Reoperation for recurrent or persistent thyroid cancer presents a challenge for the head and neck surgeon. Scarring, edema, and friability of the tissues together with distortion of the landmarks make reoperative thyroid hazardous. Meticulous surgical dissection with identification of the recurrent laryngeal nerve is of paramount importance. Intraoperative neuromonitoring is useful in reoperative thyroid surgery especially in situations where the anatomic situation diverges from the normal. Intraoperative neuromonitoring may reduce the morbidity of reoperative thyroid surgery.
Iatrogenic injury to the recurrent laryngeal nerve (RLN) remains a source of morbidity for patients undergoing surgery of the thyroid gland. The incidence of permanent damage of the nerve varies from 0.4% to 4%. In revision surgery, however, the potentials for iatrogenic injury increase significantly . Hemmerling and colleagues stated that the incidence of temporary or permanent paresis of the RLN may be as high as 20% in thyroid cancers and recurrent goiter. Intraoperative monitoring techniques have been routinely used by many surgeons to provide functional assessment of the RLN during surgery. Although there is no substitute for detailed knowledge of anatomy, the use of intraoperative neuromonitoring (IONM) can be valuable in maintaining the functional integrity of the RLN, especially during revision thyroid surgery. Kim and colleagues state that intraoperative RLN monitoring is one of the factors that have reduced the morbidity of reoperative central compartment for thyroid cancer dissections. This article explores various IONM techniques used during revision thyroid surgery.
The RLN innervates all of the muscles of the larynx except for the cricothyroid muscle, which is supplied by the external branch superior laryngeal nerve. Those muscles include the posterior and lateral cricoarytenoid muscles; the thyroarytenoid muscle (vocalis muscle); and the transverse arytenoid muscle. If a patient has an injury to one of the RLNs, they present with symptoms of hoarseness. Bilateral damage to the RLNs causes respiratory distress.
Flisberg and Lindholm were among the first to use electrical stimulation of the RLN during thyroid surgery. Since that time, IONM has gained widespread popularity, in part because of advances in electrophysiologic monitoring. Advances in electrode technology, recording and stimulation techniques, and monitoring equipment have made monitoring of the RLN a practical tool for surgeons. The application of RLN monitoring can be grouped into three categories:
- 1.
Use of IONM in identifying the RLN
- 2.
Continuous monitoring of the RLN with the use of spontaneous electromyography during resection
- 3.
Intraoperative functional assessment of the RLN preresection and postresection
Lahey and Hoover were one of the first to highlight the importance of intraoperative identification of the RLN and argued that nerve identification is an integral part of thyroid surgery. Mountain and colleagues stated that there is a three to four time greater risk of nerve paralysis if the RLN is not identified during surgery. Hermann and colleagues in their study found that nerve identification significantly reduced the incidence of nerve injury. Detailed knowledge of anatomy is of the utmost importance to the identification and preservation of the RLN, and the use of neuromonitoring should serve as an adjunct technique. Hermann and colleagues stated that neuromonitoring cannot serve as a substitute for training by an experienced surgeon. He did reason that neuromonitoring would be useful when anatomic variants are encountered and especially in the case of revision surgery. Timon and Rafferty recommended the use of neuromonitoring for all revision thyroid surgeries.
Every attempt should be made to identify the RLN anatomically. In cases of reoperative thyroid surgery when scarring has distorted the normal anatomy or encased the RLN making anatomic identification difficult, however, the RLN may be identified with the aid of evoked electromyography ( Fig. 1 ). Electrical stimulation used for nerve identification consists of the use of either a monopolar or bipolar stimulator. There are inherent advantages with the use of either stimulation technique. With bipolar stimulation, current flow is regulated between the two probes. Tiel and colleagues pointed out that greater localized current flow is achieved with bipolar stimulation. With the improved selectivity of bipolar stimulation, however, some degree of sensitivity is compromised mostly because of the distance the nerve is from the stimulation site or shunting from overlying tissue or fluid. Selesnick stated that monopolar stimulation is more effective in localizing a nerve while reducing the amount of false-negatives obtained from current shunting and stimulation distance as seen with bipolar stimulation. Monopolar stimulation may be particularly helpful during revision thyroid surgery where normal anatomy has been compromised or distorted. When the course of the RLN has been better delineated, bipolar stimulation can be beneficial in pinpointing the exact location .
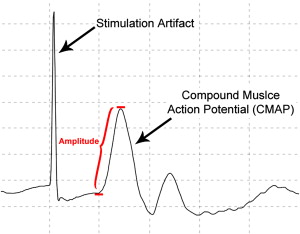
Identification of the RLN requires electrically stimulating the nerve and recording an electromyographic (EMG) response in the targeted muscles. Several parameters must be taken into consideration when applying electrical current to a nerve: the pulse, amplitude, and frequency of the applied stimulation. Standardization of these parameters is not agreed on universally. Pulse duration should range from 50 to 100 microsecond, with 50 microsecond being more optimal stimulus duration. Selesnick stated that if the pulse duration is too short, sensitivity may be compromised. When stimulating a nerve, the stimulation level can range from 0.5 to 5 mA. According to Harper , stimulation intensities vary depending on the distance from the stimulating probe, if the nerve is embedded among tissue or fluid, or if the nerve is damaged. Brennan and colleagues in their study found that normally functioning facial and RLNs had stimulation thresholds less than or equal to 0.4 mA. Marcus and colleagues reported a mean stimulation level of the RLN of 0.57 mA. The frequency of stimulation should be kept at 2 Hz or less.
There are several methods of evaluating EMG potentials from stimulation of the RLN. Recording techniques can use either surface or needle electrodes. A fiberoptic laryngoscope or laryngeal mask anesthesia is sometimes used for visual inspection of the vocal folds on stimulation of the RLN. Surgeons may use laryngeal palpation techniques to detect EMG activity during nerve stimulation .
A pair of subdermal electrodes or fine-hooked wire electrodes can be inserted directly into the vocal cords using simultaneous direct laryngoscopy. Alternatively, needle electrodes may be inserted through the cricothyroid membrane into the vocal muscle.
Tschopp and Gottardo compared the use of intralaryngeal surface electrodes with that of bipolar transligament electrode and the monopolar endolaryngeal needle electrodes. In their study, they concluded that needle electrodes are preferred over surface electrode because of their electrophysiologic properties. Needle electrodes have a smaller surface area, which increase their impedance properties, increasing their overall electrophysiologic properties making them less susceptible to contamination by adjunct muscles and movement artifact created by surgical manipulation. Jacobs and Finkel stated that using bipolar needle electrodes allows for the recording of a smaller volume of muscle, which reduces the risk of artifact caused by breathing or muscle contraction of neighboring muscles. In addition, bipolar recordings from needles inserted into each vocal cord allow for discrete unilateral recordings of each RLN separately. Tschopp and Gottardo , comparing surface electrodes with needle electrodes, found larger-amplitude EMG potentials from the transligament and endolaryngeal electrode, which are both needle and fine-hook wire electrodes.
Needle electrodes are not without disadvantages. Placement of endolaryngeal needle electrodes can become quite challenging and requires a skilled surgeon . Inserted needles are susceptible to dislocation of the electrodes during muscle contraction. Pearlman and colleagues pointed out that the risk of using needle electrodes includes electrode displacement resulting in vocal cord hematomas, lacerations, needle breakage, and possible inadvertent rupture of the endotracheal tube balloon.
Surface electrodes have gained widespread use in the field of intraoperative monitoring for recording laryngeal muscles ( Fig. 2 ). Two types of surface electrodes are commonly used. These include postcricoid surface electrodes and intralaryngeal surface electrodes that are integrated into the endotracheal tube. Tschopp and Gottardo found surface electrodes to be an inferior recording method to needle electrodes. On direct nerve stimulation, EMG potentials from surface electrodes tend to be smaller in amplitude compared with needle electrodes. This is often attributed to the impedance properties of the electrodes. They also postulated that mucus secretions further impede transmission of the EMG signal . Neural monitoring ready endotracheal tubes can be purchased with surface electrodes fully integrated. These ready-made endotracheal tubes are considerably more expensive than standard endotracheal tubes. An alternative is to attach surface electrodes directly onto a standard endotracheal tube. One of the concerns regarding the use of surface electrodes (whether integrated or attached) is the possibility of tube migration during surgery, which significantly reduces the sensitivity of the surface electrodes because placement is no longer optimal. Johnson and Goldenberg reported the concurrent use of two serially placed intralaryngeal surface electrodes for RLN recordings ( Fig. 3 ). They concluded that this technique not only guards against tube migration, but also allows for the ability to acquire side-specific information. Overall, surface electrodes are deemed less invasive than the use of needle electrodes .




