4
Indirect Laryngoscopy
Prior to the introduction of flexible fiberoptic laryngoscopes in the mid-1980s, indirect laryngoscopy was the most important clinical tool for viewing the larynx and allowing the evaluation of laryngeal pathology. The technique involves placing a small mirror in the posterior pharynx and illuminating the larynx below with light reflected off of the mirror. Although indirect laryngoscopy is a “low-tech” method of laryngeal evaluation, facility with the technique requires significant practice, and most physicians have abandoned it in favor of the easily performed and well-tolerated flexible laryngoscopy. As a result, indirect laryngoscopy is rapidly becoming a lost art. Although the days of an otolaryngologist (let alone a primary care physician) wearing a head mirror may be numbered, indirect laryngoscopy is still commonly used as a screening tool for laryngeal pathology. Any complete review of laryngeal imaging must include a discussion of the indications, benefits, technical aspects, and the limitations of indirect laryngoscopy.
 Indications and Benefits
Indications and Benefits
Indirect laryngoscopy is the simplest way to examine the hypopharynx and larynx because it does not require special equipment, other than a light source, a head mirror, and a dental mirror, to perform the examination. Indirect laryngoscopy is, therefore, also exceedingly cost effective because it does not require expensive equipment. It is indicated in any patient with symptoms referable to the throat such as dysphagia, globus sensation, and hoarseness. Indirect laryngoscopy is a good choice for the initial examination of the hypopharynx in all patients presenting to the otolaryngologist. It allows an evaluation of hypopharyngeal anatomy, mucosal color, and vocal fold movement. Indirect laryngoscopy uses incandescent light, which has the advantage of minimizing color distortion so that the assessment of tissue color is reliable.
 Technique
Technique
The light source used for indirect laryngoscopy is typically placed to the right of the patient’s head and directed toward a head mirror worn by the examiner. The head mirror reflects the light onto the dental mirror held in the patient’s mouth. (Alternatively, the examiner can wear a headlight and forego the external light source and head mirror.) A small hole in the center of the head mirror allows binocular vision as the examiner looks through the hole with the left eye (Fig. 4.1). The head mirror should be placed as close to the eye as possible (Fig. 4.2). The head mirror is designed to focus the light at a convenient working distance. The position of the light source and the angle of the head mirror can be adjusted to focus the light onto the posterior pharynx properly.

Fig. 4.1 Head-mirror position over the right eye. The examiner looks through the hole in the head mirror.
Patient positioning for optimal indirect laryngoscopy is usually seated, with hips all the way to the back of the seat. The patient should be asked to lean forward, bending at the hips and lifting the chest and chin. A “sniffing” position with the jaw forward helps to position the tongue base anterior to the larynx (Fig. 4.3). Ideally, the head of the patient is above the head of the examiner. The examiner is seated in front of the patient with his or her knees to the right of the patient. Many patients will close their eyes during the examination, but it is helpful to have them keep their eyes open, looking upward. This prevents the patient from focusing solely on the sensation they are experiencing in the throat during the examination, precipitating a gag reflex.
Using tongue blades to hold the cheeks open, the posterior pharynx can be initially examined. This allows the examiner to make any minor adjustments of the light source and head mirror needed prior to beginning the indirect laryngoscopy. It also allows for an inspection of pharyngeal structures that will impact the ability to perform the examination such as size of tongue base, length of the soft palate, jaw opening, and so forth. It provides an opportunity to reassure the patient and prepare him or her for the indirect exam.

Fig. 4.2 Head-mirror position, close to the face.
The size of the dental mirror chosen for the examination should be large enough to provide a good view of the larynx but should not be so large that it cannot be positioned in the pharynx and manipulated to allow examination of all of the hypopharyngeal structures. The mirror must be warmed to prevent fogging during the examination. Care must be taken to ensure that the mirror is not too hot. The patient is asked to protrude the tongue, which is then held out of the mouth by the examiner. A gauze sponge is used by the examiner to grasp the tongue with the left hand. It is important that the patient be instructed to relax the tongue as much as possible, allowing the examiner to pull the tongue forward. This will minimize discomfort for the patient and will also maximize the posterior pharyngeal opening through which the examination will be performed. The index finger of the left hand can be used to elevate the upper lip. The dental mirror is then placed against the soft palate and gently pushed up and back (Fig. 4.4). Sensation to the soft palate is provided by the trigeminal nerve, which is typically not involved in the gag reflex, so touching the soft palate with the mirror is generally well tolerated. On the other hand, the glossopharyngeal nerve, which provides sensation to the base of the tongue, is involved in the gag reflex, and thus touching the tongue base with the mirror should be avoided. Similarly, the pharyngeal walls, innervated by the vagus nerve, will stimulate a gag if touched.
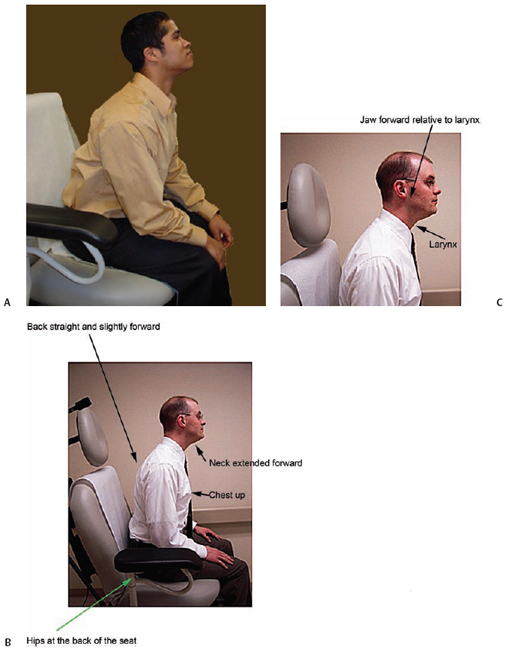
Fig. 4.3 (A) Optimal patient positioning for indirect laryngoscopy. Note head of the patient is positioned forward in a “sniffing” position. This moves the base of the tongue anterior to the larynx, improving a full view of the larynx. (B) Patient positioning during indirect laryngoscopy. The patient may need to bring his or her back off the backrest of the exam chair. (C) The anterior positioning of the head positions the jaw and tongue anterior to the larynx.
By angling the dental mirror back and forth, the larynx can often be viewed at this point in the examination. Asking the patient to say “EEEE” will also improve the ability to see the larynx. This maneuver elevates the larynx, depresses the tongue base, and brings the vocal folds together. It is important, however, to attempt to see the vocal folds while they are open, such as during respiration, as well, because lesions on the medial and undersurface of the vocal folds may be missed if the folds are only viewed during adduction.

Fig. 4.4 (A) Indirect laryngoscopy: The patient is positioned above the examiner. Notice how the patient’s mouth is at eye level for the examiner. (B) During indirect laryngoscopy, the light source is placed to the right of the patient’s head, reflected off the examiner’s head mirror and then reflected off the mirror placed in the oropharynx to illuminate the larynx. (C) Asking the patient to keep his or her eyes open during the examination helps the patient to tolerate the exam.
 Limitations
Limitations
Ten percent of patients will not be able to tolerate the examination well enough to allow a complete evaluation of all of the hypopharyngeal structures.1 A topical anesthetic applied to the posterior pharyngeal wall and tongue base can often aid in diminishing a strong gag reflex. Anatomic variations may also prevent a complete examination in up to 50% of patients.2 The anterior commissure is an area that is often difficult to see, especially if the patient has a large tongue base or is unable to relax enough to allow the tongue base to be pulled forward. A very anterior larynx is usually easier to see if the patient is positioned well above the examiner, allowing angling of the mirror to see forward of the tongue base. Nevertheless, the ability to see the laryngeal structures may be fleeting during the examination, requiring the examiner to make judgments based on a very quick view of the anatomy. The examiner may be able to see the larynx only during high-pitched phonation. This allows confirmation that the vocal folds are both moving but does not necessarily reflect conditions resulting in patient complaints. Subtle lesions are likely not to be detected, and vocal fold vibration cannot be seen with indirect laryngoscopy.
Because of the unnatural position of the patient during the examination and the restraining of the patient’s tongue, only very simple vocalizing can be evaluated with indirect laryngoscopy. The technique does not allow assessment during connected speech. This means that functional abnormalities are likely to be missed with indirect laryngoscopy alone.
Furthermore, indirect laryngoscopy does not provide for documentation of the examination. Monnery et al. found a 29% error rate in documentation with indirect laryngoscopy when the examiner created a drawing of the larynx to record the examination. Most commonly the error involved placing an abnormality on the wrong side of the larynx.1 Furthermore, descriptions or drawings of the larynx are too crude to allow detection of subtle changes in the findings on subsequent examinations. Because only one person can see the larynx during the examination, there is no possibility of simultaneous review of the findings by multiple individuals for the purposes of teaching, reviewing, or discussion.
In conclusion, indirect laryngoscopy is a long-established technique for laryngeal examination that is inexpensive and reliable in terms of tissue color assessment. It is limited by the technical skill required to achieve adequate examination, the patient’s ability to cooperate with the examination, the inability to view vocal fold vibration, and the lack of documentation.
References
1. Monnery PM, Smith WK, Hinton AE. Laryngoscopy findings in outpatient notes: the accuracy of the recording of the side of the lesion. Clin Otolaryngol Allied Sci 2001;26:278–280
2. Barker M, Dort JC. Laryngeal examination: a comparison of mirror examination with a rigid lens system. J Otolaryngol 1991;20:100–103
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


