Intraoperative Floppy Iris Syndrome—A Review and Video
David F. Chang
The author has no direct financial interest in any material or method mentioned. Dr. Chang is a consultant for Advanced Medical Optics and Alcon.
Introduction
In 2005, John Campbell and I first described a new small pupil syndrome that we named intraoperative floppy iris syndrome (IFIS).1 In addition to a tendency for poor pupil dilation, we described a triad of intraoperative signs that characterized classic IFIS:
A flaccid iris stroma that undulates and billows in response to ordinary intraocular fluid currents (Fig. 5.1).
A propensity for the floppy iris stroma to prolapse toward the phaco and side-port incisions, despite proper wound construction (Fig. 5.1).
Progressive intraoperative pupil constriction despite standard preoperative pharmacologic measures designed to maximize dilation (topical cycloplegics, phenylephrine, and nonsteroidal anti-inflammatory medications) (Fig. 5.1).
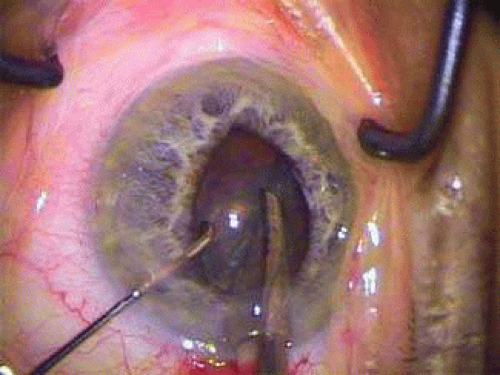 FIGURE 5.1 Tamsulosin patient with severe IFIS (iris billowing, iris prolapse, and intraoperative pupil constriction). |
We first reported the strong association of IFIS with the systemic alpha-1 antagonist tamsulosin (Flomax®, Boehringer-Ingelheim Pharmaceuticals, Inc., Ridgefield, CT).1 Tamsulosin is the most commonly prescribed drug worldwide for the treatment of lower urinary tract symptoms of benign prostatic hyperplasia (BPH). Several additional published studies have since confirmed this association.2,3,4,5,6,7,8,9,10,11
Initial Study
In order to study and characterize IFIS and possible pharmacologic associations, Dr. Campbell and I performed two separate parallel clinical studies.1 A retrospective chart review of all consecutive cataract surgeries performed in Dr. Campbell’s two-surgeon practice over a 12-month period (706 eyes in 511 patients) was used to assess the percentage of cataract patients on systemic sympathetic alpha-1 antagonist medications, as well as the percentage of these eyes that manifested IFIS. The overall incidence of IFIS was 2.3%. Three percent (16/511) of the patients, representing 3% (25/706) of the total eyes, were taking tamsulosin for BPH. IFIS was noted intraoperatively in 64% (16/25) of the tamsulosin eyes, but in none of the 15 eyes from patients taking other systemic alpha-1 blockers (prazosin, terazosin, and doxazosin). Poor preoperative dilation was common among patients on systemic alpha-1 blockers, as 68% (27/40) if the eyes had either poor, or moderately poor dilation noted in the records. Posterior capsular rupture and vitreous loss occurred in 2 of the 16 eyes with IFIS for an incidence of 12%.
A separate prospective study of 900 consecutive cataract surgeries performed by myself was used to determine the incidence and common characteristics of IFIS, and the percentage of these patients who were taking alpha-1 antagonist medications.1 Unless IFIS had been previously noted in the opposite eye (6 cases), I was masked preoperatively as to whether patients were taking alpha-1-antagonist drugs. Twenty-one eyes were diagnosed with IFIS (2.3% of the 900 cases). Nineteen of these cases were in patients who were taking or had taken systemic tamsulosin.
In all, a total of 35 eyes in the two studies had IFIS associated with systemic tamsulosin use. These eyes represented approximately 2% to 3% of the entire cataract surgical population from these two practices. Of the 37 total eyes diagnosed with IFIS in the two combined surgical series, 43% had brown irides, 57% had blue or blue-green irides, and all patients were male. Pseudoexfoliation was present in 5% of these eyes, and 19% of the IFIS cases occurred in diabetic patients.
Causes of IFIS
Subsequent clinical studies confirmed our original finding that IFIS is most commonly associated with the use of systemic alpha-1 adrenergic antagonists, such as tamsulosin.1,2,3,4,5,6,7,8,9,10,11 Subsequent clinical studies, however, have reported widely varying rates of IFIS occurring in tamsulosin patients.1,2,3,4,5,6,7,8,9,10,11 One likely reason is that there is significant variability in the severity of IFIS and the clinical definition is very subjective. All three classic clinical signs are present in severe IFIS, but not in milder cases. In addition, retrospective chart reviews typically relied on operative reports to identify iris prolapse, which may not always have been recorded. Many of these studies evaluated time periods prior to our first report of IFIS, when surgeons would have been less aware of the significance of iris billowing and prolapse. I subsequently organized a large prospective study of tamsulosin patients presenting for cataract surgery, which enrolled 167 eyes in 135 patients at 10 different surgical practices.8 Using a standardized IFIS grading scale, 90% of the eyes enrolled were diagnosed with IFIS as defined by the presence of at least one of the clinical triad of intraoperative signs.
Tamsulosin is one of several systemic alpha–1-adrenergic antagonists used to treat the lower urinary tract symptoms of benign prostatic hyperplasia (BPH). The first alpha-adrenergic blockers approved in the United States for BPH were the alpha-1 antagonists, terazosin (Hytrin®; Abbott Laboratories, Inc., North Chicago, IL), and doxazosin (Cardura®; Pfizer Inc, New York).12 The newest, non–subtype-selective alpha-1 blocker, alfuzosin (Uroxatral®; Sanofi-Aventis, Paris, France) was approved for BPH and launched in November 2003.13
These drugs improve urinary outflow by relaxing the smooth muscle in the prostate and bladder neck. Improved bladder emptying reduces the frequency of micturition in patients with BPH, which is particularly desirable at night. Because vascular smooth muscle contraction is also mediated by the alpha-1 adrenoreceptor, postural hypotension is a common and potential side effect of systemic alpha blockers used to treat the lower urinary tract symptoms of BPH. So-called uroselective drugs are those that improve urinary outflow while minimizing vascular side effects such as postural hypotension.
At least three different human alpha–1-receptor subtypes have been identified using binding and molecular cloning techniques—alpha-1A, alpha-1B, and alpha-1D.14 Their distribution varies among different human organs. Approximately 70% of the alpha-1 receptors in the human prostate are of the alpha-1A subtype.15 Based on animal and in vitro data, tamsulosin has a 20-fold greater affinity for alpha-1A than alpha-1B receptors.14 For this reason, tamsulosin is more uroselective, with fewer cardiovascular side effects compared to terazosin and doxazosin, which are not subtype-selective alpha-1 blockers. Tamsulosin, however, is the only alpha-1A subtype-selective blocker to be approved in the United States with BPH as its sole indication, and rapidly became the most commonly prescribed medication for this condition.16
The distribution of alpha-receptor subtypes in the human iris smooth dilator muscle is not known. There is indirect evidence that rabbits and humans have similar iris alpha-1 adrenoreceptors17,18 and that alpha-1A is the dominant adrenoreceptor subtype in rabbits.18,21 We postulated that systemic tamsulosin-blocked contraction of the iris dilator smooth muscle, leading to poor pupillary dilation. A lack of dilator smooth muscle tone would explain the iris floppiness and propensity to prolapse. A lack of dilator smooth muscle tone would explain the iris floppiness and propensity to prolapse. Tamsulosin did not alter the thickness of dilator muscle in a series of patients examined histologically (Destafeno JJ, Kim T. The Effect of Alpha1-adrenergic Receptor Antagonist Tamsulosin (Flomax) on Iris Smooth Dilator Muscle Anatomy. Poster, American Academy of Ophthalmology Annual Meeting, 2006). An interesting case report suggests that tamsulosin might also affect the alpha-1 receptors in the choroid as well.22
Anecdotal reports have demonstrated that IFIS can occur in patients taking the nonselective alpha-1 antagonists as well.4,5,6,7,8,9,10,23,24,25 This indicates that IFIS is a potential complication for this entire class of drugs used to treat BPH.26,27 IFIS has also been associated with the herbal BPH remedy, saw palmetto.28,29 A variety of other medications, including antipsychotic drugs, and other drugs possessing alpha-antagonist effects have been reported as being associated with single cases of IFIS.30,31,32,33,34,35 Because alpha-1 blockers are also prescribed for urinary retention or hypertension in women, it is important to remember that IFIS can arise in either sex.1,5,36,37
In comparison to tamsulosin, IFIS appears to be less frequent and less severe in patients taking nonselective alpha-adrenergic medications.1,4,5,6,7,8,9,10,38,39 In a retrospective chart review of 1,298 cataract patients, tamsulosin accounted for only 26% of the alpha-blockers used, but 71% of the cases with intraoperative iris prolapse.4 Chadha et al. performed a prospective study of 1,786 patients undergoing cataract surgery.6 They found that IFIS occurred in 57% of patients taking tamsulosin, but in only 2% of patients taking nonspecific 1 α1-antagonists. In a prospective study of 1968 cataract surgeries, Oshika et al. found the incidence of IFIS to be 43% in patients taking tamsulosin, compared to 19% in patients taking naftopidil, a nonselective α1– antagonist.7 In another prospective study, Herd reported a 37% incidence of IFIS among doxazosin patients, compared to 83% among tamsulosin patients.9 Finally, Blouin et al. looked retrospectively at 64 patients (92 eyes) who had been taking either tamsulosin or alfuzosin at the time of their cataract surgery.10 IFIS was noted in 86% of the tamsulosin patients compared to only 15% of the alfuzosin patients (p < .001).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


