Inflammatory Glaucoma
Reid A. Longmuir
John H. Fingert
Wallace L. M. Alward
Intraocular inflammation affects both aqueous inflow and outflow. A decrease in aqueous production frequently leads to a reduction in intraocular pressure. Elevated intraocular pressure can occur if aqueous outflow is decreased to a greater extent than aqueous production.1 In many eyes with uveitis, the intraocular pressure is normal or low acutely, but may become elevated later when aqueous production returns to normal and outflow remains compromised.2 Inflamed eyes should be monitored closely to detect a late rise in intraocular pressure.
In large reviews of uveitis patients, the reported prevalence of secondary glaucoma ranges from 9.6% to 23%.3,4,5 Although all types of ocular inflammation can lead to glaucoma, it is seen most frequently with iridocyclitis. In a study of 1,254 consecutive patients at a uveitis clinic, glaucoma was seen most frequently with anterior, chronic, and granulomatous disease.3 Of those with glaucoma, 67% had anterior segment inflammation, 4% had intermediate uveitis, and 13% had posterior uveitis. The remaining patients had panuveitis.3 In this study, the types of uveitis that were most likely to result in glaucoma were secondary to herpes simplex and herpes zoster (22% developed glaucoma), Fuchs heterochromic iridocyclitis, Vogt-Koyanagi-Harada syndrome, juvenile rheumatoid arthritis, syphilis, and sarcoidosis.3 Table 54D.1 outlines the many types of uveitis reported to be associated with secondary glaucoma.
TABLE 54D.1: INFLAMMATORY DISORDERS ASSOCIATED WITH GLAUCOMA | |
|---|---|
|
Mechanisms of Intraocular Pressure Rise
Open-Angle Mechanisms
Aqueous outflow is decreased when the trabecular meshwork becomes clogged with macrophages and inflammatory debris.30,31 The iridocorneal angle may also be infiltrated with lymphocytes, polymorphonuclear leukocytes, and fibrin,32 and the trabecular beams may become swollen.32 Aqueous protein alone has been shown to significantly reduce outflow.33 In acute inflammation, angle obstruction is usually temporary. In chronic or recurrent disease, however, inflammation can permanently damage the trabecular meshwork. A basement-membranelike material may develop over the angle.34 Trabecular endothelial cells that phagocytize debris may migrate away from the collagen beams or undergo autolysis, resulting in permanent impairment of function.2,35,36
Increased outflow resistance distal to the Schlemm’s canal is proposed as a mechanism for ocular hypertension in scleritis. Histopathologic study has demonstrated lymphocytic cuffing of the scleral outflow channels in scleritis patients with glaucoma.37
Although most ocular hypertension due to inflammation is a result of decreased outflow, increased aqueous production due to prostaglandins may also play a role.38 Prostaglandins have been demonstrated in the anterior chamber of uveitis patients,39 and have been implicated in the pathogenesis of glaucomatocyclitic crisis.40
Finally, chronic treatment of inflammation with corticosteroids may elevate intraocular pressure. This is discussed in detail later in the chapter.
Closed-Angle Mechanisms
Disruption of the blood–aqueous barrier allows inflammatory cells, fibrin, and debris to collect in the anterior chamber angle. The peripheral iris can then become adherent to the trabecular meshwork, resulting in the formation of peripheral anterior synechiae (Figs. 54D.1 and 54D.2).2 The areas of open angle between synechiae are often heavily pigmented and function poorly.2 Chronic inflammation may be associated with angle neovascularization, which can also cause synechiae to develop.2
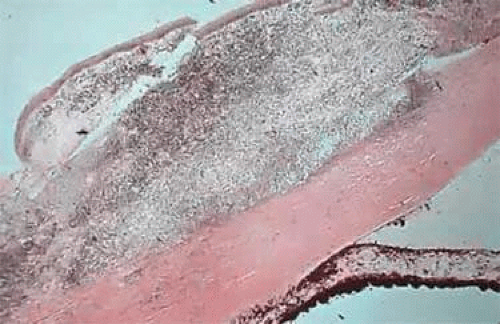 Figure 54D.1. Histopathologic slide of the iridocorneal angle of a patient with congenital syphilis. Granulomatous inflammation is present on the surface of this eye, and the angle is closed by peripheral anterior synechieae. (Courtesy of Robert Folberg, MD. Copyright University of Iowa. Alward WLM: Color Atlas of Gonioscopy. London: Mosby–Year Book, 1994.) |
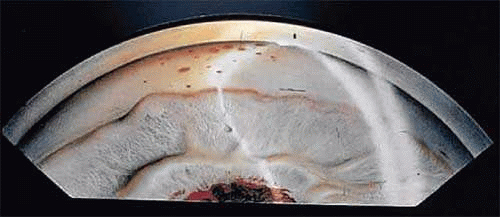 Figure 54D.2. Gonioscopic view of the iridocorneal angle in a child with uveitis. The trabecular meshwork can be seen only at the left of this illustration. The remainder of the angle has been closed by peripheral anterior synechiae. Central posterior synechiae are present at the pupil, and keratic precipitates are visible on the corneal endothelium. (Illustration by Lee Allen. Copyright University of Iowa. Alward WLM: Color Atlas of Gonioscopy. London: Mosby–Year Book, 1994.) |
Anterior segment inflammation may also cause adhesions between the iris and anterior lens capsule to form. In aphakic and pseudophakic patients, the iris may adhere to the vitreous face or intraocular lens, respectively. Seclusion of the pupil occurs when these central posterior synechiae block flow of aqueous from the posterior to the anterior chamber through the pupil. Increased pressure in the posterior chamber pushes the peripheral iris forward (iris bombé, Fig. 54D.3) against the trabecular meshwork, leading to appositional angle closure. In an inflamed eye, this can quickly lead to synechial angle closure.2
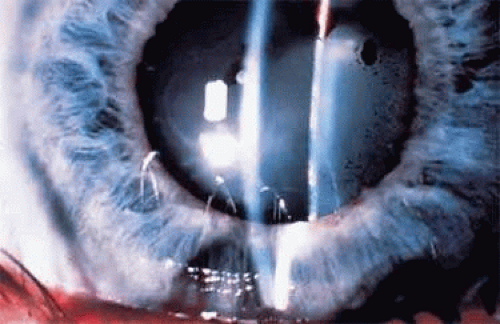 Figure 54D.3. Central posterior synechiae leading to pupillary block and iris bombé. (Courtesy Paul F. Palmberg, MD, PhD, Bascom Palmer Eye Institute, University of Miami. Alward WLM: Color Atlas of Gonioscopy. London: Mosby–Year Book, 1994.) |
Ciliary body edema may cause anterolateral rotation of the ciliary body about its attachment to the scleral spur. This relaxes the lens zonules, resulting in forward movement of a rounder lens. The anterior face of the ciliary body and peripheral iris are then brought into contact with the trabecular meshwork, causing angle closure.41,42 This mechanism of angle closure is treated with cycloplegics and steroids.41,42 Cholinergic agonists should be avoided.
Anterior Uveitis
Glaucoma is most commonly associated with anterior uveitis. Pain, photophobia, and blurred vision are characteristic symptoms of acute iridocyclitis. Chronic inflammation may be asymptomatic, and extensive glaucomatous damage can occur prior to diagnosis. On examination, conjunctival injection with perilimbal ciliary flush is present. Cell and flare are present in the anterior chamber. Keratic precipitates are present on the corneal endothelium, and if the intraocular pressure is elevated, microcystic epithelial edema may be seen. Gonioscopy may reveal increased pigmentation, inflammatory precipitates, or peripheral anterior synechiae. The iris may exhibit inflammatory nodules. Central posterior synechiae may develop, and if confluent may result in seclusion of the pupil, iris bombé, and angle closure. In the majority of patients with anterior uveitis, an underlying etiology is never determined.
Joint Disease and HLA-B27
Arthritis is often associated with ocular inflammation. In a review of 1,927 patients with uveitis, an underlying joint disease was found in 10%.43 Anterior uveitis and joint disease are also frequently associated with the genetic marker HLA-B27.44,45 HLA-B27–positive anterior uveitis is usually recurrent, unilateral, and nongranulomatous. Extensive anterior chamber cellular reaction and fibrin formation are characteristic.44,46 Of patients with acute nongranulomatous iridocyclitis, 52% to 56% are HLA-B27 positive, compared with 4% to 8% of controls without uveitis.44,47 About half (45% to 58%) of patients with HLA-B27–positive anterior uveitis have a systemic disorder associated with joint disease, such as ankylosing spondylitis, reactive arthritis (formerly known as Reiter syndrome), psoriatic arthritis, or inflammatory bowel disease.44,46,48 In one review, half of the patients with a systemic disease were diagnosed after ophthalmic consultation.48
The cause of HLA-B27–associated uveitis remains unclear; however, bacterial organisms have been investigated for a possible role in the pathogenesis of this condition. Elevated titers of antibodies to gram-negative organisms such as Yersinia enterocolitica and Helicobacter pylori have been detected in patients with HLA-B27–associated arthritis and uveitis.49,50,51,52,53 The results of these serological studies and the observed homology between gram-negative bacterial antigens and HLA-B27 molecules has suggested that an immune response to these pathogens may contribute to uveitis via molecular mimicry.54
Associated ocular hypertension is reported in 8% to 23% of patients with HLA-B27–positive anterior uveitis48,55 and 4% to 8% develop secondary glaucoma.46,48 In one study of patients with ankylosing spondylitis, 28% developed uveitis, and in some the ocular disease presented prior to joint symptoms.56 In another report of 47 patients with ankylosing spondylitis and uveitis, 4% developed ocular hypertension and 2% had secondary glaucoma.3 In a study of 113 patients with reactive arthritis, 12% had iritis and 1% had glaucoma.57 Of 26 patients with reactive arthritis and uveitis in another review, 12% developed glaucoma.3
Juvenile Rheumatoid Arthritis
Juvenile rheumatoid arthritis is defined as arthritis of at least six weeks’ duration in a child younger than age 16.58,59 It is the most common cause of anterior uveitis in childhood,4 and can be complicated by secondary glaucoma in 15% to 26% of patients4,8,60,61,62,63. The chronic, nongranulomatous uveitis is more common in pauciarticular disease and in girls who are both antinuclear antibody (ANA) positive and rheumatoid factor negative.8,63
The inflammation is often asymptomatic and usually bilateral.60 It can precede joint symptoms or persist long after the arthritis is quiet.60,64 The activity of the joint inflammation is independent of the ocular disease.64 When uveitis is the initial manifestation, the visual prognosis is poorer than if the arthritis is the presenting sign.8 In one study, presentation with advanced inflammation (posterior synechiae) was associated with glaucoma in 45% compared with 17% of patients with mild or no inflammation at onset.8
Glaucoma secondary to juvenile rheumatoid arthritis can be challenging to treat. In one report, filtering surgery was required in 19% of cases.63 Other studies indicate that filtering surgery provided adequate control in only 18% to 38% of cases.4,60 Cyclocryotherapy may be effective in lowering pressure, but one report suggests this result may last only a few months.65 Control of the uveitis is essential, and a stepwise approach to treatment has been advocated, with no tolerance for any active inflammation.66 Anterior chamber cellular response should always be treated, but flare alone becomes chronic and is not an indicator of active disease.66,67 Therapy begins with topical corticosteroids, and progresses to periocular steroid injection, systemic nonsteroidal anti-inflammatory agents, systemic steroids, and immunosuppressants.66 Glaucoma and cataracts can be exacerbated by steroid therapy.8 Oral nonsteroidal agents have been reported to improve chronic iridocyclitis and allow for reduction of steroid dose.68 Methotrexate is also steroid-sparing69 and is effective in resistant cases of the disease.63,70,71 Recent retrospective case-series studies have suggested that biological response modifiers such as infliximab may also be useful in treating refractory cases of juvenile rheumatoid uveitis.72,73,74
Herpes Simplex and Herpes Zoster
Keratouveitis due to herpes virus infections often leads to secondary glaucoma. A large study of patients revealed that uveitis associated with herpes simplex virus (HSV) and herpes zoster carried the greatest risk of development of secondary glaucoma, with 23% of cases developing this complication.3 Pathologic studies of human eyes and a rabbit model system have suggested that the mechanism of increased IOP in herpetic uveitis may be due to inflammatory changes in the trabecular meshwork (trabeculitis) and/or accumulation of inflammatory cells and debris in the outflow pathway.75,76
A review of patients with herpes simplex uveitis revealed that 28% developed ocular hypertension, with 10% of these progressing to visual field loss.9 HSV keratitis associated with elevated intraocular pressure is usually disciform or stromal.9 Management of secondary glaucoma is initially directed at controlling the viral infection and treating the inflammation.47 Topical trifluorothymidine penetrates the cornea better than other antiviral agents and may be best for treatment of HSV keratitis.77 Systemic acyclovir may also be helpful.78 Topical corticosteroids must always be used in conjunction with antiviral coverage to prevent reactivation of epithelial disease.47 Cycloplegics relieve ciliary spasm, and aqueous suppressants are best for treatment of elevated pressure.
In a study of 86 patients with herpes zoster ophthalmicus, 43% had uveitis, and 27% of these had ocular hypertension. Only one patient developed visual field loss.10 In another report of 14 patients, five had elevated intraocular pressure.79 The use of oral acyclovir80 or related antivirals (valacyclovir, famciclovir)81 within 72 hours of onset of skin lesions reduces the incidence and severity of secondary uveitis that can lead to glaucoma. Topical acyclovir has also been shown to be more effective than topical corticosteroids in shortening the course of zoster uveitis.82
Congenital Rubella
Secondary glaucoma may also be associated with congenital rubella. In one study of 125 patients with this disease, 9% developed glaucoma.83 Another review of 328 patients found 15 with secondary glaucoma, and all but one had bilateral disease. All 15 required surgery, and 8 were blind in both eyes by 7 years of age.84 A review of congenital rubella in Oman revealed that of 32 patients, 28 had ocular manifestations, including 4 with glaucoma.85 Glaucoma in rubella is usually infantile in onset and often associated with buphthalmos and persistent corneal haze.84 Late-onset forms have also been reported in older children and young adults who were aphakic and microphthalmic.86 Another form presenting later is characterized by iris stromal hypoplasia in patients without cataract or microphthalmia.87
Syphilis
Interstitial keratitis is usually a late manifestation of congenital syphilis88 due to an immune hypersensitivity reaction to treponemal antigen in the corneal stroma.88 Acutely it produces an opacified, edematous cornea with deep vascularization. It is bilateral in 90% of cases.47 Glaucoma can occur in the acute inflammatory stage, but more commonly develops later. In one study the interval from diagnosis to development of secondary glaucoma ranged from 7 to 50 years, with a mean of 27 years.89 Twenty-five percent of patients with interstitial keratitis in one review developed glaucoma.90 In another report, 24% of patients with syphilitic uveitis had ocular hypertension, and 60% of these went on to develop glaucoma.3
Both open- and closed-angle mechanisms have been described. Open-angle glaucoma may occur with increased pigmentation and a hyalinized appearance to the trabecular meshwork resulting from acute inflammation early in life.34,91 These cases usually respond poorly to medical treatment.91 Angle closure may occur acutely or subacutely due to posterior synechiae and pupillary block, or chronically with peripheral anterior synechiae.47 Patients with congenital syphilis and interstitial keratitis in infancy may have small anterior segments, microcornea, and narrow angles predisposing them to pupillary block angle closure later in life.92 Acute cases of angle closure may respond well to laser peripheral iridotomy, but if extensive synechiae are present, medical or surgical treatment may be needed.91 Intraepithelial cysts of the iris and ciliary body28 and lens subluxation or dislocation88 have also been reported as causes of angle-closure glaucoma in syphilis.
Sarcoidosis
Sarcoidosis is a disorder of noncaseating granulomatous inflammation affecting multiple organ systems including the eyes. Diagnosis is made by tissue biopsy from any area of suspected involvement, including the conjunctiva or lacrimal glands. It is more common in young adults and persons of African ancestry. In a study of 183 patients with sarcoidosis, 19% had uveitis and 6% had secondary glaucoma.93 A larger report of 532 patients found 53% with chronic anterior uveitis and 11% with secondary glaucoma.94 A review of 119 patients with sarcoid uveitis revealed 24% with elevated intraocular pressure, half of whom developed glaucoma.3 A review of 75 eyes with sarcoid uveitis reported only 7 patients with glaucoma; all of these patients had either intermediate or posterior uveitis as the primary form of inflammation.95 Blacks have a higher incidence than whites of ophthalmic involvement,93 uveitic glaucoma, and blindness.94
Although most commonly associated with anterior uveitis, sarcoidosis has been shown to be the leading cause of posterior, intermediate, and panuveitis associated with secondary glaucoma.3 One study found that nodular infiltration of the trabecular meshwork was the most common cause of ocular hypertension.96 Neovascular glaucoma associated with sarcoid-induced retinal vasculitis and ischemia has been described,97 as well as posterior scleritis with annular rotation of the ciliary body and angle closure.98 In patients with sarcoid uveitis, secondary glaucoma is often the major prognostic factor in a poor visual outcome.93,99 Eight of 11 patients with secondary glaucoma in one review experienced severe visual loss.93 Because treatment of sarcoidosis often involves use of chronic oral steroid, one must be very aware of the potential for steroid-induced glaucoma in these patients. It is also important to recognize the potential for sarcoid to involve the optic nerve directly, causing visual field loss that could resemble glaucomatous loss. This should be a particular consideration when a patient with sarcoidosis experiences rapid vision loss.
Vogt-Koyanagi-Harada Syndrome
Vogt-Koyanagi-Harada syndrome (VKH) is a bilateral panuveitis with central nervous system and dermatologic manifestations, occurring most commonly in darkly pigmented races.100 Secondary glaucoma has been reported to develop in 18% to 38% of cases,3,100,101,102 and may be due to open- or closed-angle mechanisms. In one study of 42 patients with VKH, 56% had open-angle glaucoma and 44% had angle closure.100 Acute angle closure has been reported as the presenting sign of VKH,103,104 and may be due to edema and anterior rotation of the ciliary body.105 Angle-closure attacks should be broken with laser peripheral iridotomy, but ongoing inflammation may result in closure of these iridotomies, and surgical iridectomy may be required.100 The success of standard or antimetabolite-augmented trabeculectomy is often low because of chronic inflammation in these patients, many of whom are young.100 Aqueous drainage devices may be the preferred filtering procedure.100
Behçet Disease
Behçet disease is a multisystem occlusive vasculitis which may be associated with uveitis in 66% of cases.106 Other hallmarks include retinal vasculitis, aphthous oral lesions, genital ulcers, and erythema nodosum.106 Acute uveitis may be accompanied by sterile hypopyon.107 Chronic or recurrent anterior uveitis has been reported to be complicated by glaucoma108 in 3% to 11% of cases.3,109,110 The uveitis can be difficult to control, and often requires the use of immunosuppressive agents.107
The outcome of treatment of refractory glaucoma with trabeculectomy with mitomycin C has been explored with two case-series studies. One study of 26 subjects reported achieving adequate control of IOP in 83.3% of subjects at 1 year follow-up and in 62.5% of subjects at 5 years follow-up,109 while another study of 13 subjects reported adequate IOP control in 82.6% of eyes at 1 year follow-up.111
Pars Planitis
Pars planitis, or intermediate uveitis, is a chronic inflammatory disorder of children and young adults. Clinical findings include inflammatory exudates over the inferior pars plana (“snowbank formation”), vitreous cells and debris, and retinal periphlebitis.25 Although the most common cause of visual loss is cystoid macular edema,25 glaucoma is reported to occur in 7% to 8% of cases.25,112 Reported mechanisms include peripheral anterior synechiae, iris neovascularization, and iris bombé.113 Treatment consists of periocular and systemic corticosteroids,25 which may be a contributing factor in the development of ocular hypertension.112 Resistant cases may require pars plana cryotherapy, vitrectomy, or systemic immunosuppressive agents.25
Sympathetic Ophthalmia
Episcleritis
Episcleritis is a benign, recurrent inflammation that uncommonly causes glaucoma. In two separate series of patients, 4% developed glaucoma, but this complication could not be attributed to the episcleritis alone. Some patients had preexisting primary open-angle glaucoma, and in others the problem was felt to be steroid-induced.27,37 Secondary glaucoma has also been reported where the intraocular pressure improved with steroid therapy. In these cases, inflammation of angle structures was felt to be the etiology.115 Although topical corticosteroids are often prescribed for this condition, topical or oral nonsteroidal anti-inflammatory agents can decrease symptoms effectively without the risk of inducing ocular hypertension.37,116 Because the symptoms are often self-limited and transient (1 to 2 weeks), in many cases no treatment at all is necessary.
Scleritis
Scleritis is a painful inflammation of the sclera that is associated with systemic disease in approximately half of all cases.27,37 Secondary glaucoma develops in 12% to 18%,27,31,37 and most commonly complicates sclerokeratitis37 and necrotizing scleritis.27 It is especially likely to occur when scleritis involves the entire limbal circumference.31 Mechanisms for elevated intraocular pressure in scleritis include damage to trabecular meshwork by associated uveitis,31 edema and inflammation around outflow channels,31,37 angle neovascularization,31 and corticosteroid treatment.31,37 Although usually associated with anterior scleritis, glaucoma is also reported secondary to posterior disease in which annular choroidal detachment may result in forward rotation of the ciliary body and angle closure.27,31,41,98,117 In eyes enucleated due to uncontrolled scleritis, evidence of glaucoma was found in 49%.31
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


