(1)
Department of Ophthalmology and Visual Sciences, University of Iowa Hospitals and Clinics, Iowa City, IA, USA
Ischemic optic neuropathy is one of the major causes of blindness or seriously impaired vision, yet there is disagreement as to its pathogenesis, clinical features, and especially its management. I have conducted basic, experimental, and clinical studies on it since 1955. From these studies, I discussed at length various basic and clinical aspects of ischemic optic neuropathy recently in my book entitled Ischemic Optic Neuropathies [1]. The following is a brief summary.
Terminology
A scientifically valid term is essential to describing a clinical entity. It should reflect the true nature of the disease. Before 1974, ischemic optic neuropathy was described under multiple eponyms [2]. The generic term “ischemic optic neuropathy,” which is widely used, is inadequate, as is evident from the following discussion: On the basis of blood supply, the optic nerve can be divided into two distinct regions: (1) the anterior part (optic nerve head), which is supplied primarily by the posterior ciliary artery (PCA) circulation, and (2) the rest of the optic nerve, which is not supplied by the PCAs but from multiple sources (Fig. 19.1) [3–7]. In the early 1970s, I found from my studies on the blood supply of the optic nerve [4–6], and experimental [9] and clinical [10, 11] studies, that interference with the PCA circulation resulted in the clinical picture for which I coined the term “anterior ischemic optic neuropathy – AION” [12]. This term represents the exact site and ischemic nature of the lesion in the optic nerve. Later, in 1981, I was the first to describe the clinical entity “posterior ischemic optic neuropathy” [13], which is due to ischemia of a segment of the posterior part of the optic nerve, not supplied by the PCA (Fig. 19.1).
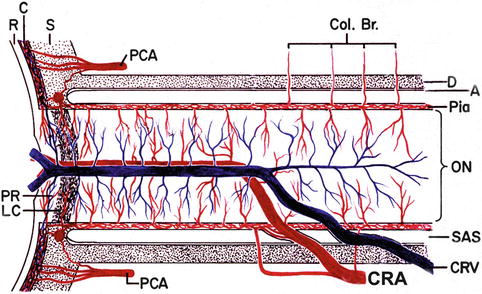
Fig. 19.1
Schematic representation of blood supply of the optic nerve (Modified from Hayreh [8]). A arachnoid, C choroid, CRA central retinal artery, Col. Br. collateral branches, CRV central retinal vein, D dura, LC lamina cribrosa, ON optic nerve, PCA posterior ciliary artery, PR prelaminar region, R retina, S sclera, SAS subarachnoid space
Ischemic optic neuropathy is not one disease but a spectrum of several different types, each with its own etiology, pathogenesis, clinical features, and management. The following is a brief account.
Classification of Ischemic Optic Neuropathy
Ischemic optic neuropathy is of two distinct types:
Anterior Ischemic Optic Neuropathy (AION)
This is due to ischemia of the optic nerve head. Etiologically and pathogenetically, AION is of two types [10, 14–16].
1.
Arteritic AION (A-AION): This is due to giant cell arteritis (GCA).
2.
Non-arteritic AION (NA-AION): This type is not due to GCA. It comprises the following two types:
(a)
Classical NA-AION
(b)
Incipient NA-AION
Posterior Ischemic Optic Neuropathy (PION) [13]
This is due to the involvement of the rest of the optic nerve. Etiologically, PION can be classified into three types:
1.
Arteritic PION: This is due to GCA.
2.
Non-arteritic PION: This is due to causes other than GCA.
3.
Surgical PION: This is a complication of non-ophthalmic surgical procedures.
Thus, ischemic optic neuropathy actually comprises six distinct clinical entities. AION is by far the most common and one of the most prevalent and visually crippling diseases in the middle aged and elderly. A-AION, though less common, is an ocular emergency and requires early diagnosis and immediate treatment with systemic high-dose corticosteroids to prevent further visual loss, which is entirely preventable.
Since ischemic optic neuropathy is an ischemic disorder of the optic nerve, the first basic requirement is a good understanding of the blood supply of the optic nerve and the role of various factors in the production of acute optic nerve ischemia.
Relative Frequency of Various Types of Ischemic Optic Neuropathy
I analyzed this in all the patients with ischemic optic neuropathies seen in my clinic from 1973 to 2008 – about 1,400 patients in all. I analyzed the relative frequency of the various types of ischemic optic neuropathy among this cohort [1]. The relative frequencies of AION and PION were 96 and 4 %, respectively. Since PION is a diagnosis of exclusion [13], however, it may sometimes have been missed, so that the frequency I found may be a slight underestimate.
Anterior Ischemic Optic Neuropathy
The total number of patients seen in my clinic with this condition was about 1,350. Of those, about 90 % had non-arteritic anterior ischemic optic neuropathy (NA-AION) and 10 % arteritic anterior ischemic optic neuropathy.
Posterior Ischemic Optic Neuropathy
There were about 50 patients. Of those, about 66 % had non-arteritic PION, 26 % arteritic PION, and 7 % surgical PION. This depends upon the referral pattern.
Of course, the relative proportion of the various types of ischemic optic neuropathy will vary among different clinics, depending upon the total number of patients seen and the type of practice, but the above data provides a useful general guide.
Investigations in Patients with Ischemic Optic Neuropathy
Apart from a detailed history and comprehensive ophthalmic evaluation, patients with AION should have the following investigations to find the cause and to prevent or reduce the risk of any further visual problems.
Fluorescein Fundus Angiography
I have always performed fluorescein angiography (normally stereoscopic) regularly in all eyes with AION. It provides important and useful information when performed during the initial stages of the disease. The telltale impaired circulation and its location in AION are seen on angiography only during early stages of the disease and during the very early retinal arterial phase of dye filling in the fundus. In my clinical studies on AION, angiography has provided crucial information about its pathogenesis as well as the differential diagnosis of arteritic from NA-AION. In eyes with arteritic AION, there is PCA occlusion caused by GCA; angiography shows absent filling of the choroid and the optic disc in the distribution of the occluded PCA (Fig. 19.2). No such filling defect is seen in NA-AION, where there is usually delayed filling of the peripapillary choroid, unless NA-AION is due to embolic occlusion of the PCA. It is most unfortunate that this extremely useful and readily available test is not used by neuro-ophthalmologists as often as it should be for the evaluation of AION. Many NA-AION patients who consult me, having previously seen neurologists/neuro-ophthalmologists, come with records of extensive investigations, including computerized tomography, magnetic resonance imaging, and/or magnetic resonance angiography ordered by the neurologists/neuro-ophthalmologists, showing no abnormality at all. I have also seen patients who lost vision in one eye due to occult GCA and had multiple neuroradiological evaluations done by neurologists/neuro-ophthalmologists, when fluorescein angiography would have immediately provided a definite diagnosis; delay in some of these cases resulted in bilateral complete blindness which could have been entirely prevented. I have found over the past four decades of dealing with AION that fluorescein angiography provides much more useful information in evaluation of AION than neuroradiological evaluations which rarely reveal any abnormality. Fluorescein angiography is also much cheaper than those neuroradiological evaluations, yet it is rarely performed.
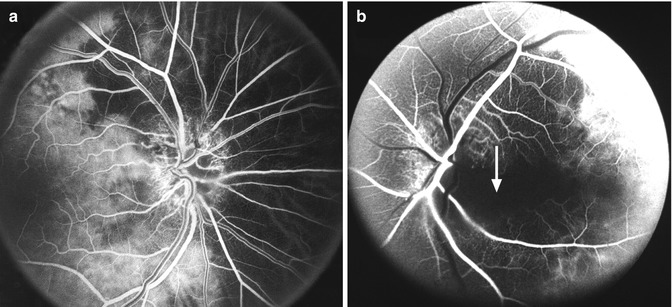
Fig. 19.2
Fluorescein fundus angiograms of two eyes show areas of supply by the occluded PCA and the patent PCA. (a) Right eye with arteritic AION shows normal filling of the area supplied by the lateral PCA (including the temporal ¼ of the optic disc) but no filling of the area supplied by the medial PCA (including the nasal ¾ of the disc) (Reproduced from Hayreh [1]). (b) Left eye with arteritic AION associated with cilioretinal artery occlusion shows normal filling of the area supplied by the lateral PCA, but no filling of the choroid and entire optic disc supplied by the medial PCA or of the cilioretinal artery (arrow) (Reproduced from Hayreh [1])
Hematologic Evaluation
I routinely do the following hematologic evaluations in all patients first seen with visual loss.
Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP) Testing
This is done regularly at the initial visit in all AION, PION, and retinal arterial occlusion patients aged 50 years or older. Testing for ESR and CRP is crucial for all these patients, without any exception, to rule out GCA, since that is an ophthalmic emergency and its early detection and immediate intensive high-dose corticosteroid therapy can prevent visual loss. I receive the result of both tests in 1–1½ h. My patients do not leave the clinic till I have the results of both ESR and CRP available to make sure no patient with GCA is missed.
Fasting Lipid Profile and Glucose Evaluation
This is performed on a subsequent follow-up visit, or as soon as possible. Hyperlipidemia is a risk factor for NA-AION [17].
I see no point in doing detailed thrombophilic testing in patients with NA-AION since it is not a thrombotic disorder but a hypotensive disorder (see below).
Temporal Artery Biopsy
This is done when a diagnosis of arteritic AION is suspected from clinical findings or GCA is suspected from the elevated ESR and CRP and other clinical findings. The use of temporal artery biopsy in GCA is discussed at length elsewhere [18, 19]. In patients suspected to have GCA, there is no urgency to do a temporal artery biopsy immediately; rather an immediate start of the treatment with high-dose corticosteroid therapy is most critical in these cases to prevent any visual loss. Corticosteroid therapy does not alter the outcome of a temporal artery biopsy [19, 20]. To wait for a temporal artery biopsy result before starting corticosteroid therapy may lose precious time and result in permanent visual loss which is quite preventable; therefore, my advice always has been not to wait for the temporal artery biopsy result to start the corticosteroid therapy. I do not recommend doing temporal artery biopsy on both sides at the same time – after all, temporal artery biopsy is not a benign procedure and I have seen scalp necrosis following this practice. To get reliable information from a temporal artery biopsy, it is essential to keep the following two important considerations in mind: (1) there should be at least a one inch piece of temporal artery, and (2) the artery must be serially sectioned. For example, in one of my cases, only 1 of about 300 sections showed definite evidence of GCA.
Systemic Evaluation
If the diagnosis of AION or PION is definite, then the patient requires complete systemic evaluation because both NA-AION and PION are multifactorial in nature, with systemic risk factors playing a role in their development. This includes evaluation for various risk factors, including diabetes mellitus, hyperlipidemia, arterial hypertension, arterial hypotension, collagen vascular diseases, sleep apnea, and other possible risk factors, depending upon a patient’s health status. Information about these risk factors is essential to the management of NA-AION and non-arteritic PION. I advise all patients to have a complete physical checkup.
Non-arteritic Anterior Ischemic Optic Neuropathy (NA-AION)
This is the most common type of ischemic optic neuropathy and has attracted the most controversy as to its pathogenesis and management. I have discussed this at length in my book Ischemic Optic Neuropathies [1]. The following is a brief summary.
There are three major misconceptions about NA-AION: (1) that its pathogenesis is not known; (2) that NA-AION and ischemic cerebral stroke are similar in nature, pathogenetically, and in management; and (3) that there is no treatment [21]. The following is a discussion of these and other issues on NA-AION.
Pathogenesis
Briefly, NA-AION is due to acute ischemia of the optic nerve head, and it is a multifactorial disease. This means many risk factors play roles in its development, and there is no one culprit which causes it. Various risk factors can be divided into two main categories: (1) predisposing and (2) precipitating risk factor(s) [17].
Predisposing Risk Factors
These may be systemic or local, in the optic nerve head itself.
Systemic Risk Factors
Various studies have shown a significantly high prevalence of arterial hypertension, nocturnal arterial hypotension, diabetes mellitus, ischemic heart disease, hyperlipidemia, atherosclerosis, and arteriosclerosis in NA-AION patients compared to the general population [17, 22–25]. Other associated systemic diseases have also been reported, including sleep apnea [27–30], arterial hypotension due to a variety of causes including shock, cardiopulmonary bypass surgery and hemodialysis, and massive or recurrent hemorrhages [31]; and malignant arterial hypertension [32]. The possibility that in an occasional patient embolism from thrombophilic factors may cause NA-AION cannot be ruled out [33]. Similarly, other rare causes include migraine, defective cardiovascular autoregulation, “Type A personality” [27], carotid dissection [34], and embolism [35]. In addition, the literature is full of anecdotal case reports of the association of “anterior ischemic optic neuropathy” with a large variety of systemic diseases and causes, but it is not possible to establish a cause-and-effect relationship in all of them. However, these rare diseases have no role in the vast majority of NA-AION cases, since it is primarily a hypotensive disorder, as discussed below.
Ocular and Optic Nerve Head Risk Factors
A significant association of NA-AION has been seen with a number of ocular and optic nerve head conditions. These include absent or small cup in the optic disc [36, 37], angle closure glaucoma or other causes of markedly raised IOP [38], marked optic disc edema due to any cause [39], location of the watershed zone of the PCAs in relation to the optic disc [40], vascular disorders in the nutrient vessels of the ONH [6], optic disc drusen, and cataract extraction [38]. There are a few reports of delayed development of NA-AION in the fellow eyes long after cataract extraction in one eye [41, 42], implying that cataract extraction per se is a risk factor; there is no evidence in support of that. A person who has the required risk factors is at risk of developing NA-AION in either eye, irrespective of whether he/she has cataract extraction or not. Optic disc-related visual field defects detected after vitrectomy [43] are most probably due to development of NA-AION in those eyes during vitrectomy and due to intra- and/or postoperative raised IOP, along with other associated systemic risk factors mentioned above.
Time of Onset of NA-AION
This Provides Important Information About the Pathogenesis
My study [44] showed that of 925 episodes of NA-AION, 73 % of patients gave a history, when specifically asked, of discovering their visual loss on awakening from sleep in the morning or from a nap or at the first opportunity in the day to use their vision critically. The incidence may actually be much higher than 73 % because other patients, who first became aware of their visual loss later in the day, could not be certain when it had first occurred, nor could they rule out the possibility that it had been there since awakening [44].
I did 24-h ambulatory blood pressure monitoring studies, recording blood pressure every 10 min during waking hours and every 20 min during sleeping hours in about 700 patients [45, 46]. Those revealed that, while blood pressure may be perfectly normal during the day, it drops during sleep – much more in some persons than in others. Figure 19.3 shows the 24-h ambulatory blood pressure monitoring graph of a patient who developed NA-AION, first in one eye and later in the second. It shows that during her waking hours, her blood pressure was within normal limits, but soon after going to sleep, her systolic blood pressure fell from 140 to 90 mmHg and diastolic from about 80 mmHg to about 50 mmHg. Her blood pressure was low throughout her sleeping hours. This is nocturnal arterial hypotension. My 24-h ambulatory blood pressure monitoring studies showed that daytime blood pressure is not at all a guide to the blood pressure during sleep, as can be seen in Fig. 19.3. Unfortunately, most of the information on blood pressure is based on daytime recording.
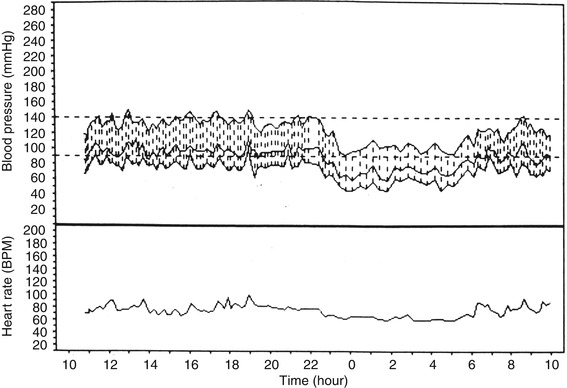
Fig. 19.3
Ambulatory blood pressure monitoring records (based on individual readings) over a 24-h period, starting from about 11 AM, in a 58-year-old woman with NA-AION first in one eye and later on in the second eye and on no medication. The blood pressure is perfectly normal during the waking hours but there is marked nocturnal arterial hypotension during sleep (Reproduced from Hayreh et al. [46])
Nocturnal Arterial Hypotension
A certain amount of fall of blood pressure during sleep is physiological, but it can be aggravated by medication, most commonly by aggressive antihypertensive therapy with beta-blockers, calcium channel blockers, angiotensin converting enzyme inhibitors, and other hypotensive drugs, especially when those are taken at bedtime or in the evening [24, 44–46]. Figure 19.4 demonstrates that very well. This patient was taking verapamil (a calcium channel blocker) three times a day (160 mg morning and bedtime and 80 mg noon) for migraine; with that the systolic blood pressure dropped from about 130 mmHg during waking hours to as low as about 80 mmHg during sleep, and diastolic blood pressure dropped from about 70 mmHg during the day to as low as about 40 mmHg during sleep. On stopping the bedtime dose, there was a marked decrease in the fall of blood pressure during sleep. Nocturnal arterial hypotension can occasionally develop without any such medication, as was the case shown in Fig. 19.3; this is most probably due to defective cardiovascular autoregulation.
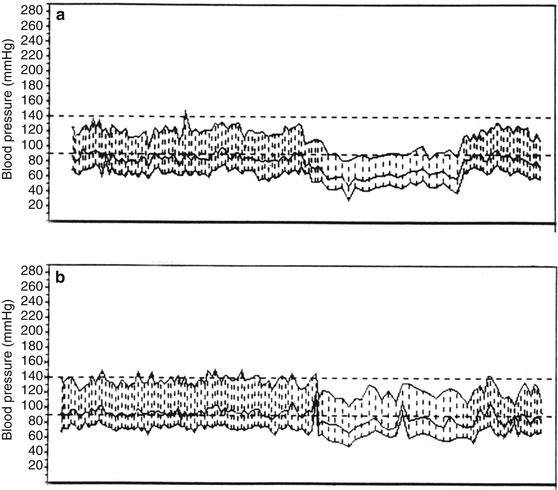
Fig. 19.4
Two 24-h ambulatory blood pressure monitoring records (based on individual readings), starting at 10 AM, of a 63-year-old woman taking verapamil hydrochloride (a calcium channel blocker) 3 times a day for migraine. Both records show normal blood pressure during the waking hours. (a) This shows when she was taking verapamil at bedtime; during sleep there was a marked degree of nocturnal arterial hypotension (blood pressure falling as low as 80/30 mmHg). (b) This shows markedly less nocturnal arterial hypotension on stopping the bedtime dose of verapamil (lowest blood pressure 110/50 mmHg) (Reproduced from Hayreh et al. [46])
It is notable that before 1960, that is, before the advent of beta-blockers and other potent modern blood-pressure-lowering drugs, NA-AION was an uncommon disease. Now, as potent antihypertensive drugs are frequently prescribed by physicians, NA-AION has become common, indicating the likelihood that they may be playing a role in its increased incidence.
In persons with predisposing risk factors, precipitating factors then act as the final insult and produce NA-AION. As discussed above, in the vast majority, visual loss develops during sleep [44]. This indicates that nocturnal arterial hypotension is the most common precipitating risk factor. In view of all this information, we can say confidently that NA-AION is a hypotensive disorder. It is due to transient nonperfusion or hypoperfusion of the blood vessels in the optic nerve head during sleep, and not due to occlusion of the PCAs as often stated. Fluorescein fundus angiography provides the best proof of that, as shown by Fig. 19.5.
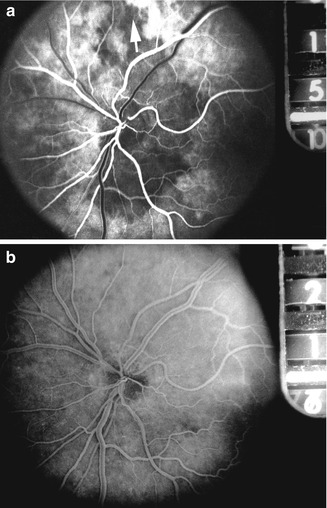
Fig. 19.5
Two fluorescein fundus angiograms at 6-s interval in a patient with NA-AION. (a) During the retinal arterial phase of the dye circulation (15 s after the injection of fluorescein), it shows no filling of the temporal, superior, and inferior peripapillary choroid and superior choroidal watershed zone (arrow) and the optic disc, with normal filling of both the medial and lateral posterior ciliary arteries. (b) During the retinal arteriovenous phase of the dye circulation (21 s after the injection of fluorescein), there is complete filling of the peripapillary choroid (main source of blood supply to the optic nerve head) and the watershed zone and no filling of the optic disc in the area of NA-AION (Reproduced from Hayreh [1])
The argument put forward by those who doubt the role of nocturnal arterial hypotension in the pathogenesis of NA-AION and the hypotensive nature of NA-AION is that in the prospective NA-AION Multicenter Decompression Trial Study [47], only 42 % of the 418 patients reported the onset of visual loss within 2 h of awakening. This is in sharp contrast to the findings of my prospective study [44] where, as mentioned above, 73 % of patients gave a definite history, when specifically asked, of discovering their visual loss on awakening in the morning or from a nap or at the first opportunity in the day to use their vision critically (the rest were not sure of the time). The findings of these two prospective studies do conflict, and that has resulted in controversy on the important concept of the hypotensive nature of NA-AION. However, study design determines the quality of the data. The accuracy of this historical information can be largely influenced by: (1) the expertise of the person asking the questions and (2) the manner in which the patient is asked about when his/her visual loss was first noticed and the circumstances of how he/she became aware of it. In my study [44], I personally collected the historical information from each patient with NA-AION and learned that the accuracy of a patient’s recall depends upon non-suggestive, unbiased, yet thorough questioning. Often the patient needs to be made aware of the importance of their recollection of their discovery of visual loss. In the NA-AION Multicenter Decompression study [47], historical information was collected by many individuals (of different levels of expertise) at different study sites, by necessity, and may not be as rigorous as in my study. It is more challenging in such a heterogeneous study to collect such historical information methodically, uniformly, and reliably, so as to reach an accurate estimate of the true proportion of patients whose visual loss occurred soon after awakening. Estimates of visual loss on awakening may be largely underestimated if based on primarily what the patients volunteer rather than the answers to specific, directed questioning. Moreover, the criterion used in that study of onset of visual loss occurring “within 2 h of awakening” was not valid, because the answer depends upon when the patients first tried to use their vision critically during the day. I think that explains the discrepancy between my study [44] and that of the NA-AION Multicenter Decompression Trial Study [47].
In conclusion, the pathogenesis of NA-AION is known, but it is highly complex. It is multifactorial in nature. Whole hosts of systemic and local risk factors, acting in different combinations, predispose an optic nerve head to develop NA-AION. There are serious confounding factors in determining risk factors for NA-AION; those are discussed in detail elsewhere [48]. One of the arguments often put forward by those who believe the pathogenesis of NA-AION is not yet known is that some patients with NA-AION seem perfectly healthy, with no apparent risk factors. The inability to pinpoint a risk factor may be due to several reasons (discussed elsewhere [48]). Thus, the axiom should be that just because one does not find any evident risk factor, that does not necessarily mean that it does not exist.
NA-AION and Ischemic Cerebral Stroke
One of the major sources of controversy on the pathogenesis and management of NA-AION stems from the almost universal belief that NA-AION and ischemic cerebral stroke are similar in nature pathogenetically and in management. As discussed above, NA-AION is a hypotensive disorder in the majority of cases and only very rarely a thromboembolic disorder. Ischemic cerebral stroke, on the other hand, is usually a thromboembolic disorder and occasionally hypotensive. This is further supported by two large studies [49, 50], which showed that aspirin, which is effective in ischemic cerebral stroke, has no beneficial effect in NA-AION. Thus, it is a fundamental mistake to equate the pathogeneses of the two conditions and their implications for the management of NA-AION. I have discussed this subject at length elsewhere [51].
Clinical Features of Classical NA-AION
NA-AION usually has classical symptoms and signs which make it easy to diagnose. The subject is discussed at length elsewhere [1]. Briefly, it is as follows.
Incidence of NA-AION
A population-based study in the state of Missouri and Los Angeles County, California, USA, found that among persons 50 or older the estimated mean annual incidence rate of NA-AION was 2.30 per 100,000 population, and it was significantly higher among white individuals than blacks or Hispanics [52]. Another epidemiological study in the population of Olmsted County, Minnesota, USA, in persons 50 and older, reported the incidence of NA-AION as 10.2 per 100,000 individuals [53]. Such a large discrepancy between the two studies indicates the problems of obtaining reliable information and the differing ethnic nature of populations since the latter study was based mostly on Caucasians.
Age, Gender, and Racial Features
NA-AION is mostly a disease of the middle-aged and elderly, although no age is immune to it. In a study of 624 patients with NA-AION, mean + SD age was 61.0 + 12.3 SD, range 18–100 years, with 11 % in young (<45 years), 49 % in middle aged (45–64 years), and 40 % in the elderly (≥65 years) persons [54]. In another study of 727 consecutive patients with NA-AION, 23 % were younger than 50 years (median 43 years; range, 13–49 years) [55]. Thus, the prevalent impression that NA-AION is a disease only of the elderly is not correct – no age is immune. It is seen somewhat more often in men than in women – in one study the ratio was 59 % versus 41 % [54] and in another study 58 % versus 42 % [55]. This would be in keeping with the greater prevalence of cardiovascular diseases among men than women. It is apparently far more common among the white population than in other racial groups [52, 54, 55] but that may be misleading for a variety of reasons.
Symptoms
In the vast majority, these are typical. There is a sudden and painless deterioration of vision, usually discovered on waking in the morning [44]. Progressive visual deterioration in some eyes with NA-AION is well known; in them, again, patients usually notice it on waking in the morning. Some patients may complain of intermittent blurring of vision when the visual field defect passes through the fixation point, because of unconscious shifting of fixation between the seeing and the blind areas near the fixation (Fig. 19.6). NA-AION patients often complain of loss of vision toward the nose and less commonly altitudinal loss. Later on, photophobia is a common complaint, particularly in bilateral cases. Some patients may complain of simultaneous onset of visual loss in both eyes; however, I found in studying more than a thousand patients with NA-AION, the perceived “simultaneous” visual loss in both eyes usually occurred because the patient was unaware of the prior visual loss in the first eye and discovered it only when the second eye became involved. Simultaneous bilateral onset of NA-AION is extremely rare; it may be seen in patients who develop NA-AION during shock with marked fall of blood pressure, hemodialysis, or spinal surgery.
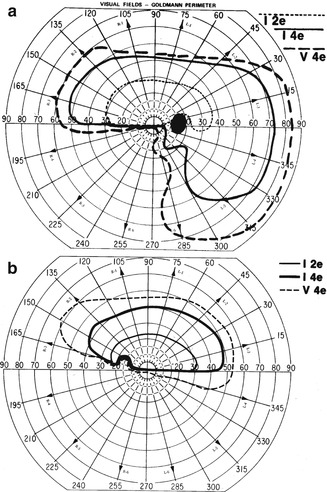
Fig. 19.6
Visual field defects in NA-AION, plotted with Goldmann perimeter (using I-2e, I-4e, and V-4e targets). (a) This shows inferior altitudinal defect with I-2e and inferior nasal defect with I-4e and V-4e. (b) This shows absolute inferior altitudinal defect with I-2e, I-4e, and V-4e. The visual acuity in both eyes was 20/20 (Reproduced from Hayreh and Zimmerman [56])
I [44] investigated seasonal variation of the onset of NA-AION for 839 episodes. The data showed that NA-AION onset was significantly more frequent in the summer Iowa City (USA) (the hot months, with temperatures from the 60s to low 90s) than in the winter (the cold months, when the maximum temperature is usually much below freezing) (p = .0030), with spring/fall or the mild months intermediate.
Visual Acuity
In a study of 500 consecutive NA-AION eyes, when patients were seen within 2 weeks after the onset of visual loss, initial visual acuity was 20/20 in 33 %, better than 20/40 in 51 %, and 20/200 or worse in 21 % [57, 58]. This shows that the presence of normal visual acuity does not rule out NA-AION. Comparison of refraction in NA-AION patients 50 years and older with that of an age-matched general population showed no significant difference between the two groups [37].
Visual Fields
In contrast to visual acuity, which can be within normal limits in almost one third of the eyes with NA-AION, visual field defects are a universal occurrence. Therefore, perimetry is the most important and essential visual function test to evaluate the visual loss. These eyes can present with a variety of optic nerve-related visual field defects. In a study of 312 consecutive NA-AION eyes, manual kinetic perimetry (i.e., visual fields plotted with a Goldmann perimeter) showed an overall prevalence of general visual field defects in 83 % with I-2e, 79 % with I-4e, and 69 % with V-4e and of scotoma(s) within the central 30° in 55, 49, and 36 %, respectively [56]. Central scotoma was seen in 49 % with I-2e, 44 % with I-4e, and 29 % with V-4e. Relative inferior altitudinal defect was common (35 % with I-2e and 22 % with I-4e), but absolute inferior altitudinal defect was seen in only 8 %. By contrast, absolute inferior nasal sector visual loss was the most common defect detected in NA-AION (22 %). Thus, a combination of a relative inferior altitudinal defect with absolute inferior nasal defect is the most common pattern in NA-AION (Fig. 19.6a). This contradicts the commonly held belief that inferior altitudinal visual field defect is typical of NA-AION.
Currently, visual fields are usually plotted using automated perimetry; unfortunately, automated perimetry provides information on only up to about 24–30° in the periphery. Kinetic perimetry, by contrast, provides peripheral visual field information all the way to about 80–90° temporally, 70° inferiorly, 60–70° nasally, and 50–60° superiorly. This has two important implications.
Central visual field defects: Large scotomas in the central 24–30° on automated perimetry may be misinterpreted as altitudinal when in fact the eye still may have intact peripheral field outside the central 24–30°. This may be a factor in the widespread erroneous belief that inferior altitudinal field defect is the most common defect in NA-AION.
Peripheral visual field defects: It is well established that the constant tracking provided by the peripheral visual fields is essential for sensory input to our day-to-day activity. For example, the peripheral visual field is vital for driving and “navigating” in the world. In view of that, to assess the visual function disability produced by NA-AION, it is important to have complete information about the peripheral visual fields and any impairment in them. While kinetic perimetry provides that information reliably, automated perimetry does not. This is a big drawback in automated perimetry to evaluate visual function in NA-AION.
Therefore, in NA-AION the visual field plotted with manual kinetic perimetry provides far superior information about the type of visual field defect and the peripheral field and for evaluating visual functional disability [56].
Natural History of Visual Outcome in NA-AION
Information on the natural history of visual outcome in NA-AION is vital to determine if any treatment modality advocated for these diseases is really beneficial or not. The gold standard is to compare the outcome of treatment with the natural history of the disease. The importance of information about the natural history of visual outcome is very well illustrated by the following example: A study of optic nerve sheath decompression for the treatment of NA-AION claimed to improve visual loss in this disease – “a disorder without any previously effective therapy” [57]. This “finding” was considered so important that it was published on an expedited basis by the Archives of Ophthalmology, and the procedure became widely popular, till a multicenter clinical trial [47] showed that it was actually harmful; eyes that had the procedure suffered significantly greater (24 %) loss of vision than those left alone (12 %). This clinical trial also showed that 32.6 % of those who had optic nerve sheath decompression had visual improvement compared with 42.7 % of the untreated group. This study concluded that this procedure is “not an appropriate treatment for non-arteritic anterior ischemic optic neuropathy.”
Two prospective studies have evaluated the natural history of visual outcome in NA-AION, one based on 125 eyes [47] and the other on 386 eyes [58]; both arrived at the same conclusion. They showed that patients seen within 2 weeks of onset of visual loss, with initial visual acuity of 20/70 or worse, experienced spontaneous improvement in 41–43 % of the cases and worsening in 15–19 %, at 6 months. One of these studies that evaluated visual fields with kinetic perimetry showed that 26 % of those who were first seen ≤2 weeks of onset with moderate to severe visual field defect showed improvement at 6 months [58]. Visual acuity and visual fields showed improvement or further deterioration mainly up to 6 months, with no significant change after that [58]. My study also showed that there is no correlation between the visual outcomes in the two eyes when a patient develops NA-AION in the second eye [59].
Anterior Segment of the Eye
This invariably shows no abnormality except for the presence of relative afferent pupillary defect in unilateral NA-AION eyes, and in some there may be raised intraocular pressure.
Optic Disc Changes
Since 1974, several studies have shown that eyes with NA-AION have a significantly higher prevalence of absent or small cup than the general population [37, 60]. This has resulted in a misconception in the ophthalmic community that a small or absent cup is actually the primary factor in the development of the disease; this has resulted in catchy terms like “disc at risk.” The role of an absent or small cup in the pathogenesis of development of NA-AION is discussed in detail elsewhere [36, 37]. That showed that in the multifactorial scenario of the pathogenesis of NA-AION, contrary to the prevalent impression, an absent or small cup is simply a secondary contributing factor, once the process of NA-AION has started, and not a primary factor [36, 61, 62].
In NA-AION, at the onset of visual loss, there is always optic disc edema [64]. There are several misconceptions about optic disc edema in NA-AION. The most common one is that in NA-AION the optic disc edema is always pale – that is not true at all initially, because the color of optic disc edema in NA-AION initially does not differ from optic disc edema due to other causes – in some cases there may even be hyperemia of the optic disc (Figs. 19.7, 19.8, and 19.9b). A splinter hemorrhage at the disc margin is common (Fig. 19.8). Optic disc pallor starts to develop about 2–3 weeks after the onset of NA-AION [62]. A study based on the evaluation of various aspects of optic disc edema in 749 eyes showed that the overall median time (25th–75th percentile) to spontaneous resolution of optic disc edema from the onset of visual loss was 7.9 (5.8–11.4) weeks [62]. The time it took to resolve depended on several factors, e.g., longer in diabetics than in nondiabetics, and worse initial visual field defect and visual acuity were associated with a faster resolution of optic disc edema. When patients were treated with corticosteroid therapy within 2 weeks after onset of NA-AION, there was a significantly faster optic disc edema resolution than in untreated cases. There is a characteristic evolutionary pattern of optic disc edema in NA-AION [62]. The involved part of the disc (i.e., corresponding to the location of visual field loss) initially has edema, with the rest of the disc normal or showing much less edema → after several days the entire disc may show generalized edema → still later, the optic disc in the originally involved part begins to develop pallor and the edema gradually starts to regress in that part, so that the uninvolved part (corresponding to the normal visual field) may have more edema than the ischemic part (that has caused confusion) → then the involved part has pallor but is not edematous any more, while the rest of the disc may show mild edema and even some pallor → the optic disc edema gradually resolves → pallor of the involved region only or the entire disc (Fig. 19.9c). In the latter case, the pallor may or may not be more marked in the involved part. Therefore, the sector of the optic disc showing edema usually corresponds to the location of the visual field defect only during the very early stage, and not later on. Similarly, Arnold and Hepler [63] recorded “no consistent correlation” of the sector of the disc edema with the visual field defect. On resolution of optic disc edema, the distribution of optic disc pallor does not always correspond with the extent and location of visual and nerve fiber loss [62].
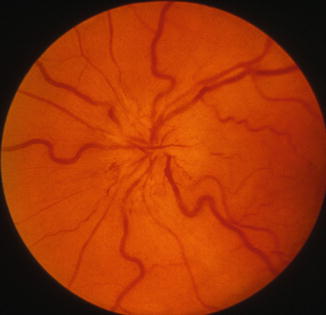
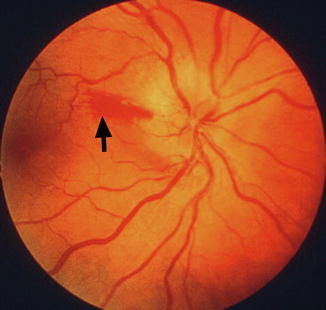
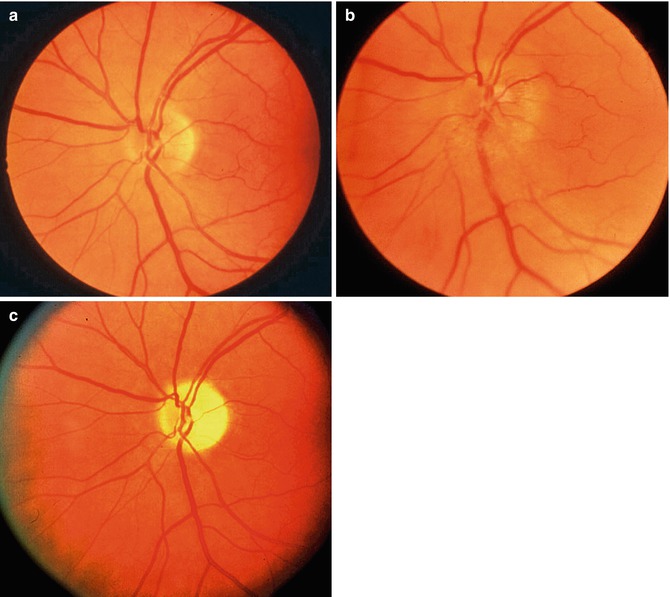
Fig. 19.7
Left fundus photograph shows optic disc edema and hyperemia during the acute phase of NA-AION (Reproduced from Hayreh [1])
Fig. 19.8
Right fundus photograph shows optic disc edema and hyperemia, with a splinter hemorrhage (arrow) during the acute phase of NA-AION (Reproduced from Hayreh [1])
Fig. 19.9
Fundus photographs of the left eye of a 53-year-old man. (a) Normal disc before developing NA-AION. (b) With optic disc edema during the active phase of NA-AION. (c) After resolution of optic disc edema and development of optic disc pallor – more marked in the temporal part than the nasal part (Reproduced from Hayreh [1])
In the fellow normal eye, the optic disc usually shows either a small cup or none. This can be a helpful clue to the diagnosis of NA-AION in doubtful cases. If both eyes originally have small disc cups, I have seen that in unilateral NA-AION, once the disc edema resolves, the cup in the involved eye may become slightly larger than the fellow eye because of the loss of nerve fibers. This has also been reported by others [64].
In an occasional case, where NA-AION is due to embolism into the PCA, the optic disc edema usually has a chalky white appearance, unlike in the classical NA-AION.
In diabetics, optic disc changes in NA-AION may have some characteristic diagnostic features. During the initial stages, the optic disc edema is usually (but not always) associated with characteristic prominent, dilated, and frequently telangiectatic vessels over the disc and much more numerous peripapillary retinal hemorrhages than in nondiabetics (Fig. 19.10a, c) [26, 65]. These findings may easily be mistaken for proliferative diabetic retinopathy associated with optic disc neovascularization. When the optic disc edema resolves spontaneously, these prominent telangiectatic disc vessels and retinal hemorrhages also resolve spontaneously (Fig. 19.10b, d). The presence of these characteristic fundus changes in some diabetics with NA-AION has resulted in a good deal of controversy because it has been thought to be a separate clinical entity – described under different eponyms, the most common being “diabetic papillopathy,” when in fact it is NA-AION [26].
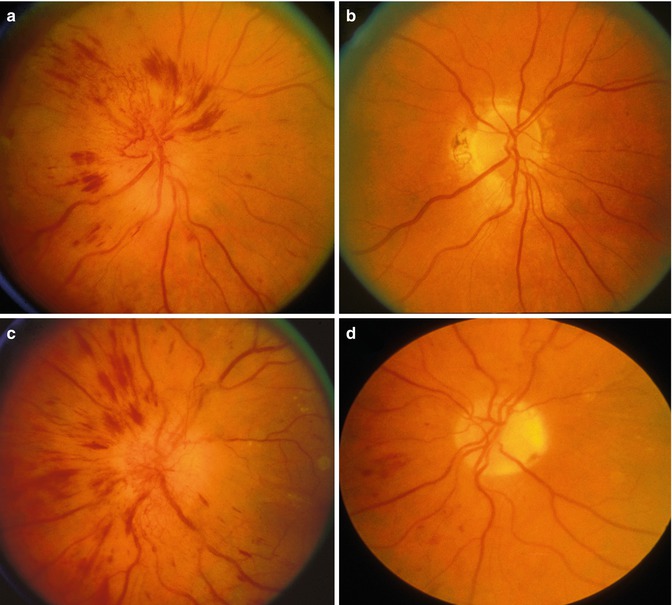
Fig. 19.10
Fundus photographs of both eyes of a 51-year-old diabetic woman, who developed NA-AION, first in the right eye (a, b) and 8 months later in the left eye (c, d). (a, c) show optic disc edema with marked telangiectatic vessels on the optic disc and multiple punctate peripapillary hemorrhages. (b, d) show no edema, no abnormal vessels on the disc, and no peripapillary retinal hemorrhages on resolution (Reproduced from Hayreh and Zahoruk [65])
Other Fundus Changes
The presence of a few splinter hemorrhages on the optic disc or immediate peripapillary region is common in association with the optic disc edema (Figs. 19.8 and 19.11a); those resolve spontaneously with optic disc edema resolution. Diabetics tend to have more peripapillary retinal hemorrhages than nondiabetics [26, 65]. Occasionally, I have seen mild serous retinal detachment between the optic disc and macula and that may even extend to the macular region to produce macular edema (Fig. 19.11). This has also been reported by other authors [66, 67]. Because of optic disc edema, there is a certain amount of retinal venous engorgement. In some eyes, as the optic disc edema resolves, some lipid deposits are seen in the peripapillary or macular region.
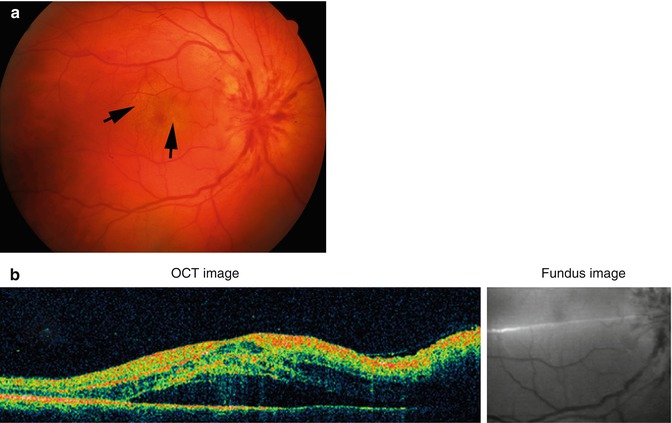
Fig. 19.11
Fundus photograph (a) and OCT (b) of the right eye with NA-AION and serous retinal detachment between the optic disc and the macula. In (a) arrows indicate the presence of lipid deposits in the central part of the macula
Fluorescein Fundus Angiographic Findings
It is only angiography during the very early arterial phase of dye filling in the fundus that demonstrates the telltale impaired circulation and its location in NA-AION. In my studies, there is almost invariably a filling defect/delay in the prelaminar region and in the peripapillary choroid (Fig.19.12) and/or choroidal watershed zones (Figs. 19.12b and 19.13) at the onset of NA-AION [35]. Others have also noted this [68, 69]. In the occasional case, where NA-AION is due to embolism into the PCA, the part of the choroid supplied by the occluded PCA or short PCA does not fill (Fig. 19.14). Late optic disc staining is a nonspecific finding of optic disc edema and has no diagnostic importance for NA-AION.
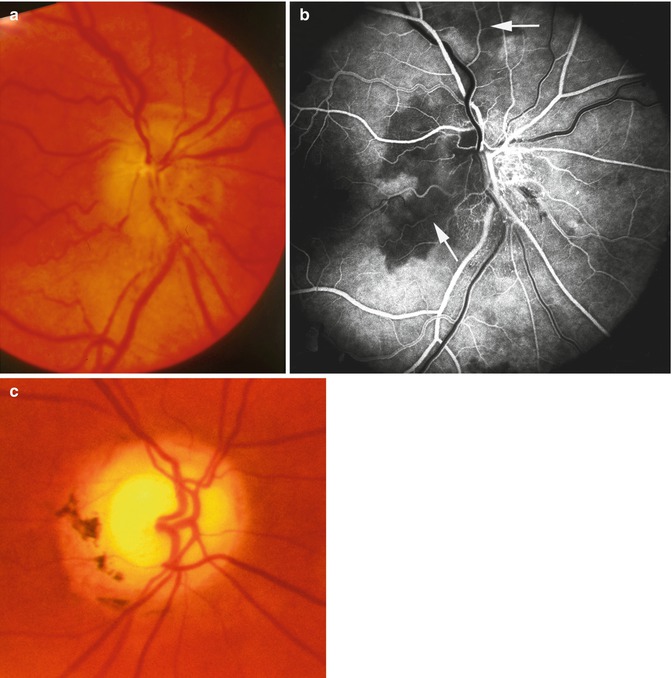
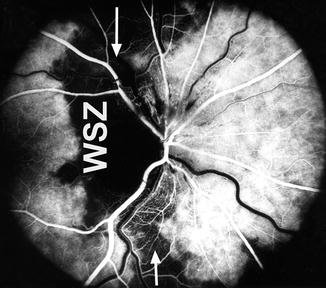
Fig. 19.12
Fundus photograph (a) and fluorescein fundus angiogram (b) of the right eye with NA-AION. (a) This shows optic disc edema, hyperemia, and hemorrhages on the optic disc. (b) Fluorescein fundus angiogram shows non-filling of the temporal part of the peripapillary choroid (arrow) and adjacent optic disc and the choroidal watershed zone (arrow) (Reproduced from Hayreh [35]). (c) Fundus photograph shows optic atrophy and optic disc cupping, with peripapillary degeneration (Reproduced from Hayreh [1])
Fig. 19.13
Fluorescein fundus angiogram of right eye with NA-AION, showing location of the watershed zone filling defect (arrows, WSZ, vertical dark band) in relation to the optic disc. The watershed zone is passing through the temporal part of the disc and adjacent temporal peripapillary choroid (Reproduced from Hayreh [35])
Fig. 19.14
Fundus photograph (a) and fluorescein fundus angiogram (b) of the right eye with embolic NA-AION. Temporal artery biopsy for giant cell arteritis was negative. Angiogram shows normal filling of the area supplied by the lateral PCA (including the temporal half of optic disc) but no filling of the area supplied by the medial PCA (including the nasal half of optic disc) (Reproduced from Hayreh [35])
Bilateral NA-AION
The cumulative probability of the fellow eye developing NA-AION has varied among different studies: 25 % within 3 years in 438 patients [70], 17 % in 5 years in 431 patients [49], and 15 % over 5 years in 326 patients [50]; however, different criteria were used to determine the probability, which may explain the differences. According to one study [70], the risk is greater in men, particularly young diabetic men, while according to another study [50] increased incidence was associated with poor baseline visual acuity and diabetes mellitus. The risk of the second eye getting involved by NA-AION was evaluated in 655 patients (206 diabetics and 449 nondiabetics) and that showed a significantly (p = 0.003) greater risk in diabetics than in nondiabetics [26]; that study also showed that the median (25th–75th percentile) time to involvement of the fellow eye by NA-AION was 6.9 (0.4–16.9) years in diabetics and 9.1 (1.8–19.0) years in nondiabetics. My study has shown that there is no correlation between the visual outcomes in the two eyes when a patient develops NA-AION in the second eye [59].
There are reports in the literature of simultaneous onset of bilateral NA-AION. As discussed above, in my study of more than a thousand patients with NA-AION, the reported “simultaneous” visual loss in both eyes due to NA-AION usually occurred because the patient was unaware of the NA-AION in the first eye until the second eye lost vision. The pattern of optic disc edema during the initial stages of NA-AION is different from that later on (see above), and that is helpful to assess the time of onset in bilateral NA-AION. Simultaneous bilateral onset of NA-AION is extremely rare, except in patients who develop sudden, severe arterial hypotension, e.g., during hemodialysis or surgical shock.
Recurrence of NA-AION in the Same Eye
Such recurrences mentioned in the literature are often more a progression of NA-AION during the acute stage rather than actual new episodes after the first episode has resolved completely. In a study of 829 NA-AION eyes, the overall cumulative percentage of recurrence of NA-AION in the same eye was at 3 months 1.0 ± 0.4 % (SE), at 6 months 2.7 ± 0.7 %, at 1 year 4.1 ± 0.9 %, and 2 years 5.8 ± 1.1 % [71]. The only significant association of recurrence of NA-AION was with nocturnal arterial hypotension. Thus, this study indicated that nocturnal diastolic arterial hypotension might be a risk factor for recurrence of NA-AION; however, since NA-AION is a multifactorial disease, other risk factors so far unknown may also play a role.
NA-AION in Diabetics Versus Nondiabetics
In a study of 655 consecutive NA-AION patients (931 eyes) – 206 patients with diabetes and 449 without – comparison of various clinical features of NA-AION in diabetics and nondiabetics showed no significant difference in age, but diabetics had slightly more women than men (45 % vs. 38 %; p = 0.078) and a higher prevalence of arterial hypertension (p < 0.0001), ischemic heart disease (p = 0.0001), transient ischemic attacks (p = 0.0003), and second eye involvement by NA-AION (p = 0.003) [26]. Initial visual acuity did not differ significantly between diabetics and nondiabetics; however, of those seen within 2 weeks of onset of NA-AION, diabetics had less severe visual field defect (p = 0.010). At 6 months after onset, there was no significant difference in visual acuity and visual field improvement between diabetics and nondiabetics. Time to optic disc edema resolution was (p = 0.003) longer in diabetics than nondiabetics. As discussed above, the optic disc edema in diabetics usually has characteristic, diagnostic dilated telangiectatic vessels during early stages of NA-AION (Fig. 19.10).
Incipient NA-AION
In 1981 [72], I reported that “symptomless optic disc edema precedes the visual loss and may be the earliest sign of AION (NA-AION).” In 2007, based on a detailed study of a series of 60 eyes with symptomless optic disc edema, I described this as a distinct clinical entity under the name of incipient non-arteritic anterior ischemic optic neuropathy [61]. In this condition, there is initially asymptomatic optic disc edema and no visual loss attributable to NA-AION. In 25 % the incipient disease progressed to classical NA-AION (after a median time of 5.8 weeks), and 20 % developed classical NA-AION after resolution of a first episode of incipient NA-AION. Patients with incipient compared to the classical NA-AION had a greater prevalence of diabetes mellitus (p < 0.0001) and lower prevalence of ischemic heart disease (p = 0.046). Comparing patients who progressed to classical NA-AION with those who did not, the former were significantly younger (p = 0.025); their visual acuity worsened in 31 %, while none of the latter did; 62 % of the former remained stable and 98 % of the latter. In the eyes with progression, central (in 31 %) and peripheral (in 77 %) visual fields worsened compared to only one eye and two eyes, respectively, that did not (p = 0.01 and p < 0.0001, respectively). Median time to resolution of optic disc edema in the progressed group was 5.8 weeks versus 9.6 weeks in those that did not. This study showed that incipient NA-AION is a distinct clinical entity, with asymptomatic optic disc edema and no visual loss attributable to NA-AION.
When a patient presents with asymptomatic optic disc edema, incipient NA-AION must be borne in mind as a strong possibility for those who have had classical NA-AION in the fellow eye, for diabetics of all ages, and for those with high risk factors for NA-AION; this can avoid unnecessary and expensive investigations. Since patients with incipient NA-AION have a greater prevalence of diabetes mellitus than classical NA-AION, this has often been misdiagnosed as “diabetic papillopathy” or “diabetic papillitis.”
NA-AION and Phosphodiesterase-5 (PDE5) Inhibitors
The subject is discussed at length elsewhere [73, 74]. Briefly, most patients who report developing NA-AION following the use of these drugs are middle-aged or elderly men who already had various predisposing risk factors for NA-AION (see above). These drugs are mostly taken in the evening for sexual intercourse. PDE5 inhibitors result in a fall of blood pressure; when taken in the evening, as discussed above, there is a high chance of them producing abnormal nocturnal arterial hypotension, which may be further aggravated if the person is taking other arterial hypotensive drugs for arterial hypertension or other cardiovascular disorders. Like the vast majority of NA-AION patients, most patients reporting NA-AION following ingestion of PDE5 discovered visual loss upon awakening in the morning. A critical review of all the reported cases shows a usually good temporal relationship between the ingestion of these drugs and onset of NA-AION. When all the above evidence is put together, it suggests that Viagra and other PDE5 inhibitors can result in development of NA-AION in persons who already have predisposing risk factors.
Amiodarone and NA-AION
There is a universal belief that amiodarone causes optic neuropathy, called “amiodarone-induced optic neuropathy.” However, the following facts do not support that view [75]:
1.
Patients who take amiodarone have cardiovascular disorders, which are per se well-established risk factors for the development of NA-AION [17, 27]. Many of these patients also have other risk factors (arterial hypertension, diabetes mellitus, hyperlipidemia, and ischemic heart disease) [17, 27]. They are candidates for NA-AION whether they are taking amiodarone or not.
2.
Patients on amiodarone often also take other drugs (beta-blockers, calcium channel blockers, ACE inhibitors) that influence the cardiovascular system. As discussed above, patients on these drugs are at high risk of developing nocturnal arterial hypotension, which is a common precipitating factor for the development of NA-AION [27, 45, 46].
3.
One of the arguments put forward to differentiate amiodarone-induced optic neuropathy from NA-AION is that some patients taking amiodarone develop asymptomatic optic disc edema that may later progress to visual loss. Asymptomatic optic disc edema has been known since 1981 as an early sign of NA-AION [72] and another study reported 60 eyes with “incipient NA-AION” that had asymptomatic optic disc edema to begin with [61]. Many of them progressed to visual loss, but not all. Not one of those patients was taking amiodarone. Optic disc edema for various reasons can persist much longer than the 6–8 weeks usually seen for typical NA-AION [62]. Moreover, there are reports of patients with asymptomatic optic disc edema progressing to visual loss after amiodarone had been discontinued [76].
4.
Most importantly, the clinical features of the optic neuropathy in patients taking amiodarone are typical of NA-AION rather than a toxic optic neuropathy.
Thus, in the multifactorial scenario of NA-AION, it is the systemic cardiovascular risk factors rather than amiodarone that cause NA-AION. Therefore, “amiodarone-induced optic neuropathy” is in fact NA-AION.
Familial NA-AION
There are five reports in the literature representing ten unrelated families in which more than one member developed NA-AION [77–81]. We [81] have shown that this rare entity of familial NA-AION is clinically similar to the classical nonfamilial NA-AION, with the exception that familial NA-AION occurred in younger patients and had much higher involvement of both eyes than the classical NA-AION. The role of genetic factors in familial NA-AION is not known. In fact, it could be argued that since NA-AION is a common disease, the possibility of occasional occurrence of clusters in families without any genetic abnormality cannot be ruled out. The potential role of genetic factors in familial NA-AION remains to be clarified by additional research. One preliminary study has suggested that the G4132A mitochondrial mutation may be associated with disease in at least one pedigree with familial NA-AION [80], but the report by us [81] indicates that this mutation is not associated with disease in two of the three familial NA-AION pedigrees in the study, nor is this mutation associated with the much more common classical nonfamilial NA-AION.
Post-hemorrhagic Amaurosis
In this clinical entity, there is a visual loss following distant recurrent or massive systemic hemorrhages, from a variety of medical conditions, e.g., uterine bleeding, gastrointestinal bleeding, hemoptysis, epistaxis, or repeated venesection, often recurrent in nature. Its pathogenesis is discussed elsewhere [31]. During recent years, a consensus has emerged that it is due to ischemia of the optic nerve head; that is, it represents NA-AION.
Management of NA-AION
This has been a highly controversial subject. A number of treatments have been advocated, principally the following.
Optic Nerve Sheath Decompression
Sergott et al. [57] in 1989 claimed that optic nerve sheath decompression improved visual function in “progressive” NA-AION. But based on my studies on different basic aspects of the subject, I [82] concluded that there was no scientific rationale for doing optic nerve sheath decompression in NA-AION and that the procedure can be harmful. After the report by Sergott et al. [57] and a few other anecdotal reports [83, 84], the procedure gained worldwide favor not only in “progressive” but also in all types of NA-AION. A multicenter Ischemic Optic Neuropathy Decompression clinical trial [47] subsequently established that this procedure is “not effective” and “not an appropriate treatment for non-arteritic AION” and “may be harmful,” because 24 % of the eyes with the optic nerve sheath decompression suffered further visual loss as compared to only 12 % simply left alone. This study also showed that 42 % of cases showed improvement in visual acuity spontaneously, without any procedure.
Aspirin
It is common practice to prescribe aspirin in NA-AION. One study [85], based on 131 patients, claimed that aspirin prevented the development of NA-AION in the fellow eye. A much larger study, based on 431 patients with unilateral NA-AION, revealed no long-term benefit from aspirin in reducing the risk of NA-AION in the fellow eye [49]. Similarly, Newman et al. [50] found no association between regular aspirin use and the incidence of new NA-AION in the fellow eye. Botelho et al. [86] also found that use of aspirin does not improve the visual outcome in NA-AION patients. These findings are not surprising, since NA-AION is not a thromboembolic disorder but a hypotensive disorder and aspirin has no effect on the blood pressure or nocturnal arterial hypotension.
Systemic Corticosteroid Therapy
The role of systemic corticosteroid therapy in NA-AION has become highly controversial; therefore, it requires detailed discussion.
A small study by Foulds [87] at the University of Glasgow, Scotland, in 1969, and my own preliminary study [11] at the University of Edinburgh, Scotland, in 1972, indicated that systemic corticosteroids may improve visual acuity in NA-AION. Based on that information, in 1973 I planned a large, multicenter randomized clinical trial to investigate systematically in a large cohort of NA-AION patients whether systemic corticosteroids improved visual outcome or not. Unfortunately, that clinical trial was not funded by the National Institute of Health (the main research funding agency in the United States), because of a firm belief among neuro-ophthalmologists (equating ischemic stroke and NA-AION as pathogenetically similar in nature) that corticosteroid therapy has no role in NA-AION. Since no alternative treatment existed, I felt that it was crucial to find out whether corticosteroid therapy was actually beneficial, ineffective, or conceivably harmful in NA-AION. Because no funds were available, instead of the “conventional randomized study,” I decided on a “patient choice” study – the next best option. Every NA-AION patient seen in my clinic was given a free and informed “patient choice.” The decision was left entirely up to the patient, to opt for corticosteroid therapy or no treatment, in consultation with their physicians or other sources. Most importantly, we had no influence at all on their choice. I specifically told all patients that I really did not know whether the treatment was beneficial, ineffective, or even harmful.
I collected the data for 28 years, completely masked about visual outcomes, numbers, and other aspects of patients in the study. The study finally included 613 consecutive NA-AION patients (696 eyes) seen in my clinic. The results are discussed at length elsewhere [88].
Treatment Protocol
Initially 80 mg prednisone daily was given for 2 weeks and then tapered down to 70 mg for 5 days and 60 mg for 5 days and after that cut down by 5 mg every 5 days, to nothing [88].
Data Analysis of the Study [88]
This revealed the following four surprises:
1.
Of the 613 patients with NA-AION, 51 % voluntarily opted for systemic corticosteroid therapy and 49 % opted for no treatment. This was a total surprise: after collecting data for 28 years, it turned out that equal numbers of the patients opted for and against treatment.
2.




Equally surprising was that rigorous statistical testing [88] found no statistically significant difference between the two groups in visual acuity and visual fields. Also there was no significant difference in systemic diseases in the two groups, except that patients who opted for treatment were slightly younger (59.2 vs. 62.0 years) and had a lower prevalence of arterial hypertension (34 % vs. 43 %). To determine if those two factors influenced the visual outcome, they were accounted for in the statistical analysis by including them as covariates in the logistic regression model. That showed that they made no difference in visual outcome (age p = 0.8; hypertension p = 0.6), so that in fact there was no significant difference in systemic diseases between the two groups in the study to influence the visual outcome.
The most crucial requirements in any “randomized clinical trial” are that the treated and untreated groups must be comparable in demographic and clinical characteristics. As is evident from above, my “patient choice” study definitely fulfilled those crucial criteria of a “randomized clinical trial.” In spite of that, critics have continued to argue that my study was not a “randomized clinical trial” (see below).
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
