 Questions
Questions
1. Adaptive immunity
a. works in an antigen-independent manner.
b. is preprogrammed by evolution.
c. is based on environmental stimulus.
d. uses only nonspecific macrophages and PMNs to destroy offending agents.
2. Which of the following lymphocytes has cytotoxic activity without a specific antigen receptor and is not antigen specific?
a. T lymphocytes.
b. B lymphocytes.
c. natural killer (NK) cells.
d. macrophages.
3. Which of the following is exclusively part of the adaptive immunity system?
a. antigen memory.
b. use of macrophages/neutrophils to combat offending agents.
c. inflammatory response.
d. leukocyte receptor activation.
4. Which of the following cells are used by only the adaptive immunity system?
a. monocytes.
b. lymphocytes.
c. neutrophils.
d. eosinophils.
5. The first cell that an antigen typically comes in contact with during the cascade of the immune response is the
a. NK cell.
b. T lymphocyte.
c. B lymphocyte.
d. macrophage.
6. A 70-year-old man infected with virus A. He has never been exposed to this virus in the past. What subtype of immunoglobulin will be made in response to the initial exposure to the virus?
a. IgA.
b. IgD.
c. IgM.
d. IgG.
7. Which type of immunoglobulin will the man in question 6 form against virus A other than IgM?
a. IgA.
b. IgD.
c. IgE.
d. IgG.
8. Class I MHC
a. are present on almost all nucleated cells.
b. refer to HLA-DR, HLA-DP, and HLA-DQ.
c. work with CD4 helper T cells.
d. are best at processing endocytosed antigens.
9. What is the most abundant antibody subtype present in the tear film?
a. IgE.
b. IgM.
c. IgA.
d. IgG.
10. The major histocompatibility antigen complex in humans (human leukocyte antigen [HLA] system) is coded for by genes located on chromosome
a. 6.
b. 11.
c. 13.
d. 18.
11. What component of the conjunctiva is the most important for immune regulation?
a. epithelium.
b. substantia propria.
c. lymphoid tissue.
d. goblet cells.
12. Presumed ocular histoplasmosis syndrome is associated with which HLA marker?
a. A29.
b. B5.
c. B7.
d. B8.
13. Sympathetic ophthalmia (S.O.) and Vogt-Koyanagi-Harada (VKH) syndrome are associated with which HLA marker?
a. B5.
b. B44.
c. B51.
d. DR4.
14. Which immunoglobulin class has the highest individual molecular weight?
a. IgA.
b. IgD.
c. IgE.
d. IgM.
15. Which immunoglobulin molecule has the longest serum half-life?
a. IgA.
b. IgM.
c. IgE.
d. IgG.
16. Which is the most abundant immunoglobulin class to cross the human placenta?
a. IgA.
b. IgD.
c. IgE.
d. IgG.
17. What is the most common type of uveitis?
a. anterior.
b. intermediate.
c. posterior.
d. panuveitis.
18. Anaphylactoid reactions are grouped into what type of hypersensitivity reactions?
a. type I.
b. type II.
c. type III.
d. type I V.
19. What type of hypersensitivity is associated with immune-complex reactions?
a. type II.
b. type III.
c. type I V.
d. type V.
20. Which immunoglobulin class is probably the oldest phylogenetically?
a. IgA.
b. IgD.
c. IgM.
d. IgG.
21. What type of cells have a particular affinity for IgE immunoglobulins?
a. eosinophils.
b. mast cells.
c. basophils.
d. macrophages.
22. Which of the following medications is an alkylating agent?
a. cyclophosphamide.
b. methotrexate.
c. azathioprine.
d. mycophenolate mofetil.
23. Which complement component is present in the highest serum concentrations?
a. C1q.
b. C3.
c. C4.
d. C5.
24. What complement component is part of the membrane attack complex?
a. C3a.
b. C4a.
c. C5a.
d. C6.
25. Which of the following substances is NOT produced by the cyclooxygenase pathway?
a. prostacyclins.
b. thromboxane.
c. leukotrienes.
d. prostaglandins.
26. What complement component begins the complement pathway?
a. C3a
b. C3b.
c. C4a.
d. C5a.
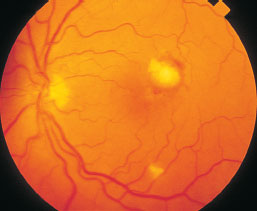
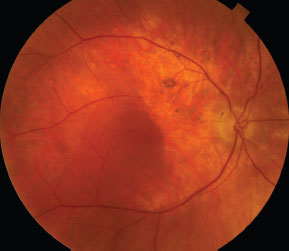
27. A 50-year-old man presents with decreased vision. His medical history is positive for endstage AIDS and current IV drug use. His fundus photo is present below. What is the diagnosis?
a. Candida endogenous endophthalmitis.
b. CMV retinitis.
c. ocular lymphoma.
d. HIV retinopathy.
28. The Arthus reaction is what type of hypersensitivity?
a. I.
b. II.
c. III.
d. I V.
29. Immune recovery uveitis (IRU)
a. occurs in patients with HZV and HSV retinitis.
b. occurs only in CMV-infected eyes.
c. does not cause macular edema.
d. does not cause epiretinal membrane formation.
30. Graves’ disease is a manifestation of what type of hypersensitivity?
a. type I.
b. type II.
c. type IV.
d. type V.
31. Which immunoglobulin has NOT been detected in tear samples?
a. IgA.
b. IgD.
c. IgE.
d. IgG.
32. Wessely rings represent what type hypersensitivity?
a. type I.
b. type II.
c. type III.
d. type IV.
Questions 33–36. Refer to vignette below. A 34-year-old man presents with a 1-week history of right eye pain and light sensitivity. The left eye is without symptoms. There are 2+ cells and 2+ flare in the anterior chamber. There is no posterior inflammation present. Upon further questioning, he has had lower back stiffness and pain upon awakening for several years. The back pain improves during the day. He has no other general medical symptoms. His social history is negative for promiscuous sexual history.
33. What is the most likely diagnosis?
a. syphilis.
b. Reiter’s syndrome.
c. ankylosing spondylitis.
d. toxoplasmosis.
34. What radiographic test would be appropriate and most cost effective in this scenario?
a. CT scan of head.
b. MRI of spinal column.
c. sacroiliac x-ray films.
d. CT scan of thoracic spine.
35. What percentage of patients with this pathology possess the HLA-B27 gene?
a. 10%.
b. 25%.
c. 50%.
d. over 75%.
36. Not including the eye and lumbosacral spine, what other area may rarely be inflamed?
a. heart.
b. brain.
c. kidneys.
d. aorta.
37. Which of the following is INCORRECT regarding Dalen-Fuchs nodules?
a. They consist of RPE and epitheloid cells.
b. They are present in sympathetic ophthalmia.
c. They are present in Vogt-Koyanagi-Harada syndrome.
d. They are present in Behcet’s disease.
38. The most common cause of anterior uveitis in the adult population is
a. herpes simplex keratouveitis.
b. idiopathic.
c. HLA-B27 iridocyclitis.
d. herpes zoster.
39. The most common cause of posterior uveitis in the adult population is
a. toxocariasis.
b. sarcoidosis.
c. toxoplasmosis.
d. idiopathic posterior uveitis.
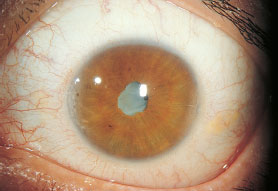
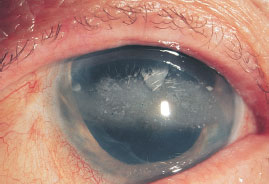
40. Patient presents with unilateral anterior segment uveitis. On slit-lamp exam, the corneal endothelium is diffusely covered with stellate KPs. There are 1+ cells in the anterior chamber. The iris has atrophy. There are no iris nodules or posterior synechiae. What is the most likely diagnosis pictured below?
a. syphilitic uveitis.
b. HLA-B27 uveitis.
c. Fuchs’ iridocyclitis.
d. sarcoidosis.

41. Which of the following is true regarding the condition seen above?
a. Hyphema may be seen after cataract surgery.
b. There is no association with glaucoma or cataract.
c. The majority of cases need aggressive steroid treatment.
d. Patient’s usually have severe discomfort when the condition is active.
42. Which condition below has inflammation that primarily affects the venules?
a. Eales’ disease.
b. systemic lupus erythematosus.
c. acute retinal necrosis.
d. polyarteritis nodosa.
43. Which of the following is true regarding Reiter’s Syndrome?
a. There are only three major diagnostic criteria.
b. The syndrome can be triggered by dysentery.
c. Iritis is the most common finding in Reiter’s syndrome.
d. The syndrome has no dermatologic manifestations.
44. Which of the following conditions are NOT associated with iris nodules and skin findings?
a. sarcoidosis.
b. juvenile xanthogranuloma.
c. neurofibromatosis.
d. pseudoxanthoma elasticum.
45. The most common cause of decreased vision in intermediate uveitis is
a. disc edema.
b. posterior subcapsular cataract.
c. vitritis.
d. cystoid macular edema.
46. The prevalence of HLA-B27 in the general population is
a. 1%–8%.
b. 10%–25%.
c. 25%–50%.
d. 50%–75%.
47. Which of the following antiretroviral agents has been shown to increase the CD8+ lymphocyte count in HIV-positive patients?
a. zidovudine (ZDV, AZT).
b. ritonavir.
c. didanosine (ddI).
d. zalcitabine (ddC).
48. What is false regarding Fuchs’ uveitis syndrome?
a. Glaucoma is common in this condition.
b. Synechiae are commonly observed in this condition.
c. Cataract is common in this condition.
d. Vitreous and retinal findings may be present.
49. What is the probability, given HLA-B27 genotype, of sacroiliac disease?
a. <5%.
b. 10%.
c. 25%.
d. 50%.
50. The most important component of long-term therapy in a young man who is HLA-B27 positive is
a. cardiac ultrasound.
b. annual tonometry.
c. systemic (oral) nonsteroidal antiinflammatory therapy.
d. physical therapy.
51. Which one of the following concerning Reiter’s syndrome is false?
a. 90% of cases are in men.
b. It may follow a bout of either urethritis.
c. Skin lesions are present at times.
d. The most common ocular finding is an acute nongranulomatous anterior uveitis.
52. Which of the following is true regarding acute iritis?
a. It is more frequently present in Crohn’s disease compared to ulcerative colitis.
b. It is usually present in psoriatic patients without arthritis.
c. It can occur with nephritis.
d. Signifies only inflammation and NOT infection.
53. The patient below is a 4-year-old girl. What is the most likely diagnosis?
a. sarcoidosis.
b. syphilis.
c. toxocara.
d. juvenile rheumatoid arthritis.
54. Which of the following lab values are most consistent with the clinical scenario presented in question 53?
a. ANA+, RF+.
b. ANA+, RF-.
c. ANA-, RF+.
d. ANA-, RF-.
55. Which of the following is NOT a risk factor for developing iridocyclitis in JRA?
a. associated type I diabetes.
b. pauciarticular arthritis.
c. female gender.
d. ANA positivity.
56. Which of the following is usually false with regard to JRA?
a. Still’s disease has a low rate of uveitis.
b. The involved eye is red and inflamed.
c. Methotrexate is a possible treatment option.
d. Cataract formation is a major issue in management of these children.
57. Which one of the following concerning Behçet’s disease is false?
a. The disease is more common among Japanese than Americans.
b. The classic acute uveitis of Behçet’s disease is typically associated with a hypopyon.
c. Anterior uveitis is more common in Behçet’s disease in men than posterior uveitis.
d. Characteristic aphthous ulcers develop on mucous membranes, including the mouth and genital tract.
58. Which of the following is true regarding Behçet’s disease?
a. The course of the ocular disease generally is self-limited.
b. There is no cardiovascular association in Behçet’s disease.
c. A shifting hypopyon may be present in the anterior chamber.
d. Steroids are generally the only long-term therapy.
59. The patient at the top of the right column presents to the clinic. What is the diagnosis?
a. episcleritis.
b. oculodermal melanocytosis.
c. conjunctival melanoma.
d. scleromalacia perforans.

60. Which one of the following concerning Kawasaki’s disease is false?
a. The vast majority of affected patients are children under the age of 10 years.
b. The hallmark of the eye findings is a bilateral conjunctival congestion that spares the limbus.
c. The hallmark of the dermatologic findings is a shedding rash affecting the extremities.
d. Corticosteroids are agents of choice to treat the underlying disease.
For Questions 61–64, refer to the below given photograph.
A 10-year-old boy presents with the complaint of new floaters in both eyes. He has stated his vision is blurry at school. He has previous had no refractive error. Upon workup, he has no systemic illness. On exam there are white clumps of debris seen inferiorly at the vitreous base in both eyes.
For Questions 61–64, refer to vignette and clinical photograph on page 160 (bottom of the right column).

61. Which of the following is true regarding the clinical scenario?
a. It is the most common form of intermediate uveitis.
b. There is usually a definable cause.
c. It is present in young people only.
d. There are no HLA associations.
62. What is a major cause of vision loss in patients with this process?
a. venous sheathing.
b. chronic cystoid macular edema.
c. retinal venous sheathing.
d. anterior chamber cells.
63. What medical condition is associated with this process?
a. syphilis.
b. sarcoidosis.
c. toxocariasis.
d. multiple sclerosis.
64. First line therapy for this process is usually which of the following?
a. laser ablation.
b. methotrexate.
c. corticosteroids.
d. cryotherapy.
65. Which of the following generally does NOT occur in patients with lupus?
a. choroidal neovascularization.
b. choroidal infarction.
c. nerve fiber layer infarct.
d. retinitis.
66. In reference to Wegner’s granulomatosis, which of the following is false?
a. Skin involvement can occur.
b. P-ANCA is a diagnostic test for this disease.
c. Glomerunephritis is a serious issue in these patients.
d. Uveitis may be anterior, intermediate, or posterior in this disease.
67. The patient presents with blurred vision, photophobia, and the below findings. What is the most likely diagnosis?
a. herpes.
b. Behçet’s disease
c. sarcoidosis.
d. reactive arthritis.

For Questions 68–71, refer to vignette and clinical the below given photograph.
A 69-year-old woman presents with decreased vision in both eyes. She states she has noted more floaters lately in both eyes. She is also having difficulty driving at night.
For Questions 68–71, refer to vignette and clinical photograph on page 161 (bottom of the right column).
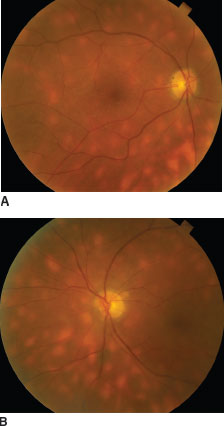
68. Which of the following is true regarding the vignette and clinical photos referenced above?
a. It is also called vitiliginous chorioretinitis.
b. It is commonly seen in African American patients.
c. The lesions pigment over time.
d. ERG is usually normal.
69. What percentage of the general population is HLA A-29 positive?
a. 1.
b. 7.
c. 50.
d. 90.
70. Which one of the following is not a late complication of this disease?
a. epiretinal membrane.
b. optic nerve disease.
c. severe vitritis.
d. choroidal neovascularization.
71. Which of the following is true about the vignette and clinical photos referenced above?
a. Optic nerve head edema is not present.
b. Progressive visual field loss can occur despite the clinical appearance of inactivity.
c. More lesions are seen on clinical exam than on indocyanine green angiography.
d. Color vision and night vision are not affected.
72. Which one of the following concerning the manifestations of sarcoidosis is false?
a. The anterior uveitis of sarcoidosis is without posterior synechiae formation.
b. A classic orbit/adnexal finding is bilateral painless enlargement of the lacrimal glands.
c. The most commonly involved organ system is the pulmonary system.
d. “Candle-wax” drippings (taches de bougie) are actually irregular granulomas along retinal Venules
73. Laboratory tests that are NOT useful in the evaluation of the patient with suspected sarcoidosis include
a. angiotensin-converting enzyme (ACE).
b. serum lysozyme (muramidase).
c. chest x-ray.
d. antineutrophil cytoplasmic antibody assay.
74. Which of the following is not a characteristic finding of sarcoidosis?
a. skin lesions.
b. caseating granulomas.
c. conjunctival nodules.
d. snowballs in vitreous.
75. Which nerve palsy is classically associated with systemic sarcoidosis?
a. oculomotor.
b. trigeminal.
c. abducens.
d. facial.
76. Which of the following is true regarding acute posterior multifocal placoid pigment epitheliopa-thy (APMPPE)?
a. It is a unilateral disease.
b. The lesions are located in the retina.
c. There is an association with cerebral vasculitis.
d. Fluorescein angiography does not aid in diagnosis.
77. What are the characteristic fluorescein angiogra-phy findings in APMPPE?
a. early hypofluorescence, late hyperfluorescence.
b. early hypofluorescence, late hypofluorescence.
c. early hyperfluorescence, late hypofluorescence.
d. early hyperfluorescence, late hyperfluorescence.
78. Which one of the following concerning congenital syphilis is true?
a. The interstitial keratitis of congenital syphilis is generally bilateral and asymptomatic.
b. Syphilitic interstitial keratitis is a direct manifestation of active corneal infection.
c. The chorioretinitis of congenital syphilis is generally bilateral and nonprogressive.
d. A diagnosis of syphilitic interstitial keratitis mandates a full course of treatment for neurosyphilis.
79. Which one of the following concerning acquired ocular syphilis is false?
a. The fluorescent treponemal antibody-absorption (FTA-Abs) is a useful measure of disease response to therapy.
b. Ocular findings may include iris nodules or vascularized papules.
c. The end stage of retinal vasculitis and inflam-mation may resemble retinitis pigmentosa.
d. Treatment of syphilitic uveitis is identical to that of neurosyphilis.
80. Which one of the following concerning Lyme disease is false?
a. The earliest eye finding is typically a follicular conjunctivitis.
b. The most common eye finding is a chronic iridocyclitis with vitreous cells.
c. Current serologic tests for Lyme disease are approaching >90% sensitivity.
d. The other organ systems commonly affected by Lyme disease include skin, central nervous system, cardiovascular, and musculoskeletal systems.
81. Which one of the following concerning ocular tuberculosis (TB) is true?
a. TB is the second most common cause of uve-itis in the United States.
b. The ocular inflammation associated with TB reflects a hypersensitivity reaction without active infection.
c. Skin testing is valuable in the diagnosis of tuberculous uveitis but may need to be repeated with higher concentrations of puri-fied protein derivative (PPD).
d. Eye disease is never seen in the setting of a normal chest x-ray.
82. Which one of the following concerning pars pla-nitis is false?
a. The majority of patients have unilateral involvement.
b. The majority of patients are under the age of 30 years.
c. The most common cause of decreased vision is cystoid macular edema.
d. It may be associated with systemic conditions such as Lyme disease, sarcoidosis, and multiple sclerosis.
83. Which of the follow is true regarding punctate inner choroiditis (PIC)?
a. It is classically seen in hyperopes.
b. The disease has associated vitritis.
c. It is a disease of the elderly.
d. Choroidal neovascularization can be a source of vision loss.
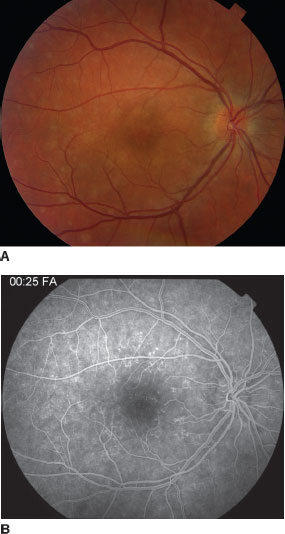
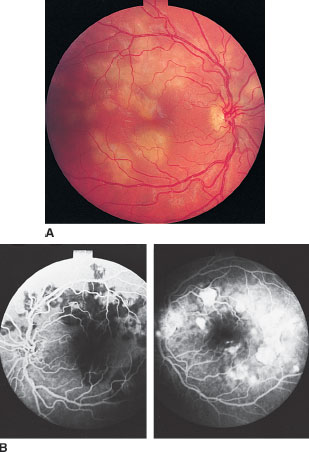
84. A 19 year-old woman presents with decreased vision and flashes in her right eye. The fundus photo and fluorescein angiogram are pictured below. What is the most likely diagnosis?
a. punctate inner choroiditis.
b. multiple evanescent white dot syndrome.
c. sarcoidosis.
d. acute zonal occult outer retinopathy.
85. The type of bacteria most commonly isolated in bleb-associated endophthalmitis is
a. Staphylococcus.
b. Neisseria.
c. Propionibacterium.
d. Streptococcus.
86. Which of the following is false in regards to endophthalmitis?
a. The Endophthalmitis Vitrectomy Study gives guidance for management of postoperative infectious endophthalmitis.
b. Endophthalmitis does not occur after extra-ocular surgery such as pterygium excision.
c. Endophthalmitis may come from an endogenous source.
d. Other uveitic conditions may masquerade as endophthalmitis.
87. What organism is classically implicated in the pathogenesis of chronic postoperative endophthalmitis?
a. Pseudomonas.
b. Neisseria
c. Propionibacterium acnes.
d. Serratia species.
88. Which endophthalmitis has the worst prognosis?
a. acute postoperative endophthalmitis.
b. chronic postoperative endophthalmitis.
c. posttraumatic endophthalmitis.
d. bleb-associated endophthalmitis.
89. The organism responsible for approximately 25% of posttraumatic endophthalmitis is
a. Staphylococcus aureus.
b. Streptococcus pneumoniae.
c. Aspergillus.
d. Bacillus cereus.
90. The organism with the poorest prognosis in post-traumatic endophthalmitis is
a. Staphylococcus aureus.
b. Streptococcus pneumoniae.
c. Aspergillus.
d. Bacillus cereus.
91. The picture below is a 60-year-old woman who complains of photopsias and blurred vision in both eyes. The left eye has similar changes. What is the diagnosis?
a. choroideremia.
b. acute zonal occult outer retinopathy (AZOOR).
c. multifocal choroiditis (MFC).
d. multiple evanescent white dot syndrome (MEWDS).
92. Which one of the following concerning fungal endophthalmitis is false?
a. Candida is the most common etiology.
b. The classic vitritis follows an earlier retinochoroiditis.
c. The majority of patients with endogenous Candida endophthalmitis will have positive blood cultures.
d. Approximately 10% of patients with candidemia will eventually develop endophthalmitis.
93. Which of the following is false regarding sympathetic ophthalmia?
a. It is associated with previous ocular surgery or trauma.
b. It characteristically affects the choriocapillaris.
c. It is associated with retinal detachments.
d. It is a diffuse ocular process.
94. Which of the following is false concerning Vogt-Koyanagi-Harada (VKH) disease?
a. Skin findings precede ocular disease.
b. Auditory symptoms may be present.
c. Retinal detachments may cause vision loss.
d. There is thickened choroidal signal on B-scan ultrasound.
95. Which one of the following concerning toxoplas-mosis is true?
a. The manifestations are strictly posterior in nature.
b. The retinal vessels are spared in ocular toxoplasmosis.
c. ELISA testing for antitoxoplasma antibodies is important in the diagnosis of atypical lesions.
d. The definitive hosts of Toxoplasma gondii is a species of small rodent.
96. Potential adverse affects of the pharmacologic management of toxoplasmosis include all of the following except
a. pseudomembranous colitis.
b. Stevens-Johnson syndrome.
c. aggravation of diabetes mellitus.
d. microcytic anemia.
97. Which one of the following regarding onchocer-ciasis is false?
a. Onchocerca volvulus is transmitted by the bite of the Simulium black fly.
b. Skin findings are rare in this condition.
c. Microfilariae may be seen swimming in the anterior chamber and may induce a severe anterior uveitis with glaucoma and cataract.
d. Chorioretinal and optic atrophy are common in advanced disease.
98. What is the most likely diagnosis in the patient pictured at the top of the right column?
a. syphilis.
b. herpetic disease.
c. scleritis.
d. sarcoidosis.

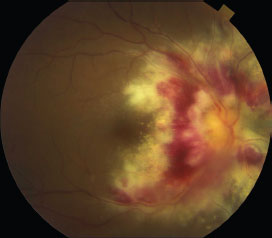
99. The picture below is from a 50-year-old man with AIDS. He is not on antiretroviral therapy. He presents with decreased vision and photopsias in the left eye. What is the most likely diagnosis given this clinical scenario?
a. sarcoidosis.
b. Lyme disease.
c. cytomegalovirus infection.
d. Behçet’s disease.
100. Which one of the following concerning cytomegalovirus (CMV) infection is false?
a. The congenital form may be heralded by fever, pneumonia, or hepatosplenomegaly.
b. The eye findings in congenital disease include cataract and peripheral retinal lesions, both atrophic and hyperpigmented.
c. Retinal detachment is uncommon in CMV retinitis.
d. Posterior segment involvement generally starts as a retinitis and secondarily involves the choroid.
101. Which of the following choices is NOT a therapeutic option for the above patient?
a. oral valganciclovir.
b. IV acyclovir
c. IV ganciclovir
d. intravitreal foscarnet.
102. Which of the following is not a risk factor for Candida endophthalmitis?
a. recent total parenteral nutrition.
b. intravenous drug abuse.
c. organ transplantation.
d. AIDS.
103. Which one of the following concerning acute retinal necrosis (ARN) is false?
a. Anterior segment inflammation is variable.
b. Posterior segment inflammation is generally heavy.
c. Retinal detachments associated with ARN may benefit from the use of tamponade with silicone oil.
d. Like other viral retinitides, affected patients are usually immunosuppressed.
104. The differential diagnosis for a patient with chronic vitreous cells does not include which of the following?
a. retinitis pigmentosa.
b. ocular histoplasmosis syndrome.
c. retinal detachment.
d. intraocular foreign body.
105. Nocardia asteroids
a. usually has only a localized abscess.
b. may present with pneumonia.
c. commonly affects the eye.
d. only causes a mild inflammatory response.
106. Which of the following concerning ocular toxocariasis is false?
a. The definitive host for the parasite is the dog or cat.
b. Ingested ova initially take up residence in the liver and lung.
c. Manifestations may include chronic endophthalmitis, localized macular granuloma, or localized peripheral granuloma.
d. Inflammation is usually bilateral.
107. Which of the following concerning the presumed ocular histoplasmosis syndrome (POHS) is true?
a. The maculopathy generally precedes the formation of peripheral punched out lesions, or “histo spots.”
b. The vitritis associated with the condition may decrease vision.
c. Fundus lesions in their acute phase represent a retinitis with a secondary choroidal reaction.
d. A patient with a macular histo spot has about a one-in-four chance of active maculopathy over the next 3 years.
108. A 23-year-old healthy young man with no medical problems presents with scotomas in both eyes. His vision is 20/25 in both eyes. He states he had a chest cold last week (images below). What is most likely the diagnosis?
a. sarcoidosis.
b. pars planitis.
c. acute multifocal posterior placoid epitheli-opathy (APMPPE).
d. Pneumocystis carinii.
109. Berlin’s nodules are located in which area of the eye?
a. pupillary border.
b. mid-iris.
c. conjunctiva.
d. angle.
110. Periocular steroid injection should be avoided in which of the following conditions?
a. pars planitis associated with sarcoidosis and cystoid macular edema.
b. necrotizing scleritis associated with rheumatoid arthritis.
c. cystoid macular edema following cataract surgery.
d. punctate inner choroidopathy.
111. Which of the following is false regarding diffuse unilateral subacute neuroretinitis (DUSN).
a. The causative worms are thought to be Ancylostoma canium and Baylisascaris procyonis.
b. Anti-helminthic medications are the only treatment options.
c. Reinfection may occur.
d. It is generally a unilateral condition.
112. What is false regarding the condition below?
a. It may occur in eyes that have undergone vitrectomy.
b. It may be seen in children.
c. It is not related to chronic inflammation.
d. Phthisical eyes may be associated with this condition.
113. What is the most common retinopathy seen in patients with HIV/AIDS?
a. toxoplasmosis.
b. cytomegalovirus retinitis.
c. Pneumocystis carinii retinitis.
d. HIV retinopathy.
114. The most common intraocular opportunistic infection associated with HIV infection is
a. toxoplasmosis.
b. acute retinal necrosis secondary to herpes simplex virus.
c. pneumocystis choroiditis.
d. CMV retinitis.
115. Which of the following is believed to be a sig-nificant risk factor for the development of pneu-mocystis choroiditis?
a. active Pneumocystis carinii pneumonia (PCP).
b. treatment of Pneumocystis carinii pneumonia with aerosolized pentamidine.
c. severe cachexia.
d. absolute lymphocyte count below 500 cells/mm3.
116. Kaposi’s sarcoma may present in what ocular structure?
a. retina.
b. choroid.
c. conjunctiva.
d. orbit.

117. In the patient photographed below, which of the following is the most likely diagnosis?
a. syphilitic uveitis.
b. herpes uveitis.
c. sarcoidosis.
d. toxoplasmosis.
118. The patient pictured below is a 26-year-old female with blurred central vision in the left eye. Her refractive error is -4.00 OU in both eyes. She has no other medical problems. What is the most likely diagnosis?
a. MEWDS.
b. Birdshot chorioretinopathy.
c. PIC.
d. Krill’s disease.

119. What percentage of patients with documented candidemia will develop Candida chorioretinitis?
a. 0%.
b. 5%.
c. 10%
d. 20%
120. Which of the following is true regarding intermediate uveitis and multiple sclerosis?
a. The incidence of uveitis in MS is approximately 1%.
b. Anterior uveitis is most commonly found in association with MS.
c. Macular edema is more common in association with MS.
d. HLA-DR51 is associated with MS and uveitis.
121. Clinical features distinguishing the progressive outer retinal necrosis (PORN) syndrome from the acute retinal necrosis (ARN) syndrome include each of the following, except
a. relative lack of vitreous inflammation.
b. relative lack of vasculitis.
c. relative early involvement of the macula.
d. better visual outcome.
122. One potential complication of cryotherapy for pars planitis is
a. exacerbation of vitritis.
b. exacerbation of posterior subcapsular cataract.
c. exacerbation of CME.
d. rhegmatogenous retinal detachment.
123. Each of the following regarding sympathetic ophthalmia is true, except
a. The incidence following penetrating trauma is approximately 0.1%.
b. The incidence following elective intraocular surgery is approximately 0.01%.
c. An exciting eye with better visual potential than the sympathizing eye should not be removed.
d. Initial treatment usually includes systemic cytotoxic agents.
124. What area of the eye has the highest blood flow ?
a. retina.
b. choroid.
c. cornea.
d. iris.
125. What percentage of patients with primary CNS lymphoma (PCNSL) have ocular involvement?
a. 5%.
b. 10%.
c. 25%.
d. 50%.
126. What is the histology of most primary CNS lymphoma?
a. Hodgkin T-lymphocyte lymphoma.
b. Hodgkin B-lymphocyte lymphoma.
c. non-Hodgkin B-lymphocyte lymphoma.
d. non-Hodgkin T-lymphocyte lymphoma.
127. Which of the following is true regarding primary CNS lymphoma?
a. Steroids may initially reduce ocular inflammation.
b. All cases are derived from B lymphocytes.
c. Vitreous biopsy is compulsory for diagnosis.
d. Surgery is the main treatment option.
128. In men, choroidal metastases most commonly derive from a primary _______ tumor.
a. lung.
b. testicular.
c. colon.
d. prostate.
129. In women, choroidal metastases most commonly derive from a primary _______ tumor.
a. lung.
b. breast.
c. colon.
d. cervical.
130. Retinal metastases are most commonly from a primary _______ .
a. breast tumor.
b. lung tumor.
c. gastrointestinal tumor.
d. cutaneous melanoma.
 Answers
Answers1. c. Innate immunity is preprogrammed by evolution to respond to offending agents. It has preprogrammed responses due to having preexisting receptors for particular stimuli. Adaptive immunity, on the other hand, is based on a specific environmental stimulus.
2. c. Natural killer (NK) cells are a distinct class of lymphocytes that have the ability to lyse a wide variety of cell types. It is felt that they represent the front-line defense against infections and neoplasia. NK cells may be involved in ocular protection against CMV retinitis or herpes simplex ocular infections.
3. a. “Memory” is exclusive to the adaptive system. On repeated exposure of an offending stimulus, the immune response is more aggressive. This is not true of innate immunity. This is based on memory B and T lymphocytes. The other choices are used by both innate and adaptive immunity.
4. b. The lymphocytes, both B and T, are used only by the adaptive immunity system. Macrophages, monocytes, neutrophils, eosinophils are common to both innate and adaptive immunity as nonspe-cific effector cells.
5. d. Macrophages can initiate the immune cascade by phagocytosing antigen and presenting it to T cells. Macrophages are also known as antigen-presenting cells.
6. c. IgM peaks earlier and disappears earlier than IgG during the primary immune response.
7. d. IgG is the major antibody formed following exposure to an antigen that has previously been encountered.
8. a. Class I MHC molecules, HLA-A, -B, -C, are used in CD8 regulatory T lymphocytes. They are present on almost all nucleated cells. Class II MHC, HLA-DR, HLA-DP, HLA-DQ , are used in CD4 helper T lymphocytes. Class II dependent APCs are best at dealing with endocytosed antigens from the environment.
9. c. IgA is the most abundant antibody in the tear film. IgA is present in mucosal secretions of the body.
10. a. The HLA complex governs immune response and surveillance.
11. c. Mucosa associated lymphoid tissue, or MALT, is the most important immune regulatory component of the conjunctiva. Similar types of lym-phoid tissue are found in the gut, genitourinary tract, and respiratory tract.
12. c. B7 is associated with POHS.
13. d. DR 4 is associated with S.O. and VKH. Other HLA associations are listed below. A29—Birdshot chorioretinitis B7 and DR2—POHS and MS B8—Sarcoidosis, intermediate uveitis B27—Idiopathic iritis, psoriatic arthritis, inflam-matory bowel disease, ankylosing spondylitis, Reiter’s syndrome B44—Retinal vasculitis B51—Behçet’s disease (in Asians only) DR4—JRA, VKH, sympathetic ophthalmia.
14. d. IgM is made of five units, each unit the size of one IgG.
15. d. IgG has the longest half-life, 21 to 23 days. IgA is second at about 6 days, followed by IgM (5 days), IgD (3 days), and IgE (2 days).
16. d. IgG transfer occurs both passively and by active transport to the placenta. (Minimal amounts of IgA also may cross by passive diffusion.)
17. a. Anterior uveitis is the most common type of uveitis.
18. a. Type I hypersensitivity reactions are anaphylactoid.
19. b. Type III. The types of hypersensitivity are listed below:
Type I: Anaphylactoid
Type II: Cytotoxic antibodies
Type III: Immune complex
Type IV: Cell-mediated
Type V: Stimulatory
20. c. IgM or IgM-like immunoglobulins tend to be the only type present in organisms with the most “rudimentary” immune systems.
21. b. Mast cells and IgE promote allergic reactions.
22. a. Cyclophosphamide and chlorambucil are alkylating agents. Methotrexate, azathioprine, and mycophenolate mofetil are antimetabolites.
23. b. C3 is present in serum at a concentration of approximately 1 mg/mL.
24. d. The membrane attack complex, or MAC, consists of C6–C9 complement components.
25. c. Leukotrienes are formed by the lipoxygenase pathway. Cyclooxygenase inhibitors (nonste-roidal agents) block production of all three end products.
26. b. C3b begins the complement pathway.
27. a. This is a classic picture of Candida endogenous endophthalmitis. Lesions begin in the choroid, progress anteriorly through the retina and break through into the vitreous cavity. Intravitreal and systemic therapy may be needed for treatment. Surgery may also be an option. The patient’s history is strongly suggestive of Candida. The patient also needs an infectious disease/endocarditis work up.
28. c. The Arthus reaction (type III) results from formation of antigen–antibody complexes in tissue.
29. b. Immune recovery uveitis occurs in patients infected with HIV/AIDS and CMV. As the immune system improves, patients can suffer from anterior/intermediate uveitis and also develop CME. Epiretinal membranes may also be seen in this condition. It occurs only in eyes infected with CMV. In one study, IRU was associated with previous CMV retinal surface area infection of 25%. Intravitreal injections of steroids are avoided in this condition.
30. d. Graves’ disease and myasthenia gravis are excellent examples of type V hypersensitivity. In these conditions, antibodies react with specific cell surface receptors and either stimulate or depress cellular function.
31. b. All major immunoglobulins classes except IgD have been detected in human tears. IgA (secretory immunoglobulin) is the primary immunoglobulin in tears.
32. c. Wessely rings, also known as immune rings, are ring infiltrates of the corneal stroma, parallel to the limbus. Some corneal rings are probably formed as antigen from a corneal infiltrate encounters antibody from peripheral corneal blood vessels. The infiltrate generally contains complement factors and PMNs.
33. c. Anklyosing spondylitis presents with acute iritis. The back pain and stiffness is usually worse after inactivity and improves with activity.
34. c. Sacroiliac x-ray films may display sclerosis and narrowing of the joint space. Sacroiliitis may also be present.
35. d. Up to 90% of patients with ankylosing spon-dylitis are positive for HLA-B27. HLA-B27 is also associated with several other diseases, although the chance that an HLA-B27 positive individual will have a seronegative spondyloar-thropathy or eye disease is approximately 25%. Fifty percent of patients with acute iritis may be HLA-B27 positive.
36. d. Aortitis occurs in 5% of cases. Aortic valve insufficiency may also be present.
37. d. Dalen-Fuchs nodules are focal accumulations of epithelioid-like cells between Bruch’s membrane and the retinal pigment epithelium (RPE). They may include depigmented RPE cells. They are classically associated with sympathetic ophthalmia and VKH syndrome. They also may be found in tuberculous choroiditis and sarcoidosis.
38. b. Idiopathic iridocyclitis is the most common cause of anterior uveitis, making up at least 10% of all uveitis cases. HLA-B27 iridocyclitis is the second most common cause, and juvenile rheumatoid arthritis and herpes (simplex or zoster) follow in incidence.
39. c. Toxoplasmosis is the most common cause of posterior uveitis, accounting for up to 7% of total uveitis cases. Other causes of posterior uveitis include retinal vasculitis, necrotizing herpetic retinopathy, and idiopathic causes.
40. c. The differential diagnosis of diffusely distributed keratic precipitates includes Fuchs’ het-erochromic iridocyclitis, and rarely sarcoidosis, syphilis, and toxoplasmosis. The diffuse distribution, along with a gelatinous, stellate appearance, makes the KPs of Fuchs’ iridocyclitis distinctive.
41. a. Postoperative hyphema can be seen due to rupture of delicate vessels that cross the angle. Cataract and glaucoma are frequently present. For unknown reasons, synechiae are unusual in Fuchs’ heterochromic iridocyclitis. Some experts question the “inflammatory” nature of this disorder. Visual prognosis is usually good after cataract extraction. The majority of cases have minimal symptoms and do not require therapy.
42. a. Eales’ disease, birdshot retinochoroidopathy, multiple sclerosis, sarcoidosis have inflammation that is centered on the venules. The other answers listed all primarily have vasculitis that is confined to the arterioles.
43. b. Reiter’s syndrome is another HLA-B27 associated disease. The classic findings include urethri-tis, polyarthritis, and conjunctivitis. Iritis is seen but less commonly. It usually affects young males. It may be triggered by diarrhea or dysentery episodes, and has been associated with Chlamydia, Shigella, Salmonella, Yersina, and Ureaplasma urealyticum. Keratoderma blennorrhagicum and circinate balanitis can also be seen in this syndrome. Other associations include Achilles ten-donitis, nail pitting, oral ulcers, plantar fasciitis.
44. d. Granulomas as well as Koeppe and Busacca nodules may appear as iris nodules in ocular sar-coidosis. Juvenile xanthogranuloma features yellow iris nodules, appearing during childhood and associated with spontaneous hyphema. Juvenile xanthogranuloma most frequently involves the skin. Raised orange lesions are typical. In neuro-fibromatosis, Lisch nodules, actually clusters of nevus cells, are definitive. Cutaneous neurofibro-mas, café-au-lait spots, and Lisch nodules are all important diagnostic criteria. Pseudoxanthoma elasticum is associated with “chicken skin” of the head and neck, but no iris nodules.
45. d. Intermediate uveitis accounts for 15% of all uveitis cases, and is associated with several systemic disorders including sarcoidosis, MS, Lyme disease, TB, and syphilis. Idiopathic intermediate uveitis, or pars planitis, accounts for more than 80% of cases. 80% of pars planitis cases are bilateral. Macular edema, followed by cataract, is the most consistent cause of decreased vision in pars planitis. Cystoid macular edema may complicate anterior or posterior uveitis, but much less frequently.
46. a. The HLA antigens are determined by a series of four gene loci located on chromosome 6. HLA-B27 is present in 1.4% to 8.0% of the general population.
47. b. Ritonavir is a protease inhibitor that can increase CD8+ lymphocyte counts.
48. b. In Fuchs’ uveitis syndrome, or Fuchs’ het-erochromic iridocyclitis, cataract and glaucoma occur commonly. Synechiae are rarely seen. Macular edema, retinal scarring, and retinal vascular inflammation have been reported in this condition.
49. c. Up to 25% of individuals with HLA-B27 develop sacroiliac disease. Symptoms of sacro-iliac disease may be subtle. Personal or family history of back problems in patients with iritis should prompt the physician to obtain sacroiliac radiographs.
50. d. Asymptomatic sacroiliac disease can be seen in patients with HLA-B27 spondylitis, particularly in young men. Because irreversible damage may occur before the onset of significant symptoms and simple physical therapy is effective in limiting disability, physical therapy, consisting of back flexibility and stretching exercises, is recommended in young men who are found to be HLA-B27 positive.
51. d. The most common eye finding in Reiter’s syndrome is a nonspecific conjunctivitis. Nongranulomatous iritis, which can be bilateral and chronic, is less common. Keratoderma blen-norrhagicum and circinate balanitis are also diagnostic criteria for the disease.
52. c. Although it is associated with both forms of inflammatory bowel disease, iritis occurs more commonly in patients with ulcerative colitis. Less than 15% of patients with ulcerative colitis and <5% of patients with Crohn’s disease develop acute anterior uveitis. Acute anterior uveitis is associated with psoriatic arthritis, but usually not with psoriasis without arthritis. Tubulointerstitial nephritis uveitis (TINU) occurs in women from adolescence to early 30s. Infectious sources must always be kept in mind in a uveitic condition.
53. d. Juvenile rheumatoid arthritis (JRA) is the most common systemic disease with iridocyclitc association in children.
54. b. ANA+, RF- are risk factors for development of chronic iridocyclitis.
55. a. Diabetes is not a risk factor. The other listed answers are risk factors for development of iridocyclitis.
56. b. On external examination, these eyes are usually white. The disease progresses in an insidious nature. This is why there can be hidden damage done to the eye. This disease is divided into systemic (Still’s disease), polyarticular onset, and pauciarticular onset. Band keratopathy can be seen in this disease also. It is present in the picture.
57. c. Behçet’s disease is much more common among Japanese and individuals from eastern Mediterranean countries. Posterior uveitis, which can include retinal vasculitis, retinal hemorrhages, and retinal necrosis, is more common than anterior uveitis in Behçet’s disease. Oral lesions are the most common finding in Behçet’s disease. These are recurrent in nature.
58. c. The hypopyon can shift as the patient tilts their head. Behçet’s disease is generally recurrent disease. Patients suffer relapses frequently. Some of the cardiac issues include endocarditis, coronary arteritis, pericarditis, myocarditis, endo-cardial fibrosis. In addition, pulmonary arteritis can occur as well as GI ulcers. Corticosteroids are used to treat Behçet’s disease. Other immu-nomodulatory medications such as chlorambucil and azathioprine have been shown to preserve vision.
59. d. Scleromalacia perforans is a type of scleritis. The sclera is severely thinned and the underlying uvea is protruding. It is usually associated with connective tissue diseases and workups are warranted by medicine or rheumatology.
60. d. Aspirin is the drug of choice for Kawasaki’s disease. Although the vast majority of patients recover without complication, approximately 3% of children with Kawasaki’s disease develop acute coronary arteritis, which may lead to myocardial infarction and death. Corticosteroids are contra-indicated in Kawasaki’s because of the increased risk of coronary aneurysm formation.
61. a. The above child has pars planitis. It is an idio-pathic condition and the most common cause of intermediate uveitis. Pars planitis has bimodality in its age distribution. It has been associated with HLA-DR15 and HLA-DR51.
62. b. Classically, chronic CME is a major cause of decreased vision in pars planitis. Also in these patients, the following may occur to cause vision loss: retinal detachment, band keratopathy, PSC cataracts, ERM.
63. d. HLA-DR15 is also associated with MS. Patients with MS can present with a pars planitis type clinical picture.
64. c. Corticosteroids are first line therapy for pars planitis. These can be periocular/topical/sys-temic/intravitreal. Laser or cryo-ablation can be applied if corticosteroid therapy does not control the disease. Vitrectomy and systemic immuno-therapy are other options.
65. d. Ocular manifestations of SLE include all of the choices except for retinitis. Also patients may present with retinal vascular occlusions and subsequent development of neovascularization.
66. b. p-ANCA aids in the diagnosis of polyar-teritis nodosa. c-ANCA is highly diagnostic for Wegner’s granulomatosis.
67. b. The oral lesions seen are aphthous ulcers seen in Behcet’s disease. These can occur on all mucosal surfaces and are painful. Major criteria for diagnosis of Behcet’s disease include recurrent oral aphthous ulcers, skin lesions, ocular inflam-mation, and genital ulcers.
68. a. Birdshot is typically seen in Caucasian women over 40. The ERG can be reduced and the lesions generally do not pigment over time.
69. b. HLA A-29 is present in 7% of the general population. This test is confirmatory in birdshot chorioretinopathy with positivity in >90%.
70. c. The other answers listed can cause vision loss late in the disease.
71. b. Visual field loss can be progressive. Optic nerve edema can be present during the acute phase. Color vision can be decreased, as well as night vision. ICG angiography shows more hypo-fluorescent lesions than on clinical exam or fluo-rescein angiography.
72. a. Posterior and anterior synechiae can be extensive in sarcoidosis. Although the iridocyclitis in sarcoidosis is classically granulomatous, it also can be nongranulomatous.
73. d. An elevated angiotension-converting enzyme (ACE) level occurs in approximately two-thirds of patients with sarcoidosis, and an abnormal chest x-ray (hilar and/or mediastinal adenopathy) is very likely to be found. Elevated serum lysozyme is more sensitive but less specific. Gallium scan also may be helpful in the diagnosis. The anti-neutrophil cytoplasmic antibody (ANCA) assay is useful in diagnosing Wegener granulomatosis, not sarcoidosis.
74. b. Caseation is the hallmark of tuberculosis. Sarcoidosis features noncaseating granulomas.
75. d. Parotid gland infiltration compresses the facial nerve as an innocent bystander (remember that the terminal branches of the facial nerve splits within the substance of the parotid gland). Palsy can be bilateral. The Heerfordt-Waldenström syndrome describes fever, parotid enlargement, anterior uveitis, and facial nerve palsy secondary to sarcoidosis.
76. c. There is a potential association with cerebral vasculitis. In addition, APMPPE has also been associated with other inflammatory and infectious conditions.
77. a. This is the classic finding regarding APMPPE lesions.
78. c. Interstitial keratitis (IK) usually produces intense pain and photophobia. The immune response in interstitial keratitis is felt to be an immune response to treponemal antigens (and not live organisms). Standard regimens for neurosyphilis are sufficient to treat luetic IK. Although results of the RPR and Venereal Disease Research Laboratory (VDRL) tests may be negative in congenital syphilis, those of the FTA-Abs are usually positive.
79. a. Although nontreponemal tests such as the VDRL and rapid plasma reagin (RPR) titers decrease with successful syphilis treatment, the FTA-Abs titer usually does not decrease after treatment. Ocular inflammation (e.g., uveitis, chorioretinitis) secondary to syphilis should be treated as neurosyphilis.
80. c. Lyme immunofluorescent antibody titers and ELISA for IgM and IgG are positive in only 40% to 60% of cases.
81. c. Tuberculosis is an uncommon, but increasingly frequent, cause of uveitis in the United States. Tuberculous bacilli may be found histo-pathologically in eyes with tuberculous uveitis. Tuberculous uveitis may be present even with a normal PPD and normal chest x-ray. For these cases, a second strength (250 tuberculin units) skin test may be positive. Systemic corticoste-roids may cause a dangerous flare-up in otherwise quiescent tuberculosis. Tuberculosis may cause a severe scleritis as well.
82. a. Eighty percent of cases of “peripheral” or intermediate uveitis are bilateral. Vitrectomy may be helpful in clearing media opacities and alleviating vitreous traction, but chronic cystoid macular edema often limits vision. Hypotony due to chronic ciliary body inflammation may also occur.
83. d. PIC is commonly seen in young, myopic, mostly Caucasian women. It is localized to the macular area and has no vitritis. CNVM formation can cause severe vision loss in these patients.
84. b. MEWDS, multiple evanescent white dot syndrome, has classic findings including foveal granularity and white spots that resolve.
85. d. Acute bleb-associated endophthalmitis can occur at any time following filtration surgery. Pneumococcus (S. pneumoniae) and H. influenzae are the most frequent pathogens. This tends to be a very aggressive infection.
86. b. Although prolonged, complicated, invasive surgeries have a higher incidence of postoperative endophthalmitis, even surgeries that do not include ocular penetration, such as pterygium excision and strabismus surgeries may be associated with endophthalmitis.
87. c. Serratia species produce severe acute postoperative endophthalmitis. Certain organisms are clearly implicated in chronic postoperative endo-phthalmitis and are associated with typical time courses:
Staphylococcus epidermidis, within 6 weeks.
Candida species, 1 to 3 months.
Propionibacterium acnes, 2 months to 2 years.
88. c. Posttraumatic endophthalmitis incurs a poor prognosis, with <10% retaining vision better than 20/400.
89. d. Posttraumatic endophthalmitis has a uniquely high percentage of Bacillus species, especially Bacillus cereus, represented etiologically. Estimates have ranged from 20% to 25%, and the organisms seem to be particularly associated with retained metallic foreign bodies, as well as farm or soil-related injuries. Bacillus cereus endophthalmitis can be extremely fulminant. Of slightly greater incidence is Staphylococcusepidermidis (about 30% of posttraumatic endophthalmitis).
90. d. Bacillus cereus may be the single most destructive organism encountered in ocular infections. The organism’s enzymes and exo-toxins can produce unsalvageable destruction within 24 hours. Of interest, Bacillus cereus and Clostridium are two organisms capable of producing systemic, constitutional symptoms from endophthalmitis.
91. b. AZOOR is the diagnosis. The classic curvilinear area is seen that separates normal retina and damaged retina. Patients are usually young myopic females. Vitritis may be present. Patients develop bilateral disease. Most patient’s visual acuity remain in the 20/40 range. Visual field also stabilizes over time.
92. c. The majority of fungal endogenous endo-phthalmitis occurs without evidence of fungemia.
93. b. Sympathetic ophthalmia characteristically spares the choriocapillaris.
94. a. Ocular and CNS findings precede skin changes in this disease. The differential diagnosis for VKH includes sympathetic ophthalmia and posterior scleritis.
95. c. Granulomatous inflammation of the anterior segment can occur in toxoplasmosis. High IOP can also occur. Perivasculitis near active retinal lesions is common (Kyrieleis arteriolitis). The classic lesion of toxoplasmosis is exudative focal retinitis. The definitive host for Toxoplasma gon-dii is the cat, where it is found as an intestinal parasite. (The gondi is a small South American rodent, which is an important intermediate host in that region of the world.)
96. d. Clindamycin is clearly associated with pseu-domembranous colitis. Sulfa drugs can cause Stevens-Johnson syndrome, as well as either hemolytic or aplastic anemia. Pyrimethamine can cause aplastic anemia (hence the concurrent use of folinic acid). Steroid therapy can aggravate diabetes.
97. b. The larvae of Onchocerca volvulus form subcutaneous nodules when they develop into mature worms. This is one manifestation of onchodermatitis.
98. d. The nodules pictured are classic for ocular sarcoid. Sarcoidosis can involve all areas of the eye. The orbit, cranial nerves, and glands can also be affected by sarcoid. These nodules may be easily biopsied for tissue diagnosis.
99. c. This is a classic picture of CMV retinitis. The white areas are active with viral infections. This is a serious disease and potentially may cause blindness from necrosis of the retina and retinal detachment. Patients are treated with a combination of antiviral medications such as ganciclovir and foscarnet, systemically and intravitreally.
100. c. Ocular infection by CMV may cause exudative or rhegmatogenous retinal detachments, with holes in the area of retinal necrosis.
101. b. IV gangciclovir, IV foscarnet, IV cidofovir, oral valganciclovir, and intravitreal ganciclovir/ foscarnet are treatment options. IV acyclovir is generally not used in CMV retinitis.
102. d. Iatrogenic immunosuppression, intravenous drug abuse, and indwelling intravenous catheters for hyperalimentation are risk factors for candidal infections. Candida endophthalmitis is less common in AIDS (mucocutaneous candi-diasis is common).
103. d. Patients with necrotizing herpetic retini-tis/acute retinal necrosis (ARN) are usually otherwise healthy and not debilitated, as opposed to the typical patient with viral (CMV) retinitis. (Severe, bilateral ARN has been described in patients with AIDS.)
104. b. Ocular histoplasmosis syndrome has NO vitreous cells. The other conditions are masquerade syndromes that may produce a chronic vitreous cellular reaction. Primary CNS lym-phoma is also on this differential and critically important to consider.
105. b. Systemic infection with Nocardia is characterized by pneumonia and disseminated abscesses. Nocardia is a filamentary bacterium. Ocular involvement results from hematogenous spread and is rare. It may cause a range of ocular inflammation from a focal mass to disseminated inflammation.
106. d. Toxocara canis is an intestinal parasite of dogs and cats. Dogs are more commonly implicated in human infections. After ingestion of ova, larvae are spawned that will penetrate the intestinal wall and take up residence in the liver and lungs. From there, larvae can disseminate to any organ, including the eye. Eye involvement is usually unilateral. Dragging of the retina may occur.
107. d. Peripheral histo spots begin to appear around adolescence. The maculopathy usually does not appear until the 20s. The early stage of the disease is thought to be a choroiditis. Vitreous cells are not seen in POHS. Visual complaints are caused by the maculopathy and development of CNVM.
108. c. The presentation shown is that of APMPPE. This disorder is seen in healthy young adults after a flu-like illness. It is seen equal in males and females. Scotomas are acute in presentation. In the fundus, there are several large, flat lesions at the level of the RPE. On angiography, these lesions classically show early hypofluorescence and late hyperfluorescent staining. The majority of these patients return to good visual acuity within 6 months. The condition is self-limited. Rarely, it may be associated with cerebral vasculitis.
109. d. Berlin’s nodules are located in the angle. Koeppe nodules are present on the pupillary border, and Busacca nodules are located in the mid-iris. Iris atrophy and anterior and posteror synechaie may also occur in uveitis.
110. b. Periocular steroid injection should not be used in cases of infectious uveitis. They can also lead to further melting and perforation in necro-tizing scleritis. Longer-acting steroids (e.g., tri-amcinolone) given via periocular injection have the potential for raising IOP for an extended period of time.
111. b. The worms typically affect unilaterally, (hence the name). Laser photocoagulation of the subretinal worm is highly effective. Systemic therapy with thiabendazole and albendazole has also been implemented in some cases. Reinfection is possible with this disease with a second worm.
112. c. This is an example of band keratopathy. It can be seen in eyes with history of previous surgery (including vitrectomy and use of silicone oil), ocular tumors, phthisis, and chronic inflam-matory conditions. It is related to the deposition of calcium in the cornea.
113. d. HIV retinopathy is the most common ocular manifestation of patients with AIDS. It is characterized by microaneurysms, cotton-wool spots, and retinal hemorrhages. Fifty to seventy percent of patients with AIDS develop some ocular abnormality. One series reported that up to 92% of patients with AIDS would develop cotton-wool spots.
114. d. CMV retinitis, along with Pneumocystis cari-nii pneumonia and Kaposi’s sarcoma, was one of the infections recognized early in the course of the epidemic as a defining feature of the disease.
115. b. Pneumocystis choroiditis is seen particularly in patients receiving aerosolized pentamidine. Histopathologically, the lesions in the choroid contain cysts or trophozoites of Pneumocystis carinii. IV TMP–SMX therapy is the treatment of choice for PCP choroiditis. APMPPE can resemble this clinical disease.
116. c. Kaposi’s sarcoma may be noted on the eyelid skin or conjunctiva. Skin lesions usually appear as nontender, elevated, purple nodules. Conjunctival involvement is manifested by red subconjunctival masses.
117. b. Herpetic uveitis, HSV and HZV, may cause stromal atrophy of the iris. This is a clue to diagnosis. The other conditions tend not to cause atrophy. Transillumation allows for best visualization of iris stromal atrophy.
118. c. The picture in question 118 is classic punctate inner choroidopathy The patient is in the classic demographic as she is a young, myopic woman.
119. c. Chorioretinits from documented candidemia can occur in 9% to 10% of patients.
120. a. Most patients develop an intermediate uveitis (pars planitis) or panuveitis. Macular edema is less common. HLA-DR15 is associated with MS and uveitis. The uveitis is usually less aggressive than the idiopathic form.
121. d. Both PORN and ARN are manifestations of severe posterior segment infection by the herpes family of viruses. ARN, particularly in immunocompetent hosts, responds to intravenous acyclovir more reliably than PORN. Up to two-thirds of PORN eyes will end up with no light perception (NLP), despite treatment. The vision outcomes in PORN are poor.
122. d. Laser photocoagulation may have the same salutary effect on resistant pars planitis as cryo-therapy, but without the risk of RD.
123. d. Systemic corticosteroids are generally used initially, followed by cyclosporine or cytotoxic drugs as second-line options.
124. b. The choroid has the highest amount of blood flow in the entire body.
125. c. Up to 25% of patients with PCNSL will have ocular involvement.
126. c. Ninety-eight percent are non-Hodgkin B-lymphocyte lymphomas. Two percent are T-lymphocyte lymphomas.
127. a. Steroids may initially improve the inflamma-tion but will eventually fail as a therapy. Most cases are B cell derived. Vitreous biopsy/retinal biopsy/CSF histology may lead to a diagnosis. Vitreous biopsy is not the only way for tissue diagnosis. The current therapy is combination chemotherapy and radiotherapy. Surgery alone is associated with a poor prognosis.
128. a. Choroidal metastases are most commonly from a primary lung tumor in men.
129. b. Choroidal metastases are most commonly from a primary breast tumor in women.
130. d. Retinal metastases are rare. Cutaneous melanoma is the most common primary tumor.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


