The primary objectives of management of chronic otitis media with and without cholesteatoma include (1) elimination of infection or cholesteatoma; (2) prevention of recurrent disease; and (3) reconstruction of the tympanic membrane and ossicular chain to minimize the postoperative air bone gap. As judged by published success rates in achieving a dry, safe ear over time and in reconstruction of the middle ear, surgical management of the chronic ear remains one of the more challenging disease processes in otology. In chronic otitis media with cholesteatoma, combined rates of either residual or recurrent cholesteatoma occur in up to 50% of patients.1–3 In general, most series suggest a lower recidivism rate for cholesteatoma in cases managed by canal wall-down technique as compared with canal wall-up.3–6 However, even without recurrent cholesteatoma, the canal wall-down technique appears to predispose the patient to persistent or recurrent intermittent drainage requiring revision surgery7–9 in up to 60% of cases. Hearing results have been likewise disappointing in chronic otitis media as compared with other middle ear reconstructive problems. Thus, postoperative air bone gaps <20 dB were reported in 38%,10 and >30 dB in 30%.11 In 400 second-stage procedures of chronic otitis media, closure of the air bone gap to <20 dB occurred in 68% of patients with intact stapes. In general, postoperative air bone gaps are even larger when the stapes superstructure is not intact.5,12–14 Although some authors a priori prefer either the canal wall-up technique2, 15 or canal wall-down technique,16 it is this author’s opinion that each case should be individualized to minimize recurrence of disease. Factors Involved in Treatment Algorithm for Chronic Otitis Media INITIAL EVALUATION The initial evaluation of patients with chronic otitis media should include a thorough otologic and general medical history. The otologic history must include careful documentation of symptoms and previous treatment, both medical and surgical. The general medical history should include documentation of potential predisposing factors including upper respiratory allergy, smoking, diabetes mellitus, and possible immunologic compromise. Examination should include a thorough otologic and complete head and neck examination. Audiometry is essential. Bacteriologic cultures, including anaerobes in cases of chronic otitis media with otorrhea may be helpful. Computed tomography (CT) of the temporal bones, in both the axial and coronal planes, will provide valuable information concerning pneumatization of the mastoid, extent of cholesteatoma and granulation tissue, potential complications such as dehiscence of a semicircular canal or the facial nerve, or unexpected findings such as extension of disease to the petrous apex. In chronic otitis media with impending complications, CT is particularly useful. CATEGORIZATION OF CHRONIC OTITIS MEDIA As part of the initial evaluation of the patient with chronic otitis media, an attempt should be made to assign the disease process to one of the categories shown in Table 38-1. In the author’s hands, such subcategorization of disease will suggest a management strategy selected from a medical and/or surgical algorithm. Failure to control chronic otitis media can be attributed to the improper selection of a medical or surgical strategy at least as often as inadequate execution of that procedure. REVIEW OF ALGORITHM FOR MANAGEMENT OF PRIMARY CHRONIC OTITIS MEDIA After initial evaluation, including ancillary studies and assignment to a subcategory of disease (Table 38-1), possible contributory disease processes such as allergic rhinosinusitis, smoking, obesity and/or diabetes mellitus, immunocompromise, should be assessed and controlled if possible (Fig. 38–1). Chronic otitis media with cholesteatoma almost always requires surgical intervention. In those cases without otorrhea, surgery may be limited to the removal of cholesteatoma and reconstruction of the ossicular chain and tympanic membrane. However, in those with otorrhea, even with limited cholesteatoma, a complete tympanomastoidectomy, either canal wall-up or canal wall-down, should be performed. For example, chronic active otitis media with cholesteatoma limited to the attic with no history of otorrhea may be managed successfully with atticotomy and reconstruction without mastoidectomy, whereas chronic active otitis media with cholesteatoma, limited to the attic, but with a history of recurrent or chronic infection, mandates mastoidectomy as well as atticotomy. Similarly, chronic inactive otitis media without frequent reactivation represents an elective surgical candidacy for reconstruction of the tympanic membrane and ossicles and does not require mastoidectomy. By contrast, chronic inactive otitis media with frequent reactivation, that is spontaneous recurrent otorrhea after adequate medical management, generally requires rnastoidectomy. In many of these cases, the recurrent otorrhea may be explained by obstruction of the aditus ad antrum and sequestration of the mastoid air space by –aditus block.”17
| Chronic active otitis media With cholesteatoma With otorrhea Without otorrhea Without cholesteatoma With otorrhea Chronic inactive otitis media With frequent reactivation Without frequent reactivation |
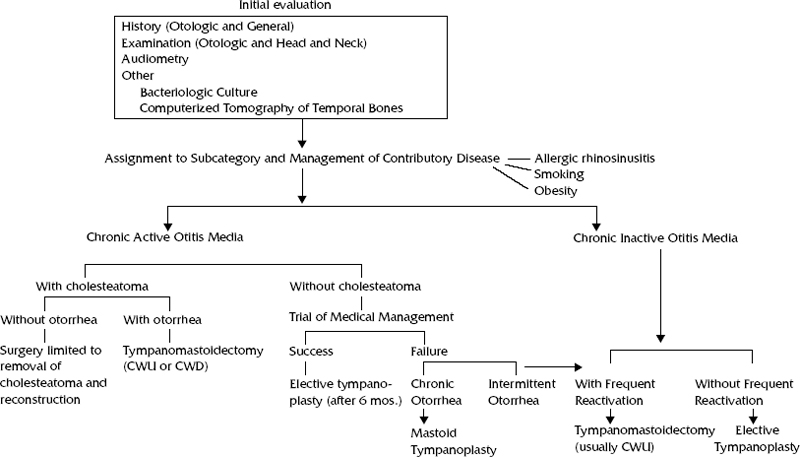
Figure 38-1 Algorithm for management of primary chronic otitis media. CWU, canal wall-up; CWD, canal wall-down.
In those cases with chronic active otitis media without cholesteatoma, a trial of medical management should be undertaken. This includes management of potential contributing diseases, and knowledge of the bacteriology of the suppuration. In most patients in whom otorrhea has stopped for at least 6 months, elective tympanoplasty and ossiculoplasty may be considered. For those who fail medical management, those with persistent chronic suppuration should undergo tympanomastoidectomy. Cases in which the suppuration temporarily clears only to recur promptly after cessation of medical management should be reassigned to the category –chronic inactive otitis media with frequent reactivation.”
FACTORS AFFECTING CHOICE OF CANAL WALL-UP OR CANAL WALL-DOWN APPROACH
The selection of the canal wall-up versus the canal wall-down approach should be individualized based on the experience of the surgeon and details of the clinical variables of the case in question. Examples of preoperative clinical variables that frequently have an influence on this decision are shown in Table 38-2. For example, a very poorly pneumatized mastoid as determined by preoperative physical examination and imaging is a relatively negative indicator for the canal wall-up approach. Similarly, a unilateral nonhearing ear (dead ear) with chronic otitis media, is a good candidate for canal wall-down surgery and tympanomastoid obliteration. In patients who have had multiple previous procedures, particularly those in whom the canal has been partially or totally removed, I prefer the canal wall-down technique with mastoid obliteration. Individuals with bilateral longstanding chronic otitis media are generally managed by canal wall-down technique.
Intraoperative findings that will suggest selection of the canal wall-down technique include inadequate surgical access with preservation of the canal wall, extensive cholesteatoma, and the presence of complications such as facial paresis or labyrinthine fistula.



