Purpose
To assess the safety and to conduct a preliminary assessment of efficacy of intravitreal infliximab, an anti–tumor necrosis factor antibody, for sight-threatening relapsing uveitis in Behçet disease.
Design
Prospective, noncomparative, interventional pilot study.
Methods
A single intravitreal injection of infliximab (1 mg/0.05 mL) was given to 15 patients with relapsing posterior uveitis at the onset of a unilateral attack. Best-corrected visual acuity, anterior chamber cells, vitreous haze, and posterior eye segment inflammation were assessed at baseline and at 1, 7, 14, and 30 days after treatment.
Results
Ocular or extra-ocular side effects were not observed. Baseline best-corrected visual acuity (mean logarithm of minimal angle of resolution, 0.74; range, 0.15 to 1.7) improved significantly by day 7 and continued to improve through day 30 after infliximab (mean, 0.30; P < .0001). Profound decreases in anterior chamber cells and vitreous haze (both P < .0001), as well as beneficial effects in retinal vasculitis ( P = .0001) and retinitis ( P = .001) were evident through day 30. Cystoid macular edema persisted in 9 of 11 eyes affected, but central macular thickness decreased from a baseline mean of 434 to 309 mm at the end of follow-up ( P < .0001). Lack of systemic treatment at baseline in 4 patients or background immunosuppressive medications, which remained unchanged during follow-up, did not influence significantly these responses; additional treatment was not required.
Conclusions
These findings suggest that intraocularly produced or acting tumor necrosis factor, or both, is crucial in Behçet disease-associated relapsing uveitis and that intravitreal infliximab should be considered when systemic administration is not feasible or contraindicated. Further studies may identify patients for whom intravitreal infliximab is preferable to systemic treatment.
Tumor necrosis factor (TNF) is a key proinflammatory cytokine with pleiotropic functions implicated in the pathogenesis of ocular inflammation associated with systemic (auto)immune diseases, such as juvenile idiopathic arthritis, rheumatoid arthritis, seronegative spondyloarthropathies, inflammatory bowel disease, and Behçet disease. Evidence also has suggested a role of TNF in additional ocular pathologic features with an inflammatory component, such as diabetic macular edema and neovascular age-related macular degeneration (AMD).
Behçet disease, also referred to as Adamantiades-Behçet disease, is a chronic multisystem inflammatory disorder of unknown cause classified among the vasculitides. Behçet disease affects the small and large vessels of the venous and arterial systems, and in addition to recurrent mucocutaneous lesions, the disease’s hallmark, many patients experience ocular inflammation, which may result in irreversible damage and visual loss. In 2006, an analysis of clinical data derived from 25 eye centers from 1465 prevalent cases with ocular lesions revealed that, despite treatment advances, Behçet disease carries a poor visual prognosis with one quarter of the patients blind. A retrospective study of 880 consecutive Behçet disease patients with uveitis seen at a single centre from 1980 through 1998 revealed that the risks of losing useful vision at 5 and 10 years for men and women is 21% versus 10% and 30% versus 17%, respectively. Rapid and effective suppression of inflammation is the first aim of treatment of sight-threatening involvement of the posterior eye segment to avoid development of permanent lesions in the retina and optic disc. In patients who are unresponsive or intolerant to systemic medications, despite the lack of evidence from randomized controlled trials, either intravitreal or intravenous high-dose corticosteroids generally are used, with cataracts and glaucoma being common side effects.
The anti-TNF monoclonal antibody infliximab has been used widely in rheumatoid arthritis, spondyloarthropathies, inflammatory bowel disease, and psoriasis during the last decade. A single intravenous infusion of the anti-TNF monoclonal antibody infliximab in patients with Behçet disease in whom sight-threatening panuveitis developed despite intensive immunosuppressive therapy resulted in rapid and effective suppression of ocular inflammation. More recently, we reported that a single intravenous infusion of infliximab exerts a significantly faster effect in suppressing ocular inflammation than intravitreal triamcinolone or intravenous high-dose methylprednisolone in these patients. Up to the year 2010, results on more than 262 infliximab-treated patients with ocular Behçet disease have been published, with an impressive improvement rate of approximately 90%. According to the European recommendations for the management of Behçet disease, any patient with more than 2 lines of drop in visual acuity on a 10/10 scale, with retinal disease (retinal vasculitis or macular involvement), or both should receive either infliximab or cyclosporine A in combination with azathioprine and corticosteroids; alternatively, interferon-α with or without corticosteroids can be used.
Blocking TNF actions by intravenous administration of infliximab has been associated with reactivation of latent tuberculosis, which is particularly prevalent in countries where Behçet disease is endemic. Moreover, in patients with a history of cancer or congestive heart failure, systemic anti-TNF treatment is contraindicated. Therefore, providing that therapeutic intraocular concentrations of infliximab can be achieved, an intravitreal injection with minimal systemic absorption would minimize, if not eliminate, systemic adverse effects of TNF blockade. Along this line, several experimental studies on the efficacy and safety of intraocular administration of infliximab have been conducted. Herein, we present the results of a pilot study on the safety and efficacy of a single intravitreal injection of 1 mg infliximab given for a sight-threatening uveitis attack in patients with Behçet disease.
Methods
Protocol
This prospective, 4-week, noncomparative, interventional, nonrandomized single-center pilot study included patients with relapsing ocular inflammation associated with Behçet disease in whom a unilateral sight-threatening attack of uveitis developed affecting the posterior eye segment.
Sight-threatening uveitis attack was defined as an acute decrease in best-corrected visual acuity (BCVA) and the presence of inflammation of the posterior segment, without or with concomitant anterior uveitis (more than 0.5+ cells in the anterior chamber) or vitreitis evidenced by the presence of haze. Posterior segment inflammation was documented by the presence of at least one of the following: retinal vasculitis, retinitis, cystoid macular edema (CME), and papillitis. A single intravitreal injection of infliximab (1 mg/0.05 mL), was administered at the onset of the attack, in addition to baseline maintenance therapy, which remained unchanged during the following month.
BCVA and ocular inflammation were assessed at baseline, as well as at days 1, 7, 14, and 30 after baseline, as described. CME, when present, was assessed by optical coherence tomography (OCT III; Humphrey Company, San Leandro, California, USA). Intraocular inflammation was evaluated and analyzed, based on published criteria modified to fit to uveitis in Behçet disease, as follows: anterior segment (grading of anterior chamber cells from 0 to 4), vitreous (grading of vitreous haze from 0 to 4), and posterior segment of the eye (presence as 1, absence as 0 of retinal vasculitis, retinitis, and CME). Using these data, the fundus inflammation score (retinitis, retinal vasculitis, CME, and papillitis; maximum score of 4) was calculated at each visit. The institutional review board approved the study and all patients provided written informed consent after being informed about the nature and possible consequences of the procedure, according to the Declaration of Helsinki.
Intervention
Infliximab injection was accomplished under sterile conditions. The eye was prepared using the standard protocol for intravitreal injections. A vial containing 100 mg infliximab powder (Remicade; Sherring-Plough, Athens, Greece) was reconstituted with 5 mL sterile water and 0.05 mL of this solution, containing 1 mg of infliximab, was injected intravitreally 3.5 mm from the limbus with a 30-gauge needle under topical anesthesia and under sterile conditions. The solution’s osmolarity and pH were 306 mOsm/kg and 7.25 mOsm/kg, respectively. The injected eye was instilled with topical ofloxacin 0.3% immediately after the injection.
Statistical Analysis
Mixed model analysis for longitudinal data was considered for the assessment of logarithm of the minimal angle of resolution BCVA, total inflammation score, fundus score, macular thickness, intraocular pressure, anterior chamber cells, and vitreous cells. Models were fitted by restricted maximum likelihood using patients as random factors; the selection of the best covariance matrix was based on the Akaike information criteria, and in all models, the best fit was under the compound symmetry because the correlation between repeated measurements seemed to remained the unchanged.
Generalized estimating equations modeling population averages were used for the longitudinal binary outcome regarding presence of vasculitis, retinitis, or CME. In both mixed model and generalized estimating equation analyses, 2 approaches were considered: at the first approach, time was fitted as continuous variable (with random intercept) to test the time dependence of the predictors; at the second approach, time was considered class variable to find the exact time point the improvement was initiated. Statistical analysis was performed with SAS software version 9.2 (SAS Institute, Cary, North Carolina, USA).
Results
Fifteen patients (10 men) fulfilling the International Study Group criteria for Behçet disease and mean disease duration ± standard deviation of 5.6 ± 5.3 years were studied. Their ages ranged from 23 to 53 years (± standard deviation, 35.3 ± 8.9 years). At the day of the unilateral ocular attack, 4 patients were not receiving systemic immunosuppressive treatment. Oral medications in the remaining patients included monotherapy with azathioprine (n = 4) or cyclosporine A (n = 1), combinations of azathioprine and corticosteroids (n = 2) or of azathioprine and cyclosporine A (n = 3), or the triple combination of azathioprine, cyclosporine A, and corticosteroids (n = 1). All these oral background medications remained stable during follow-up. Thirteen patients were naïve to anti-TNF treatment, whereas 2 patients had received intravenous treatment with infliximab for relapsing ocular inflammation in the past.
Safety
After the single intravitreal injection of 1 mg infliximab, clinical ocular side effects, including any evidence of induction of intraocular inflammation, were not observed during follow-up in all 15 eyes. Mean intraocular pressure changed nonsignificantly from 14.1 mm Hg at baseline to 18.9 mm Hg at days 1 and 7, to 17.8 mm Hg at day 14, and to 15.7 mm Hg at day 30 and did not require any intervention. No extraocular adverse events were observed by the physicians or were reported by the patients during follow-up.
Efficacy
At the onset of uveitis attack, BCVA ranged from 20/800 to 20/200 (n = 15) in the Snellen chart. Baseline mean values of logarithm of the minimal angle of resolution BCVA, anterior chamber cells, vitreous haze, as well as the presence of retinal vasculitis, retinitis, and CME are shown in the Table . Papillitis was not present in any eye.
| Baseline | Day 1 | Day 7 | Day 14 | Day 30 | Significance of Change from Baseline through Day 30 ( P Value) a | |
|---|---|---|---|---|---|---|
| Mean logMAR best-corrected visual acuity (95% CI) | 0.74 (0.51 to 0.96) | 0.67 (0.45 to 0.89) | 0.54 (0.32 to 0.76) b | 0.38 (0.16 to 0.60) | 0.30 (0.07 to 0.52) | < .0001 |
| Mean anterior chamber cells (95% CI) | 2.13 (1.55 to 2.72) | 1.93 (1.35 to 2.52) | 1.07 (0.49,1.64) b | 0.67 (0.27 to 1.07) | 0.20 (0.0 to 0.51) | < .0001 |
| Mean vitreous haze (95% CI) | 1.73 (1.24 to 2.22) | 1.73 (1.24 to 2.22) | 1.20 (0.77 to 1.63) b | 0.80 (0.37 to 1.23) | 0.33 (0.06 to 0.60) | < .0001 |
| Vasculitis present, n | 10/15 | 10/15 | 10/15 | 10/15 | 1/15 b | .0001 |
| Retinitis present, n | 8/15 | 8/15 | 7/15 | 1/15 b | 0/15 | .0010 |
| Cystoid macular edema present, n | 11/15 | 11/15 | 11/15 | 11/15 | 9/15 | NS |
| Mean macular thickness, mm (95% CI) | 434 (364 to 504) | ND | 408 (338 to 479) b | 353 (285 to 421) | 309 (227 to 391) | < .0001 |
| Mean fundus score (95% CI) | 1.93 (1.53 to 2.33) | 1.93 (1.53 to 2.33) | 1.87 (1.46 to 2.27) | 1.47 (1.06 to 1.87) | 0.67 b (0.26 to 1.07) b | < .0001 |
a Using mixed-model analysis for longitudinal data or generalized estimating equations, when appropriate.
b Denotes the first time point in which improvement from baseline became statistically significant.
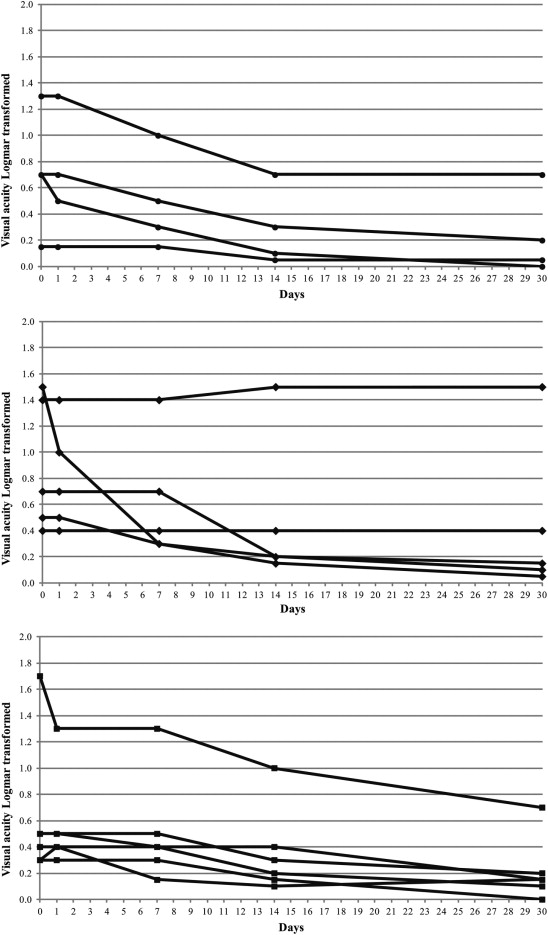
At day 1 after the intravitreal injection of infliximab, no significant changes were evident. At day 7, however, anterior chamber cells and vitreous haze decreased significantly, whereas BCVA improved significantly. Further progressive decreases of anterior chamber cells and vitreous haze and improvement of BCVA were evident at days 14 and 30. As shown in the Table , beneficial effects were evident through day 30 in all components of ocular inflammation except CME presence. Retinal vasculitis, which persisted until day 14 in all 10 eyes, was cleared at day 30 in 9 of 10 eyes. Retinitis cleared before day 14 in 7 of 8 eyes. Individual changes in BCVA from baseline through day 30 are shown in Figure 1 . Consequently, the mean fundus inflammation score decreased from 1.93 at baseline to 0.63 at day 30 ( P < .0001); at this time point, complete resolution of inflammation was evident in 6 of 15 eyes (fundus score, 0).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


