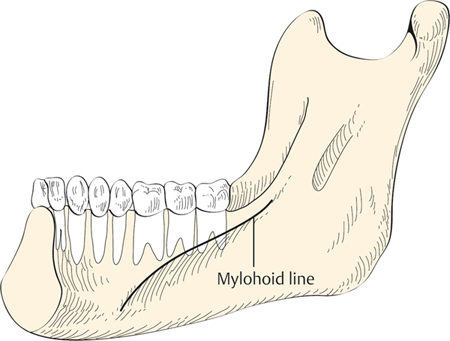
24 Infections of the Fascial Spaces of the Head and Neck Neck spaces are potential fascial planes extending from the skull base to the mediastinum. These potential spaces lie between the layers of the superficial fascia and deep layers of the cervical fascia surrounding the structures of the neck. The fascial layers limit and also direct the spread of infection. These spaces include submandibular, parapharyngeal, retropharyngeal, and prevertebral spaces. Infection of these spaces may vary from lymphadenitis, neck abscess, lethal necrotizing fasciitis, jugular venous thrombosis to descending mediastinitis.1–3 The knowledge of the neck spaces is invaluable to understand the spread of infection and to prevent potential life-threatening conditions. Neck infections were more common in the preantibiotic era. Even today, it still presents as a challenging condition.1–5 Once the infection or an abscess is formed in one fascial plane, it can potentially spread to other areas with a potentially lethal, especially airway, compromise.6 It can affect the pediatric as well as adult population; however, the cause may vary. In the pediatric population, the most common cause of infection is cervical lymphadenitis, and in adults, the infection is of odontogenic and peritonsillar origin. Submandibular space infections are common.4 Recurrent neck space infections may have underlying congenital cysts that usually need further investigation and treatment. The anatomy of the neck spaces is helpful in understanding the source, direction, and spread of infection (Table 24.1). It is the space of the floor of the mouth. It is bounded superiorly by the mucosa of the floor of the mouth, anteriorly by the mylohyoid and the anterior belly of the digastric muscle, posteriorly by the posterior belly of the digastric muscle and the stylomandibular ligament, medially by the hyoglossus and mylohyoid. It is in continuity with the floor of the mouth along the posterior edge of the mylohyoid. The relationship of the apices of the teeth to the mylohyoid line determines the source of infection from dental origin. The apices of the teeth anterior to the second molar lies superior to the mylohyoid line and the apices of the second and third molars extend below the mylohyoid line as shown in Fig. 24.1. Hence infection at the apices of the teeth anterior to the second molar would present with infection in the floor of the mouth, and infection posterior to the second molar would present with infection in the submandibular triangle of the neck.7 Table 24.1 Anatomy of the Fascial Neck Spaces
Anatomy of the Neck Spaces
Submandibular Space
Neck spaces | Boundaries | Contents |
Submandibular space | Superior: oral mucosa Inferior: anteriorly by mylohyoid and anterior belly of the digastric muscle Posteriorly: posterior belly of the digastric muscle and stylomandibular ligament Medial: hyoglossus and mylohyoid Lateral: skin, platysma, and mandible | Superior sublingual space: sublingual gland Inferior inframylohyoid space: submandibular gland |
Parapharyngeal space | Superior: skull base Anterior: pterygomandibular raphe Posterior: prevertebral fascia Medial: superior constrictor, pharyngobasilar fascia Lateral: deep lobe of the parotid gland, mandible | Prestyloid compartment: fat, lymph nodes Internal maxillary artery: pterygoid muscles Poststyloid compartment: carotid artery Internal jugular vein: cranial nerves IX, X, XI, XII Sympathetic chain |
Retropharyngeal space | Superior: skull base Inferior: superior mediastinum, tracheal bifurcation Anterior: pharynx, esophagus Posterior: alar fascia Lateral: carotid fascia | Lymph nodes |
Prevertebral space | Superior: skull base Inferior: coccyx Anterior: prevertebral fascia Posterior: vertebral bodies | Alveolar tissue |
Carotid space | Anterior: sternocleidomastoid Posterior: prevertebral space Medial: visceral space Lateral: sternocleidomastoid | Carotid artery, internal jugular vein, nerve X, ansa cervicalis |
Adapted from Lee KJ, Lee MS. Essential Otolaryngology: Head and Neck Surgery. New York, NY: McGraw-Hill; 2003.
Clinical Insights
Ludwig angina can lead to a potential airway compromise. The infection presents with a sudden onset of the inability to swallow and dribbling. This is because the infection in the sublingual space pushes the tongue to the roof of the mouth and posteriorly causes an airway compromise. It is one of the otolaryngological emergencies. The need of the hour is an experienced anesthetist and ENT surgeon ready for fiberoptic intubation and, if unsuccessful, for tracheostomy to secure the airway, followed by incision and drainage of the abscess.
Parapharyngeal Space
It is an inverted pyramidal space with its base at the petrous temporal bone of the skull base and its apex at the hyoid bone. It is bounded anteriorly by the pterygomandibular raphe, posteriorly by the prevertebral fascia, and laterally by the deep lobe of the parotid gland.7 Infection in this space is usually secondary to tonsillar/peritonsillar infections,4,5 as shown in Fig. 24.2.

Figure 24.2 Left peritonsillitis. The patient presented with odynophagia, fever, and a degree of trismus. It is the most common cause of deep neck space infections in adults.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


