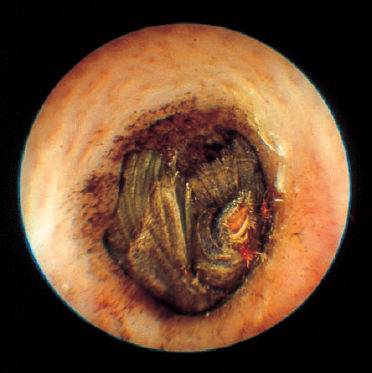
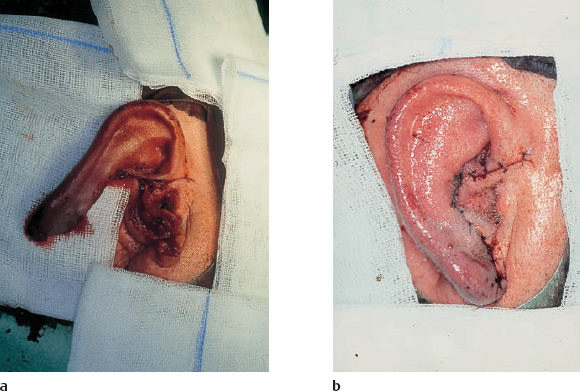
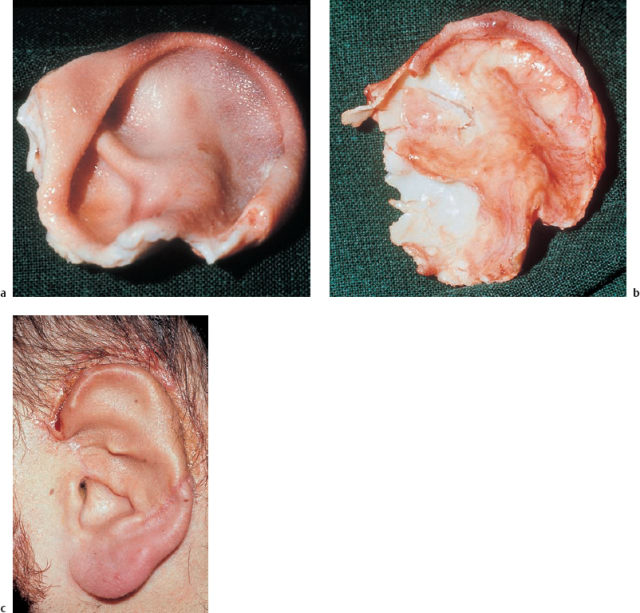
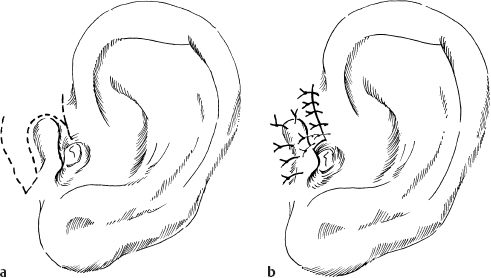
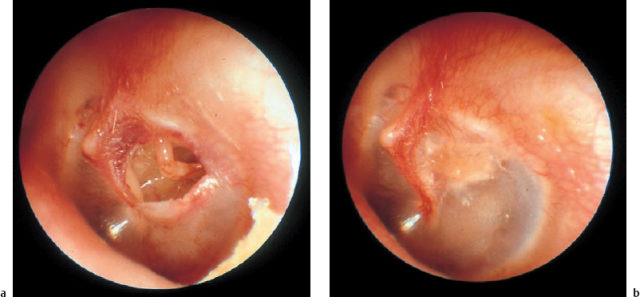
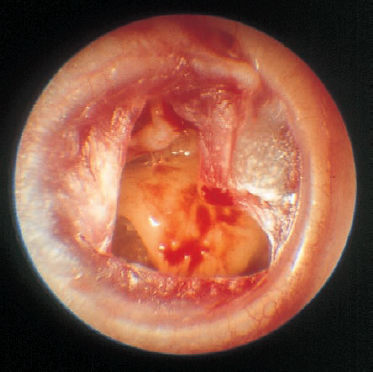
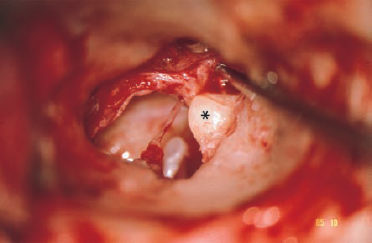
5 Injuries to the Ear and Temporal Bone Injuries to the external ear cause a wide variety of pathological changes. Most of these can be regarded as emergency conditions that require immediate surgical treatment to prevent acute or delayed complications. There are two criteria for a need to intervene due to the potential sequelae: functional impairment and aesthetic deformity. The aim in all types of functional and aesthetic rehabilitation is to achieve the best possible restoration of the previous morphology. Foreign-body penetration of the external auditory canal mainly occurs in childhood, with loose material such as paper or matchsticks, and parts of toys such as plastic wheels or marbles, being pressed into the ear. However, insects are also able to enter the meatus and can become trapped on the drum membrane (Fig. 5.1). The symptoms that follow include itching or pain, or at a later stage infectious dermatitis with discharge from the ear. When the ear is examined, the diagnosis is easy. Removing foreign bodies is usually unproblematic. Even children are able to tolerate gentle extraction. Aspiration or mobilization with a 90° hook is more practical than using pincers, which can easily push a globe deeper into the canal. The use of local anesthesia, or a short period of general anesthesia, is exceptional and restricted to the removal of bulky objects in infants. The use of irrigation is questionable, as the foreign body may be concealing a perforation, or may have induced ulceration. It is often necessary to clean hard ear wax out of an ear canal during the removal procedure, and this can be achieved by chemical dissolution with docusate sodium (Otowaxol) and subsequent aspiration. Hematoma in the pinna (Fig. 5.2), caused by blunt trauma exerting shearing forces on the skin, is an emergency condition that requires immediate evacuation and subsequent compression. Aspirating the blood with a 2-gauge needle may be adequate during the first few hours, but it may soon become necessary to carry out a short skin incision along the helix to remove blood clots. We also apply cold wet compresses soaked in a disinfectant such as ethacridine lactate (Rivanol). Perichondritis can be expected to develop in all cases of untreated ear hematoma, with a risk of cartilage necrosis and severe ear deformity (Fig. 5.3). One should not hesitate to open the hematoma or abscess via a generous skin incision along the helix fold, or with a postauricular incision and resection of some cartilage—cleaning necrotic cartilage and pus out of the wound cavity. Wound drainage is indicated, with H2O2 irrigation, over the following days. Broad-spectrum antibiotic treatment is also necessary. Use of a thorough mattress suture is recommended for prophylaxis against recurrent hematoma. This encourages the development of fibrous scarring through the fenestrated cartilage from skin to skin. Dog bites and stab wounds involve the same risk of perichondritis, and require very close attention. Immediate broad-spectrum antibiotic treatment is required, as well as a refresher vaccination against tetanus. As soon as circumscribed swelling or fluctuation appears (Fig. 5.4), adequate circumcision and drainage is necessary. Delayed treatment, when there is incipient necrosis of the cartilage, includes creating a broad opening, with generous resection of the infected cartilage. It has proved valuable to insert a stabilizing stent (autogenous cartilage, collagen foil). The complication rates for necrosis, recurrent abscess, and extrusion have unexpectedly been very low. Fig. 5.1 Foreign bodies deep inside a right external auditory canal: a moth and aphids. Fig. 5.3 Auricular deformation after inadequate treatment of an auricular hematoma. Fig. 5.4 Perichondritis after a dog bite. a Early inflammatory reaction. Laceration and avulsion of the pinna require difficult and urgent surgery. Reconstructing the pinna’s original shape for aesthetic purposes is the basic task. As in facial plastic surgery, one should try to preserve as much of the cartilage and skin as possible. Contaminated wounds should be scrubbed rather than excised. Resynthesis of fragments depends on the local circulation. If the covering periosteum is still bleeding, the fragments can be sewn together with 4–0 Vicryl sutures (Fig. 5.5). If it is ischemic, but there is sufficient vascularized skin for complete coverage, one can also try to reconstruct the auricle, possibly with the additional insertion of a stent to prevent shrinking. Smaller substantial defects can be reconstituted using local transposition or rotation flaps (Fig. 5.6). When there is complete or near-complete avulsion, end-to-end resuturing of the fragment is hopeless. In these cases, skeletonizing of the pinna (Fig. 5.7) and use of a local or distant (supraclavicular, groin) subcutaneous implant is recommended. At a second-stage or third-stage operation, the revitalized autogenous cartilage can serve as a profile frame for a new pinna, covered by the local or transplanted skin. It has been reported that vascular microanastomosis is successful, but this of course assumes that vessels adequate for anastomosis can be identified. Fig. 5.6 Skin incision for reconstruction of the auricle. The circumcised local flap is folded upward, and the resulting subauricular defect is closed with sutures. Minor stab wounds, which are quite frequent and may be self-inflicted or iatrogenic, usually do not require specific treatment other than conservative local cleaning and disinfection. However, larger wounds caused by tree branches, ski poles, etc., need to be inspected microscopically and diagnosed for possible injury to the tympanic cavity, floor of the middle cranial fossa, and mandibular joint. Sagittal computed tomography (CT) is a convenient method of obtaining a precise investigation. Larger defects in the meatal skin are covered by split skin, to prevent subsequent stenosis by scars. An endaural Botey incision helps expose the meatal walls. Bone fragments are removed, and a damaged mandibular joint is revised according to the type of injury. A small injury to the dura at the meatal roof can be inspected and closed via the endaural approach (Fig. 5.8). A larger penetrating endocranial wound is best explored and closed using an extradural, transtemporal approach (see chapter 13). This allows wide inspection of the temporal bone and temporal lobe. The brain can be cleaned locally, and the dural defect is closed with a fascial patch or an allogenic patch (e.g., Tutoplast). Fig. 5.8 Injury to the meatal roof, with a small dural fistula. Exploration and closure were carried out using the endaural approach (left ear). TM Tympanic membrane Partial or circular stenoses of the external auditory canal (EAC) can lead to external otitis and the development of meatal cholesteatoma. Patients may present with chronic discharge, hearing loss, or troublesome itching. The management consists of scar removal and implantation of a new cutaneous lining on the remodeled EAC walls. I prefer the usual Botey endaural skin incision, as in endaural tympanomeatoplasty. Special care needs to be taken to preserve as much of the original skin as possible. After excision of bridging scar formations, the resulting open bone areas are covered with postauricular split skin, or preferably with thinned full-thickness skin. Fig. 5.10 Posttraumatic stenosis of a left external auditory canal (EAC). a Preoperative appearance. b The widened orifice of the EAC after the Z-plasty. If there is a shortage of skin—e.g., in pinna defects—a superiorly pedicled skin flap from the cheek, rotated posteriorly, provides excellent material, and the formation of this type of flap using a Z-plasty at the same time pulls the meatal entrance anterosuperiorly, widening it by about 30% (Figs. 5.9, 5.10). Injuries to the middle ear are basically caused by mechanical trauma via the EAC, or by petrous bone fractures. The most frequent forms are barotrauma and piercing injury, but iatrogenic injuries occurring during office procedures or during surgery are also encountered. Particularly when there are anatomical abnormalities (atretic complex, displacement of the internal carotid artery, stapedial artery, sigmoid sinus, or facial nerve), severe impairment can be caused during normal manipulations such as paracentesis, cleaning of the EAC, or closure of a visible perforation. Middle ear trauma can involve: Fig. 5.12 Recent traumatic subtotal perforation of the drumhead, requiring treatment with myringoplasty. The margins of the defect have been epithelialized with inward-folded remnants (right ear). Fig. 5.13 Luxation of the incus with middle ear trauma. The stapes is visible below a thin chorda tympani. Extraction, reconstruction, and reinterposition of the dislocated incus (*) are indicated (left ear). Traumatic perforations of the drum membrane have a strong tendency to close spontaneously (Fig. 5.11). The resulting scar can become atrophic or hypertrophic, with chalky incrustation. As soon as the outer squamous epithelium has folded inward, however, a perforation will stay open, and a secondary cholesteatoma may occur (Fig. 5.12). Disruption of the ossicular chain can happen with or without a drum perforation. It is induced by barotrauma, direct external piercing forces, and more frequently by temporal bone fractures (Fig. 5.13
 External Ear Trauma
External Ear Trauma
Foreign Bodies
Injury to the Auricle



b After resection of necrotic cartilage and interposition of homologous cartilage.

Injury to the External Auditory Canal

Posttraumatic Stenosis of the External Auditory Canal
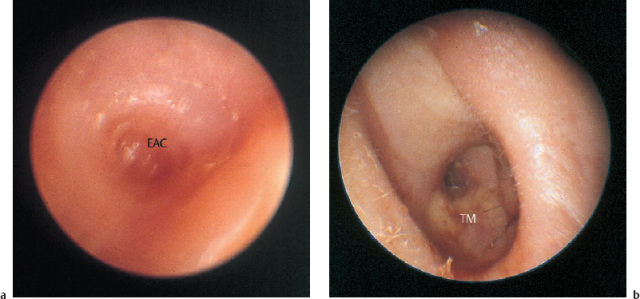
TM Tympanic membrane
 Middle Ear Trauma
Middle Ear Trauma
Clinical Entities
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


