Fig. 10.1
Intraocular lymphoma manifesting mainly vitreous opacification. (a) Fundoscopic examination shows characteristic vitreous opacities spreading radially to the periphery of the fundus. (b) Dynamic examination of vitreous opacities using a scanning laser ophthalmoscope shows an image resembling aurora
Features of Subretinal Lesion
Typically, lymphoma cells infiltrate beneath the retinal pigment epithelium and show patchy lesions yellowish-white in color. In the initial disease stage, tiny infiltrates like small exudates can be seen in uveoretinitis (Fig. 10.2). These lesions increase in number over time and become slightly elevated (Fig. 10.3). In some cases, the lesions fuse and expand, forming a widespread lesion in the fundus (Fig. 10.4). Characteristic brownish pigments (so-called leopard spots) are often observed in the yellowish-white lesions (Figs. 10.4 and 10.5). These subretinal lesions may reduce in size or become atrophic over time with or without treatment (Fig. 10.5). Once these atrophic changes involve the macular area, significant disturbance of visual acuity may occur.
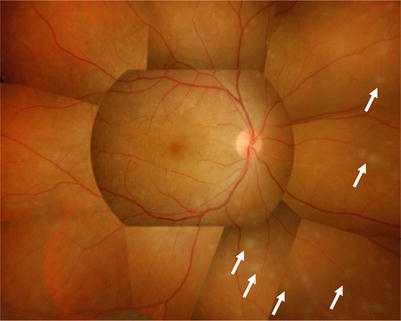
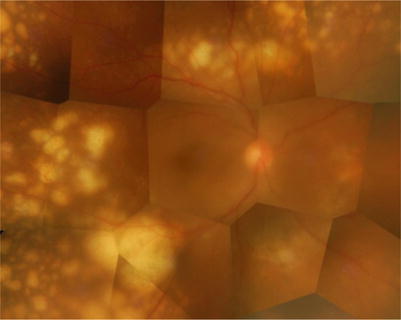
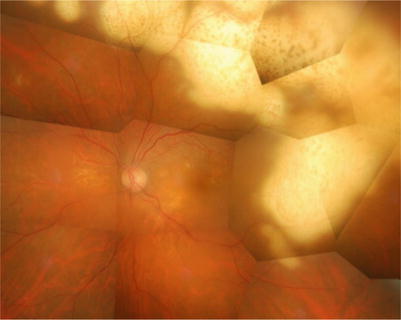
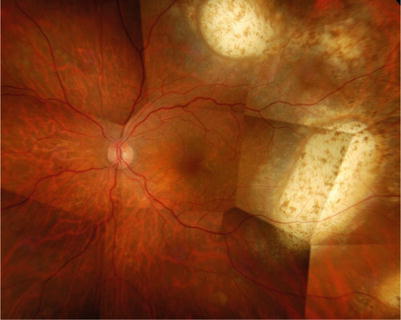
Fig. 10.2
Intraocular lymphoma manifesting subretinal infiltration. In the early stage, small exudative lesions (arrow) that are seen in uveoretinitis are observed
Fig. 10.3
The subretinal lesions increase in number gradually and tend to fuse and expand
Fig. 10.4
The lesions fuse and may form a widespread infiltrative lesion
Fig. 10.5
Irrespective of treatment or no treatment, subretinal lesions gradually become atrophic forming scars (same case as in Fig. 10.4)
On fluorescein angiography, various findings indicating damage of the retinal pigment epithelium by infiltrating cells can be observed. Hypofluorescence as a result of blockade by subretinal lesion as well as granular hyperfluorescence and late staining due to disturbance at the level of retinal pigment epithelium are some of the typical findings. Even though ophthalmoscopic examination reveals no obvious abnormalities, fluorescein angiography may depict hypofluorescence and hyperfluorescence (Fig. 10.6). Unlike uveitis, cystoid macular edema is rarely seen [9].
Fig. 10.6
Intraocular lymphoma manifesting subretinal infiltration. Even though ophthalmoscopic findings show no obvious abnormalities (a), fluorescein angiography detects hypofluorescence or hyperfluorescence (b)
Optical coherent tomography (OCT) can detect granular lesions at retinal pigment epithelium level in the early disease stage (Fig. 10.7a) and subretinal lesions between the retinal pigment epithelium and Bruch’s membrane reflecting histopathological features [10]. Therefore, OCT may be useful in the diagnosis and monitoring of the progression or regression of intraocular lymphoma with retinal involvement [11].
Fig. 10.7
Optical coherent tomography (OCT) detects the presence of lesion beneath the retinal pigment epithelium (arrowhead) (a). In the very early stage, tiny granular lesions are observed at the level of retinal pigment epithelium (b)
Recently, the utility of fundus autofluorescence (FAF) in the assessment of disease activity has been reported [12].
Reaction in the Anterior Segment
Many patients with primary intraocular lymphoma have little or no anterior segment inflammation. During relapse, however, cell infiltration in the anterior chamber together with fine, coarse, and reticular keratic precipitates often with spinous margin may be present (Fig. 10.8).
Fig. 10.8
During relapse, cells in the anterior chamber together with coarse and reticular keratic precipitates are observed (a). Confocal microscopy depicts clearly the reticular structure of keratic precipitates (b)
Optic Disk Swelling
Lymphoma cells infiltrate the optic disk and its surrounding, which may cause hyperemia and swelling of the optic disk and further retinal exudative change around the optic disc.
Retinal Hemorrhage
Retinal hemorrhage is uncommon at the initial onset of intraocular lymphoma or during the early stage of primary disease, but hemorrhage may be found during relapse or in untreated cases in which the disease has advanced. When retinal hemorrhage is present with yellowish-white infiltrative lesions, differentiation from cytomegalovirus retinitis and other conditions is necessary (Fig. 10.9).
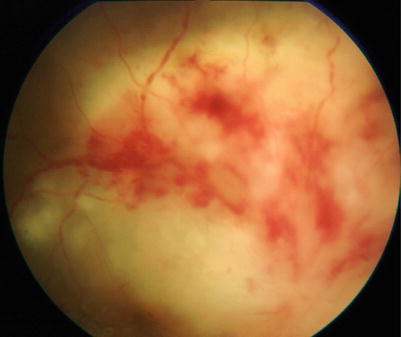
Fig. 10.9
In a case with hemorrhage accompanied by severe subretinal lesion, differentiation from infectious uveoretinitis such as cytomegalovirus retinitis is an issue
Retinal Vasculitis (Sheathing of Retinal Vessel)
Although rare, sheathing of retinal vessels resembling retinal vasculitis may be observed. The sheathing may arise from infiltration of lymphoma cells to the vascular wall, while reactive vasculitis is also a possibility.
Diagnosis
Intraocular lymphoma should be considered when an elderly patient presents with ocular findings described above and is unresponsive to corticosteroid therapy. Examination of intraocular fluids and/or tissue is necessary for a definitive diagnosis.
When Vitreous Opacification Is Present
When cells are observed in the vitreous body, perform a conventional vitrectomy to collect the cells for use in diagnostic investigations. Vitrectomy also has therapeutic significance, because vitreous excision can be performed to improve visual function in patients with severe opacification. Vitrectomy can be conducted satisfactorily using small-gauge vitreous cutters such as a 25-gauge system, but setting a lower cutting rate is desirable to minimize destruction of the infiltrating cells. While exercising care to prevent complications, collect 0.5–1 ml of undiluted vitreous fluid. This sample is used for the following investigations: (1) morphological evaluation of infiltrative cells (cytology), (2) measurement of cytokines, and (3) detection of clonal rearrangement of the heavy chain gene by PCR in the case of B-cell lymphoma or detection of T-cell receptor (TCR) in the case of T-cell lymphoma. Other studies may also be conducted, such as (4) flow cytometry to examine surface markers of infiltrating cells and (5) detection of chromosomal abnormalities. For (3), (4), and (5), vitreous sample diluted with irrigation fluid may also be used.
Cytological examination is essential for the diagnosis of intraocular lymphoma. The lymphoma cells are characterized by large and pleomorphic nuclei with prominent nucleoli (Fig. 10.10). However, according to a study of a large series, cytology was sufficient to provide a diagnosis of intraocular lymphoma in only 48 % of all cases [4]. The reason is that vitreous cells consist of a mixture of neoplastic lymphocytes, inflammatory cells, and necrotic cells [6], which may confound diagnosis. While the neoplastic cells are mainly CD20-positive cells derived from B cells, a certain number of T cells also coexist in the vitreous [13], and assessment of the degree of atypia of the infiltrating lymphocytes depends on the subjective judgment of the pathologist, which is a major issue of cytological diagnosis. In addition, neoplastic cells obtained by vitrectomy may be fragile, lytic, and necrotic, which is another factor rendering cytological diagnosis difficult. In many cases, before a biopsy is conducted, the patient would have been treated with corticosteroids under a presumptive diagnosis of “uveitis,” and corticosteroids are known to induce apoptosis in lymphoma cells [14], which may also affect the efficacy of cytological diagnosis.
Fig. 10.10
Neoplastic lymphoma cells obtained by vitrectomy demonstrating large, pleomorphic nuclei (a). Infiltrating cells are positive for the B-cell antigen CD20 (b)
Biochemical analysis of the intraocular fluid is critical for the diagnosis of intraocular lymphoma. High intraocular level of interleukin (IL)-10 or high IL-10/IL-6 ratio supports a diagnosis of intraocular lymphoma [3, 11]. However, for intraocular lymphoma secondary to systemic malignant lymphoma, IL-6 level may be higher than IL-10 level. Furthermore, while a high IL-10 level in aqueous humor has diagnostic value, a low level does not exclude a possibility of intraocular lymphoma.
Most intraocular lymphomas are of B-cell origin. Therefore, another useful test is to extract DNA from B lymphocytes and amplify with PCR using primer corresponding to the CDR3 IgH variable region, for detecting clonal rearrangement of the heavy chain gene [1–3].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


