Fig. 22.1
Photograph of Seoul-type keratoprosthesis (a, b) Seoul KPro whose skirt is made of polyurethane. (a) Front view. (b) Rear view. (c, d) Seoul KPro whose skirt is made of polypropylene. (c) Front view. (d) Rear view
The potential advantage of Seoul KPro is that it is doubly fixated to the healthy and stable sclera internally and to the cornea externally. Since most prostheses are placed in diseased corneas, the extrusion resulted not only from inadequate corneal healing capacity but also from a deficiency in the compatibility of the keratoprosthesis and surrounding cornea [22]. Scleral fixation might provide strong support for the keratoprosthesis, even in the absence of corneal support. Rabbit experiments have shown the average retention time of the double-fixated Seoul KPro to be longer than that in the single-fixated preliminary design of Seoul KPro [21].
The formation of a retroprosthetic membrane is a common postoperative complication of keratoprosthesis [12, 13, 15]. Those who use long-core prostheses report a lower incidence of retroprosthetic membranes [14]. In order to reduce the formation of a retroprosthetic membrane, the long cylinder-shaped optic was introduced, and the PMMA was treated with a hydrophilic surface poly(ethylene) glycol (PEG) grafting polymerization. The PEGs were grafted to the PMMA of the whole optic and the anterior flange of fluorinated silicone, which improved the hydrophilicity and tear stability on the front surface and reduced the retroprosthetic membrane formation behind the optic [23, 24].
In order to enhance wound adaptation surrounding Seoul KPro, we adopted a porous polymer like e-PTFE, in which the pore size was initially 20 μm. However, no fibrovascular ingrowth was observed in the 20 μm pores of the e-PTFE, and a larger size of e-PTFE was unavailable due to patent issues [25, 26]. Therefore, this study investigated polyurethane (0.4 mm thick, 40 μm pore size) as a skirt material and applied it to the second-generation Seoul KPro. Animal studies showed good adaptation of the wound and marked fibrovascular invasion into the polyurethane of the second-generation Seoul KPro [25, 26]. However, a long-term follow-up of more than 2 years in human clinical trials showed the polyurethane to be degenerated [27]. Finally, it was found that the nonwoven fabric of polypropylene was nondegradable and presented good invasion of fibrovascular tissues [27]. A human clinical trial also displayed no degradation of nonwoven polypropylene until 3 years after surgery. Consequently, it was used as a skirt for the third-generation Seoul KPro.
22.3 Clinical Indications and Contraindications
22.3.1 Indications
Seoul KPro has been used for the advanced stages of Stevens-Johnson syndrome, ocular chemical burn, ocular cicatricial pemphigoid, other autoimmune diseases, and other intractable ocular surface conditions with poor prognosis using traditional penetrating keratoplasty accompanied by limbal transplantation. Seoul KPro is also considered in cases of repeated failures of limbal transplantation with penetrating keratoplasty.
22.3.2 Contraindications
Seoul KPro is not recommended in a patient with repeated central graft failures or herpes keratitis if the limbus is intact. Seoul KPro must not be chosen as a first treatment option in subjects who can be amended by conventional penetrating keratoplasty.
22.4 Surgical Techniques
The surgical procedures are as follows (Video 22.1 attached): The pupil is dilated prior to surgery, and 360° of conjunctival peritomy is performed and the conjunctiva is recessed to expose the sclera. The abnormal fibrovascular tissues on the cornea are extensively removed. A Flieringa fixation ring (Storz, USA) is fixed with 6-0 black silk (Ethicon, Johnson & Johnson, USA) 2 mm away from the limbus. Half-thickness corneal trephination, 6 mm in diameter, is performed with a Barron trephine (Katena, USA), and a 360° intralamellar dissection is performed with a disposable crescent blade (Becton, Dickinson and Company, USA) to make an intrastromal pocket, 2 mm in length (Fig. 22.2a). After excising the trephinated central cornea, capsulorrhexis of the lens capsule is performed, and the nucleus is removed. The residual cortex, posterior capsule, and a part of the anterior vitreous are removed using a vitreous cutter, and a sector iridectomy is then performed. The Seoul KPro is placed into an eyeball after tying 10-0 polypropylene sutures (Ethicon, Johnson & Johnson, USA) of both haptics (Fig. 22.2b) and then 10-0 polypropylene sutures go through each side of the sclera from inside out at 3 mm away from the limbus (ab interno technique, Fig. 22.2c) and are temporarily tied. The skirt is inserted into the previously prepared corneal pocket (Fig. 22.2d), and the polypropylene sutures of the haptics are permanently tightened to the sclera (Fig. 22.2e) when the intraocular pressure of the eyeball is normalized with 4–8 cardinal 10-0 nylon interrupted sutures. The skirt is fixed completely with additional 10-0 nylon interrupted sutures (Fig. 22.2f). A cryopreserved human amniotic membrane is placed over the entire cornea including the prosthesis and secured with the conjunctival edges using 10-0 nylon to reduce inflammation and to enhance epithelization of the wound (Fig. 22.2g). To enhance the early stabilization of the surgical wound after Seoul KPro implantation by suppressing matrix metalloproteinase (MMP)-9 expressions, cultivated autologous oral mucosal epithelial sheet can be transplanted instead of amniotic membrane transplantation [28].
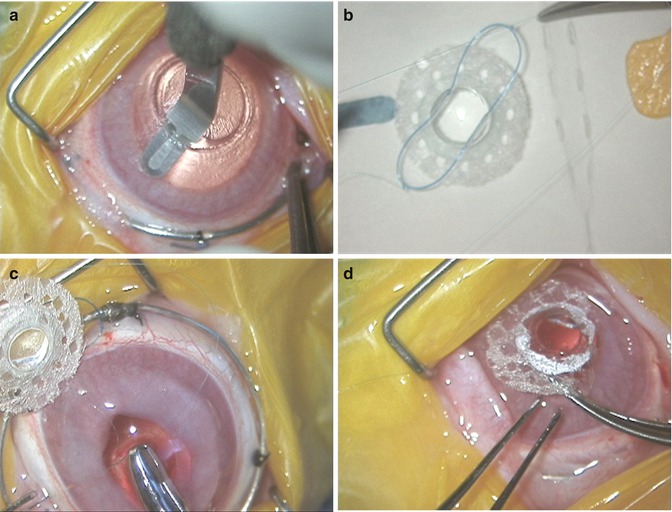
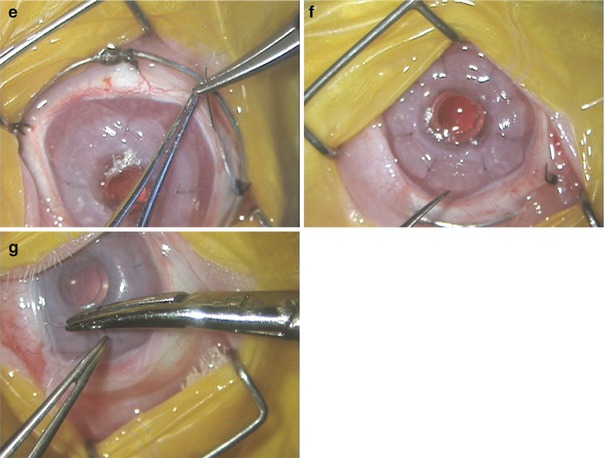
Fig. 22.2
Surgical procedures used for implanting the Seoul KPro. Specially made Seoul KPro was used in animal experiments just for demonstration (the material property was the same as that used in the clinical trial, except that the brown color was not added to the anterior flange of the fluorinated silicone). (a) An intrastromal pocket, 2 mm in length, was made with a disposable crescent blade. (b) Each haptic of the Seoul KPro was sutured using 10-0 polypropylene (Ethicon, Johnson & Johnson, USA, 788G). (c) Each haptic of the Seoul KPro was anchored transclerally (ab interno technique) 1 mm posterior to the limbus in the rabbit eye (or at 3 mm posterior to the limbus in the human eye). (d) The skirt was inserted into the previously prepared corneal pocket. (e) Polypropylene sutures were fixed to the sclera after the intraocular pressure was normalized by 4 cardinal fixating sutures of the skirt. (f) The skirt was fixed completely to the cornea using additional 4–8 interrupted sutures with 10-0 nylon. (g) Cryopreserved human amniotic membrane was placed over the entire cornea using 10-0 nylon sutures
At the end of the operation, 20 mg of gentamicin sulfate and 20 mg of dexamethasone sodium phosphate are injected subconjunctivally.A temporary tarsorrhaphy is performed in the lateral third of both lids with 6-0 black silk (Ethicon, Johnson & Johnson, USA) for 1–2 weeks.
22.5 Brief Outcome of Clinical Trials
We reported the preliminary results of the Seoul KPro-implanted eyes of the first seven human cases [29]. Five of the enrolled patients were diagnosed with Stevens-Johnson syndrome, one with a chemical burn and the other suffered from an ocular cicatricial pemphigoid. All patients failed to restore their visual acuity by repeated penetrating keratoplasties before Seoul KPro implantation. 85.7 % of the anatomical success was achieved, and visual rehabilitation was supported by Seoul KPro implantation during an average follow-up of 25.6 months (Fig. 22.3a–f) [29]. We also presented the outcome of long-term follow-up in nine patients [30]. The Seoul KPro showed good anatomical success in 66.7 % for an average of 62.8 months, and the average visual acuity rehabilitation time was 31.6 months [30].




