Infection, Infiltration, and Benign Neoplasms of the Larynx
Craig R. Villari
Melissa M. Statham
Multiple infectious and benign conditions can affect laryngeal biomechanics and detrimentally affect laryngeal function and vocal performance. A variety of clinical presentations is possible ranging from dysphonia or dysphagia to airway compromise depending on pathology, the affected laryngeal subsite(s), and premorbid laryngeal anatomy. Treatment is targeted to the specific pathology, which is usually diagnosed from a thorough history, physical examination, and detailed laryngoscopy, but may also require more specific laboratory or radiologic examination.
INFECTIONS OF THE LARYNX
Viral Laryngitis
The most common cause of infectious laryngitis is viral (1). Viral laryngitis is typically self-limited with a normal duration of 5 to 7 days (2). Patients are usually dysphonic but may also present with odynophagia. History may include a viral prodrome with upper respiratory tract symptoms and physical examination usually demonstrates edematous, erythematous vocal folds (Fig. 67.1) with loss of normal vibratory pliability. Treatment includes supportive care with hydration and removal of laryngeal phonotory trauma (phonation and coughing, pollutants). The most common viral pathogens in the upper respiratory tract include rhinovirus, influenza A, B, C, and parainfluenza viruses. Patients with substantive vocal fold edema from viral laryngitis are at increased risk of repetitive phonotrauma leading to more significant vocal fold injury, such as midmembranous vocal fold lesions, epithelial and subepithelial trauma/ulceration, and scar (3). As such, these patients should ideally be limited to relative or absolute voice rest. Evidence suggests that anti-inflammatory medication may decrease subjective discomfort and decrease odynophagia, but one would not expect such treatment to decrease duration of illness as it could not affect the underlying viral etiology (4). Systemic corticosteroids may be utilized judiciously to treat moderate to severe laryngeal edema associated with very substantial symptoms, especially in patients with significant vocal demands that cannot be mitigated with behavioral modification. Antibiotics are not indicated in patients presenting with symptoms typical of viral laryngitis (1). Acute dysphonia lasting longer than 2 weeks is unlikely to result from viral laryngitis, and other etiologies should be investigated, including a detailed laryngoscopy.
Bacterial Laryngitis
Although rare, the physician should begin to consider a bacterial etiology when the supportive measures discussed above fail to decrease symptoms or if symptoms worsen after an initial plateau of symptoms. Initial clinical presentation may be similar to that of viral laryngitis, but supraglottitis and epiglottitis may result. As with the pediatric population, these conditions require escalated care, given the potential for airway demise. The causative bacteria are also similar to those in the pediatric population and include Haemophilus influenzae, Streptococcus species, and Staphylococcus species. Haemophilus species remain the most common but methicillin-resistant Staphylococcus aureus infections have been reported (1,5,6,7).
Diagnosis relies on endoscopic examination (Fig. 67.2) of the larynx. Radiologic imaging may be used to supplement endoscopic evaluation, and findings can include the classic “thumb-print” sign of supraglottic inflammation. Treatment depends on the clinical presentation with attention focused on airway competence. In a recent study, only 2 of 10 adult patients with supraglottitis evaluated over a 6-month period required airway intervention (8). Despite the majority of patients not needing airway protection, increased work of breathing and/or stridor must
be given proper credence. Medical treatment is targeted to the pathogen identified by culture. Additional supportive measures such as hydration and steroids are indicated (9).
be given proper credence. Medical treatment is targeted to the pathogen identified by culture. Additional supportive measures such as hydration and steroids are indicated (9).
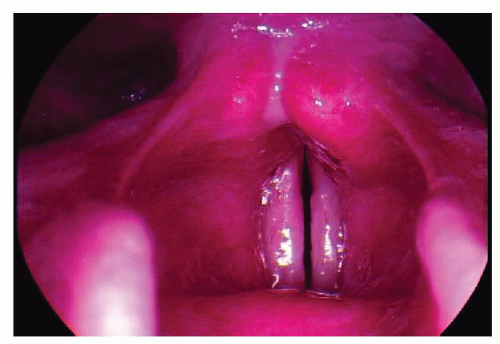 Figure 67.1 Acute laryngitis: note global laryngeal edema and erythema. |
Though not common in the United States, rhinoscleroma can also affect the larynx. Caused by Klebsiella rhinoscleromatis, patients tend to have laryngeal involvement (13/22 patients) and may need emergent tracheotomy to maintain airway patency (3/13 with laryngeal involvement) (10). In that series, all tracheotomy patients were decannulated with appropriate antibiosis. Pathologic examination demonstrates the gram-negative coccobacillus of Klebsiella on culture, as well as Mikulicz cells on mucosal biopsy.
Fungal Infection
Fungal laryngitis often occurs in immunocompromised patients, such as patients with systemic causes for immunosuppression (HIV, chemotherapy, diabetes, etc.) and individuals who are locally immunocompromised because of steroid inhaler use (11). Such infections are overwhelmingly candidal in etiology and will respond to systemic antifungal treatment (11,12). Patients will present with laryngopharyngeal symptoms, such as dysphagia and dysphonia. Physical examination demonstrates white plaque-like epithelial lesions of the mucosa surfaces, which may be focal or diffuse (Fig. 67.3). Conservative treatment with a systemic antifungal and a topical antifungal are appropriate, but shortinterval evaluation is necessary to assess resolution as persistent lesions merit biopsy and possible culture of lesions.
 Figure 67.2 Bacterial laryngitis: note posterior glottic purulence. |
Though the majority of fungal infections are Candida sp., other fungal organisms, such as blastomycosis, coccidioidomycosis, and histoplasmosis may also infect the larynx. These infections target immunocompromised patients as seen with Candida sp. infections but tend to occur in endemic geographic regions. Blastomycosis and histoplasmosis are prevalent in the Mississippi and Ohio River valleys, and coccidioidomycosis is endemic in the southwestern United States and Central America. However, patients may become infected outside of endemic areas (13). Biopsied lesions require culture with periodic acid Schiff and histologic examination to evaluate possible granulomatous conditions such as tuberculosis (14). Hematoxylin and eosin (H&E) staining demonstrates pseudoepitheliomatous hyperplasia with possible ulceration. Microscopic broad-based budding cells are a pathognomic feature of blastomycosis. Clinically, patients can present with a range of symptoms and physical exam findings, spanning from dysphonia to occult airway compromise (15,16). Treatment involves long-term systemic antifungal therapy with agents such as amphotericin or triazole.
Mycobacterial Infection
Laryngeal tubercular infection from Mycobacterium tuberculosis is classically associated with active pulmonary disease but can present as isolated laryngitis (17,18). Laryngeal
M. tuberculosis infections follow similar natural history to pulmonary tuberculosis and most commonly present as lesions in the posterior glottis. Patient factors include increased prevalence in underdeveloped countries, areas of over-crowding and communal living, and immunocompromised populations. While laryngeal infections present with similar symptoms as pulmonary infections (cough, hemoptysis, unintentional weight loss, fever, night sweats), patients may also present with laryngopharyngeal symptoms such as dysphonia, dysphagia, and odynophagia. Physical examination can demonstrate exophytic masses that mimic malignancy (19,20). Pathologic examination demonstrates caseating granulomas that are pathognomonic to M. tuberculosis infection. Treatment is targeted with multidrug regimens with culture guidance, as multidrug resistant M. tuberculosis strains are on the rise.
M. tuberculosis infections follow similar natural history to pulmonary tuberculosis and most commonly present as lesions in the posterior glottis. Patient factors include increased prevalence in underdeveloped countries, areas of over-crowding and communal living, and immunocompromised populations. While laryngeal infections present with similar symptoms as pulmonary infections (cough, hemoptysis, unintentional weight loss, fever, night sweats), patients may also present with laryngopharyngeal symptoms such as dysphonia, dysphagia, and odynophagia. Physical examination can demonstrate exophytic masses that mimic malignancy (19,20). Pathologic examination demonstrates caseating granulomas that are pathognomonic to M. tuberculosis infection. Treatment is targeted with multidrug regimens with culture guidance, as multidrug resistant M. tuberculosis strains are on the rise.
 Figure 67.3 Fungal laryngitis: note white fungal plaques with marginal erythema on midmembranous vocal folds. |
Other Infections
Less common infections of the larynx include leprosy and syphilis. Mycobacterial leprae and Mycobacterium lepromatosis, the causative infectious agents of leprosy, cause dramatic systemic and laryngeal epithelial changes. As with the other laryngeal infections, patients can present with variable severity in symptoms, with the most severe being occult aspiration or complete upper airway obstruction requiring tracheotomy (21,22). The World Health Organization recommends multidrug treatment with combinations of dapsone and rifampin with possible adjunctive clofazimine.
Syphilis is caused by Treponema pallidum infection and generally presents in stages. The primary stage generally presents to the otolaryngologist as a painless oropharyngeal chancre. During the secondary stage, patients can present with laryngeal manifestations, including leukoplakia, exophytic mass(es), and very rarely, decreased vocal fold mobility (23,24). Diagnosis involves serologic studies (venereal disease research laboratory or rapid plasma regain) and/or dark-field microscopy to visualize the pathopneumonic spirochetes sampled from suspect mucosal lesions. The mainstay of treatment is penicillin. For those patients with penicillin sensitivities, definitive allergy testing and desensitization may be required prior to treatment.
Idiopathic Ulcerative Laryngitis
Idiopathic ulcerative laryngitis (IUL) was first described in 2000 and a large clinical series was presented in 2011 (3,25). This condition involves dysphonia and severe cough following an upper respiratory tract infection and ulceration(s) of the midmembranous vocal fold. IUL appears to occur more in females than males (3). An etiologic agent(s) has not been identified and medical therapy with antibiotics, antifungal, and proton pump inhibitors are typically used but without an obvious positive response. These patients should be observed with serial office endoscopy (preferable video recorded) and the urge to perform a biopsy should be resisted. Biopsy will most likely be nondiagnostic and result in scar formation at the ulcer site. Patients should be counseled regarding the duration of the condition (average 3.3 months with a range from 2 to 10 months) and the possibility of vocal fold scar formation following the resolution of the ulcer(s) (3). If progression of the ulcer(s) occurs during serial examination a biopsy may be warranted.
INFILTRATION OF THE LARYNX
Multiple inflammatory processes can affect the larynx. These differ in their underlying presentation and pathologic and histologic features. As a group, these conditions generally cause decreased vocal fold pliability and/or lesions of the vocal folds, supraglottis, or subglottis. Symptoms correspond to the severity of vocal fold infiltration and potentially degrees of airway compromise.
Wegener Granulomatosis
Wegener granulomatosis is associated with necrotizing granulomatous inflammation and vasculitis of small blood vessels. The disease tends to affect the upper airway, the lungs, and the kidneys (26). The otolaryngologist may identify a patient because of nonhealing ulcers in the nasal cavity or, more rarely, subglottic airway stenosis. Diagnosis relies on thorough physical examination, nasal and laryngeal endoscopy, and testing for classical antineutrophil cytoplasm antibody (c-ANCA). Interestingly, 10% to 20% of those with airway symptoms have been reported to have a negative c-ANCA test (26).
The best treatment for these patients involves a multidisciplinary approach. Medical management with systemic corticosteroids and/or cyclophosphamide is used to obtain remission, and medications such as methotrexate, trimethoprim methoxazole, or azathioprine are used for maintenance therapy (26). Surgical treatments include subglottic expansion (subglottic releasing incisions with balloon or rigid dilation) and intralesional injection of corticosteroids (27). Subglottic stenting is generally avoided in favor of tracheotomy for recalcitrant presentations (28). In the setting of inactive Wegener granulomatosis with resultant subglottic stenosis, cricotracheal resection is also a viable treatment option.
Rheumatoid Arthritis
Rheumatoid arthritis affects millions of people worldwide with a predilection for females. It affects the larynx in just over one-fourth of cases (29). In comparison to unaffected control subjects, patients with rheumatoid arthritis had more frequent loss of higher frequency phonation, generalized dysphonia, decreased vocal fold mobility, and
laryngeal edema (30). These symptoms are modulated by the active status of the patient’s disease. Active rheumatoid arthritis tends to present with a substantial laryngitis with erythematous arytenoid mucosa (30,31,32). Chronic rheumatoid arthritis also selectively targets the arytenoid cartilages, but more specifically seems to affect the cricoarytenoid joint causing ankylosis and possible joint fixation (26). Patients may also present with rheumatoid nodules, also known as bamboo nodes, which are focal subepithelial lesions, typically on the superior surface of the membranous vocal fold. Treatment of rheumatoid arthritis relies upon medical management with immunomodular and anti-inflammatory treatments. Although outcomes data are sparse, surgical management may be indicated to manage airway symptoms or to judiciously remove rheumatoid nodules to improve phonation (32,33). (See Chapter 68) Alternatively, serial vocal fold steroid injections are a lessinvasive treatment that may improve vocal outcome (34).
laryngeal edema (30). These symptoms are modulated by the active status of the patient’s disease. Active rheumatoid arthritis tends to present with a substantial laryngitis with erythematous arytenoid mucosa (30,31,32). Chronic rheumatoid arthritis also selectively targets the arytenoid cartilages, but more specifically seems to affect the cricoarytenoid joint causing ankylosis and possible joint fixation (26). Patients may also present with rheumatoid nodules, also known as bamboo nodes, which are focal subepithelial lesions, typically on the superior surface of the membranous vocal fold. Treatment of rheumatoid arthritis relies upon medical management with immunomodular and anti-inflammatory treatments. Although outcomes data are sparse, surgical management may be indicated to manage airway symptoms or to judiciously remove rheumatoid nodules to improve phonation (32,33). (See Chapter 68) Alternatively, serial vocal fold steroid injections are a lessinvasive treatment that may improve vocal outcome (34).
Amyloidosis
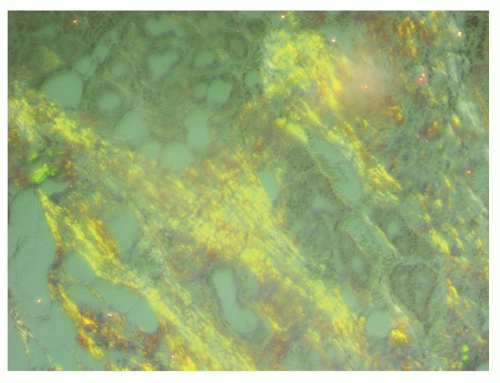
Amyloidosis is an autoimmune condition characterized by extracellular deposition of fibrillar proteins in affected tissue. Laryngeal involvement is rare and may not be associated with primary systemic amyloidosis. However, laryngeal amyloidosis may be present in conjunction with other systemic conditions such as multiple myeloma (35,36). Patients usually present with bulky deposition of amyloid protein with variable degrees of infiltration of the vocal fold, paraglottic space, and the supraglottis. Presenting features include cough, dysphonia, dysphagia, and possible stridor. Biopsy is required for diagnosis as amyloid has a pathognomonic apple green birefringence after staining with Congo red (Fig. 67.4). Referral is needed to examine for underlying secondary causes, such as systemic amyloidosis. There are reports of complete resolution with radiation therapy, but this treatment modality has not gained mainstream acceptance (37). Surgical intervention is usually undertaken to address specific symptoms and can improve vocal deficits. Recurrence is quite common (38).
 Get Clinical Tree app for offline access 
|


