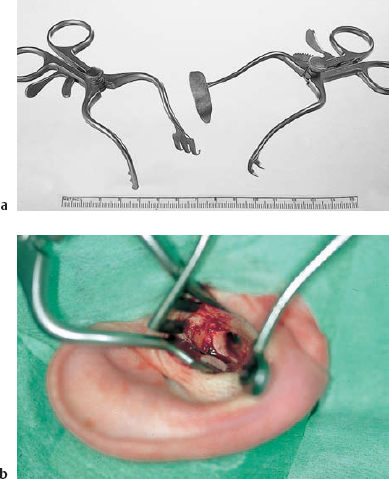
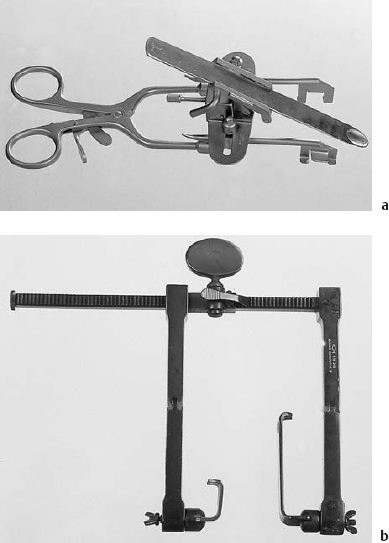
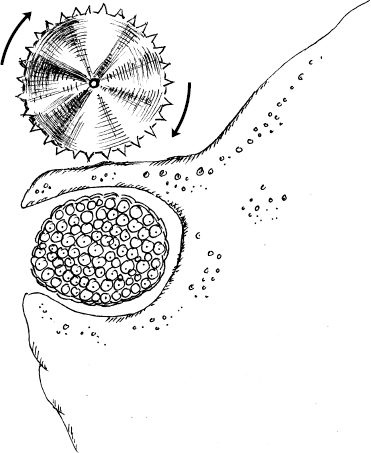
2 Instruments and Setting The smaller a surgical field, the greater the expenditure required for suitable equipment. This paradox also applies to microsurgery of the ear. Due to the vulnerability of the ear’s superfine structures, any improvised use of inadequate instruments is liable to cause injury to important tissues. A complete range of microtools therefore has to be readily available, and the instruments also require special care and skill. Centralized sterilization, for instance, is a daily source of extra costs for repairing and storing multiple sets. Any lack of technically trained personnel for the maintenance of high-technology equipment items such as the microscope, laser, and monitoring apparatus will be paid for dearly with frequently occurring defects. Detailed knowledge of the technical prerequisites is needed before an ear and skull base surgery service can be organized. On the other hand, highly skilled surgeons are often known to use a comparatively small selection of specialized instruments to which they have become accustomed. The following sections describe the author’s own personal instrumentarium, and make no claim to represent a standardized range of equipment. Many operations in the area of the external ear can be performed with the naked eye. As soon as the external auditory meatus and middle ear are entered, however, an operating microscope with optical magnification from six-fold to 40-fold is required. In Europe, the Contraves, Wild, and Zeiss companies, among others, are known for their wide ranges of models for use in various disciplines. As a student of H.L Wullstein, who together with Littmann designed the first classic Zeiss operating microscope for ear surgery (Littmann 1954), I have become accustomed to using Zeiss products. At present, I use a ceiling-mounted model, the OpMi 111, with Supralux 300 xenon light illumination (Fig. 2.1). This provides optimal brightness and brilliance. It should be mentioned that in full power mode, this instrument warms up the surgical field within the area of focus. When working on nerves or the inner ear, one should avoid prolonged exposition without cooling the structure with saline, or one should select an intensity below the maximum. For office follow-up examinations, I use a compact model, the OpMi 6. Additional intraoperative use of endoscopes has attracted interest in recent years (Thomassin 1994, Magnan and Sanna 1999). In particular, thin endoscopes with an angled view (30°, 70°) have proved valuable for exploring niches “around corners.” I have often used a 4-mm rigid endoscope (Wolf, Ltd.) with an angle of 70°—more for inspecting the internal auditory meatus than for studying mesotympanic or epitympanic recesses behind the bony bridge. To check retraction pockets, however, a fine 30° angled otoendoscope is indispensable. A 0° endoscope is also valuable for all kinds of endophotography of the ear in the office. Fig. 2.1 Rack-mounted operating microscope (Zeiss OpMi 111, S5 Superlux 300, f 125) with a Supralux xenon light source. Positioning of the patient for the enlarged middle fossa approach. For exposure of the surgical field within the middle ear and temporal bone, two or three curved retractors of two different sizes each are necessary. I have designed two special retractors for endaural surgery. One opens the external auditory canal (EAC) in the horizontal plane, and has only small spikes on its anterior branch, fitting into the auxiliary skin incision (Fig. 2.2). The second model retracts the entrance of the EAC vertically. Its lower branch has an S-curved blade, which fits snugly into the meatal orifice without injuring the skin. At the same time, its lateral extension depresses the antitragus. Fig. 2.3 Retractors for temporal bone surgery. a The Fisch self-retaining retractor. b The Fisch mandibula retractor for the infratemporal approach. For retraction of the temporal dura during middle cranial fossa approaches, I still prefer the Fisch self-retaining retractor (Fig. 2.3a). It is flexible, and has differently curved exchangeable spatulas, which compensates for the disadvantage that its two branches are rather bulky. Driscoll et al. (1999) have published a useful technical comparison between the House—Urban retractor and the Fisch, Garcia-Ibañez, and UCSF models, together with their compression effects on the temporal lobe. For the lateral infratemporal approach, the Fisch mandibula retractor has proved valuable (Fig. 2.3b). Bone removal is still the focus in microsurgery of the ear. There is no lack of various types of: Fig. 2.4 Correct direction (arrows) for drill rotation at free edges of bone. The diamond drill is an ingenious solution for the problem of shaving a hard substance like bone without injuring the soft tissue lying beneath it. For superfine bone removal at the internal auditory meatus, or around the facial nerve, or for sculpturing autologous bone prostheses, very small sizes of diamond are needed. The formula for the velocity of the bone cutting process is: v = α×π×n where v is velocity, a is the diameter, the constant π is 3.14, and n corresponds to the rotatory frequency per minute (Elies 1996). Not included in this formula are the coefficients for material resistance and for the sharpness of the burr’s profile. The diameter d of the burr’s globe or cylinder shape is directly proportional to the rapidity of bone removal. Various electric or air-driven drilling machines are available, and these are convenient for middle ear surgery. For surgery in the depth of the temporal bone or the skull base, however, there are some problems. Very long and thin angled shafts are required, and reverse rotation must be available. These requirements involve the disadvantages of reduced driving power and rapid heating. Air-driven drills are generally cooler, but their handpieces are comparatively heavy. I have not yet found the ideal microdrill—one that would be robust enough for ample bone resection within the petrous bone, but which would not become hot after prolonged hard bone work. New geometrical arrangements of the cutting blades have been developed to prevent them becoming obstructed with bone dust (Elies 1996). Single-use burrs have not yet become popular.
 Visualization
Visualization

 Severance of Tissue
Severance of Tissue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


