxity with punctal eversion (arrow). |
Flaccid Canaliculus Syndrome
The flaccid canaliculus syndrome was described by Jones and Wobig.43 Involutional changes may produce a nasolacrimal system that appears open to irrigation. However, lid laxity and poor lacrimal pump function contribute to poor tear drainage. Horizontal shortening of the lid may help, but frequently, a Jones tube combined with DCR is required. Again, caution must be exercised to ensure that the patient does not have an underlying dry-eye problem. If so, reflex tearing will continue and the patient may be unhappy.
Irritation from Lashes
Trichiasis and distichiasis are causes of reflex tearing, as previously discussed. These problems can be managed by cryosurgery, electrolysis, or a variety of lid margin procedures. Likewise, entropion can cause reflex tearing secondary to lash irritation. Rotation of the lid margin or other standard entropion procedures can eliminate these causes of epiphora.46,47,48,49
TRAUMA
Trauma can occur at any site in the nasolacrimal drainage system. The form of trauma can range from chemical and thermal burns to avulsions and lacerations.
Burns
Whatever the source of energy causing a burn, the treatment is much the same to repair punctal or canalicular stenosis. Silastic stenting is required more frequently when the initial injury was thermal. The stenting also must be left in place for much longer than the usual period.
Lacerations
Lacerations of the punctum are rare, and those to the sac alone can be repaired primarily. The most common form of laceration to the nasolacrimal drainage system is the canalicular laceration. The guiding principle in the repair of the canaliculus is to reestablish the patency of the damaged system. The surgeon should minimize further trauma to the nasolacrimal system and be cognizant of the cosmetic details. Use of the pigtail probe in the repair must be used cautiously because it can too easily damage the sac and common internal punctum. The operating microscope assists in visualization of the lacerated ends and is highly recommended for surgical management. If the surgeon is more comfortable with high-power loupes, use of the operating microscope may be unnecessary. In fact, loupes may be more advantageous because the surgeon may have a greater field of vision and more mobility while repairing the laceration. The proximal or lateral end is located easily by passing a probe through the punctum (Fig. 12A and 12B). The medial or distal end usually can be identified easily with the use of the magnification. When both upper and lower canaliculi are cut near the sac, identification may be difficult. When a single canaliculus is cut, the use of a milky white steroid–antibiotic suspension injected through the intact canaliculus can assist in locating a cut end. Air can be injected in a similar fashion under a pool of saline, and the resultant bubbles can assist in localizing the distal end. The use of the operating microscope under high power has made these maneuvers unnecessary in most cases.
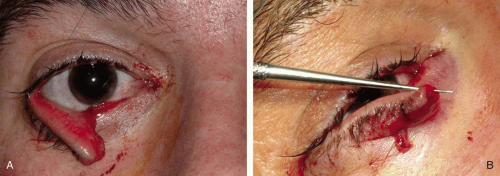 Fig. 12 A and B. Lower canalicular laceration with the distal (lateral) portion identified by a fine punctal dilator. |
Surgical technique for the repair of lid lacerations has evolved to Silastic intubation of the nasolacrimal system.6 Either monocanalicular or bicanalicular stents can be inserted (Fig 13A, B, C, D). The Silastic material moves easily and does not prohibit the lid from blinking normally. The flexibility of the tubing also allows for simpler anastomosis of the lacerated ends of the canaliculus. With Silastic intubation, 7–0 absorbable sutures can be placed submucosally (Fig. 14). The Silastic is placed into the nasolacrimal duct as described for pediatric dacryostenosis, and the canaliculus is repaired around the stent. If the laceration is in the medial canthal tendon area, repair of the deep and superficial heads of the pretarsal muscle should be done.6 The lid can further be supported by a mattress-type suture sling using a 4.0 vicryl on a P2 needle, transnasal wiring, or a supramid suture on a ski needle (Figs. 15 and 16). The orbicularis and skin are closed in layers with appropriate sutures. The Silastic tubing should be left in place for 4 to 6 months, if possible. Lack of epiphora is a positive sign indicating that the tears are passing despite the cicatrix from the laceration. The tears pass around the silastic tube into the nasolacrimal sac and exit from the duct. Unless chronic infection mandates removal, tubing should remain in place until symptoms or epiphora cease. A good rule of thumb is that the closer the laceration is to the punctum, the earlier the tube can be removed.
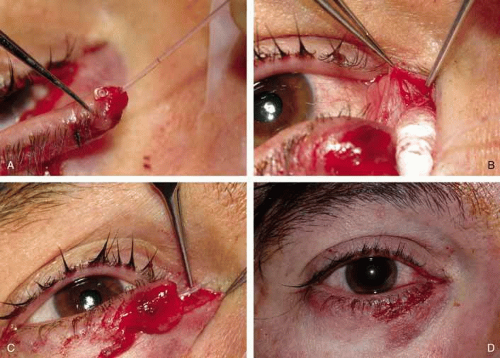 Fig. 13 A–D. Monocanalicular stenting of canalicular laceration from Figure 12 in the office under local. A mini Monaka (FCI Ophthalmics, Marshill Hills, MA) is placed though the lateral portion of the lacerated canaliculus (A). The medial portion of the canaliculus is identified in the area of the canthal tendon (B) and the Silastic stent is fed into the lacrimal sac (C). The final appearance immediately on completion of canalicular and eyelid laceration repair (D). |
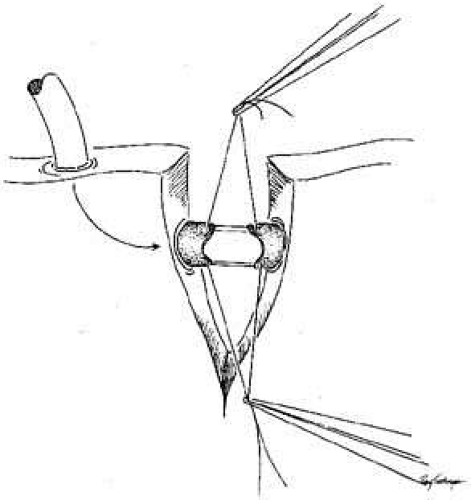 Fig. 14 Repair of canalicular laceration over a Silastic stent. Two to three sutures may be placed submucosally to close the mucosal tear. |
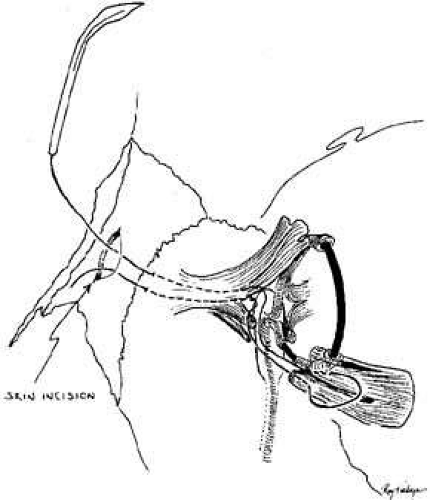 Fig. 15 Reattachment of the medial canthal tendon showing posterior placement of ski needles through the insertion of the heads of the pretarsal orbicularis muscle and running below the periosteum to the insertion of the canthal tendon. |
 Fig. 16 Repair of the laceration. The canthal tendon was reattached with ski needles on the supramid suture. Bicanalicular Silastic tubing was passed through the nasolacrimal duct as for pediatric dacryostenosis. |
We recommend use of the Monaka or mini-Monaka system (FCI Ophthalmics, Marshall Hills, MA) for monocanalicular trauma. The mini-Monaka is an excellent choice for adults repaired under local anesthesia. This short stent has a built in punctal anchor and is more rigid than standard silicone tubing. The stent is first introduced into the lateral portion of the torn canaliculus and seated at the puncta. Once the lateral portion is appropriately placed, the remainder of the stent can be fed medially into the other portion of the canaliculus and down into the sac followed by suturing as above. For children, and those adults requiring sedation, the Monaka monocanalicular stent with a prolene feeder and a Ritleng probe can also be used. The advantage of this system is that traction can be applied to the tubing as it exits the nose thus rotating the lacerated eyelid into the appropriate anatomic position. There are several other methods of monocanalicular intubation mentioned for historic purposes only. A Veirs rod, which is a metal rod bonded onto a silk suture, may bridge the laceration and can be fixed to the lid with the suture.50 A Johnson wire can be placed into the canaliculus to provide a scaffold for repair. The wire can then be sutured onto the lid.51 Long52 devised a lacrimal stent from a silicone tubing attached to a punctal plug. The silicone tube bridges the laceration, which can then be fixed in place with the punctal plug. If both canaliculi are damaged, intubation of the entire lacrimal excretory system is advisable. Lacerations of both canaliculi at or near the common internal punctum are best managed with a DCR and retrograde probing with Silastic intubation, as previously described in the section on congenital abnormalities.
Major Midface Trauma
Fracture to the midface can shear the nasolacrimal duct. Surgical repairs in this region, especially when transnasal wiring is done, may damage the lacrimal sacs or ducts, causing nasolacrimal drainage obstruction. Lacrimal reconstruction in the absence of frank dacryocystitis should be delayed if possible until the major bone work in the orbital region is completed.53 Otherwise, good results may be undone, and subsequent repeat surgery often proves to be challenging. Less than optimal results may ensue (Fig. 17A and 17B and Fig. 18). As an aside, the best approach in these patients is to repair the nasolacrimal system in the acute setting at the same time the fractures are repaired. However, this is often not possible for logistical reasons. If at the time of the fracture repair the nasolacrimal duct is found to be severed, either stening the duct or a DCR should be done.
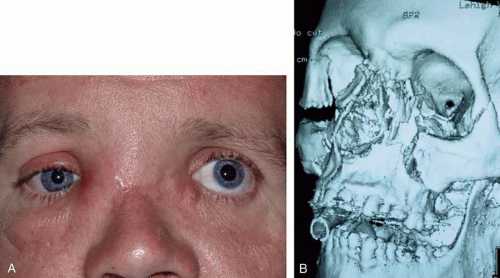 Fig. 17 A and B. Patient with severe midface trauma, facial and orbital fractures status postfracture repair now with bilateral dacryocystitis (A). Comoputed tomography (CT) scan with three-dimensional reconstruction showing initial orbital fractures involving midface and path of nasolacrimal duct (B). |
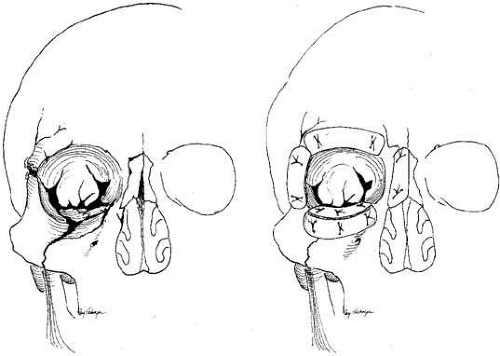 Fig. 18 A. Midfacial fractures can shear the nasolacrimal duct. The orbital contents are freed subperiosteally and elevated by split-thickness rib grafts (B). Nasolacrimal and lid reconstruction should be delayed until this major bone work of the midface is completed and it is certain that additional grafts or orbital shifts will not be required. |
SURGICAL MANAGEMENT
The objective of lacrimal drainage surgery is to establish flow of tears from the cul-de-sac to the nasal cavity. The techniques used in children and adults are virtually the same. There are, however, some specific differences that will be reviewed.
SURGICAL MANAGEMENT OF LOWER SYSTEM BLOCKS
Pediatric Irrigation and Probing Under General Anesthesia
When pediatric general anesthesia is safely available and is selected by a surgeon, a face mask usually will suffice. However, a laryngeal mask is preferred because it is an excellent device that allows free access to the nose for retrieval of dye and irrigated fluids. Furthermore, it maintains the airway, even if it is necessary to perform Silastic intubation of the nasolacrimal system.54 An intravenous drip should be established before the surgeon performs the actual probing and irrigation. Endotracheal intubation should be done if there is any question about the child’s airway. When the child is asleep, careful examination of the canaliculi should be done with gentle dilation of the punctum, as previously described, and careful passage of a lacrimal cannula (blunt 23-gauge cannula) attached to a 3-mL Luer-Lok syringe containing several milliliters of 2% fluorescein solution. The surgeon should feel for veils and strictures in each canaliculus and at the internal common punctum, before attempting to probe the nasolacrimal duct. The surgeon can attempt to use hydraulic pressure irrigation while occluding the opposite punctum as the initial effort to open the lower (distal) portion of the nasolacrimal system. If this maneuver fails, the lacrimal cannula can be used as a probe because it is between a number 0 and a number 00 Bowman probe in size (Fig. 19). After the cannula is shaped into a slight curve, this instrument can be passed gently into the nasolacrimal duct by the upper canaliculus. The lower canaliculus should be manipulated as little as possible. If any resistance is encountered because the cannula is too large, the surgeon should withdraw this instrument immediately and use a smaller Bowman probe. The probing instrument is slipped down into the nasolacrimal duct until it meets resistance at the lower end. The surgeon then should turn the curve of the cannula medially, and with a gentle but firm push, enter the inferior meatus. When the cannula is passed through the duct, any scraping sensation, rather than a smooth, sliding sensation, usually indicates a false passage or the presence of extensive scar tissue. In such instances, the instrument should be withdrawn, and the surgeon should make a gentle attempt to find the normal channel. If passage into the nose is not achieved because of a presumed false passage, it is preferable to stop the procedure and reschedule a probing and irrigation under a general anesthetic several weeks later to allow the operative inflammation to subside. The resolution of inflammation is aided by irrigation with 0.5 mL of an antibiotic steroid solution.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


