Incisional Keratotomy
Daniel H. Chang
David R. Hardten
Incisional techniques for correcting astigmatic refractive errors were among the first refractive corneal procedures performed. Naturally occurring astigmatism is very common, and up to 95% of eyes have some clinically detectable astigmatism in their refractive error, with up to 75% of the general population having clinically significant astigmatism.1,2 This chapter provides an overview of incisional keratotomy, particularly for the correction of astigmatism; but a discussion of radial keratotomy (RK) is also provided both for historical and for conceptual purposes.
HISTORY
Astigmatic keratotomy appears to have been the first refractive corneal surgical procedure performed by ophthalmologists. In 1885, Schiötz,3 a Norwegian ophthalmologist, reported the case history of a patient who developed 19.50 D of astigmatism after cataract surgery. Four months postoperatively, he used a von Graefe knife to make a 3.5-mm penetrating incision at the limbus in the steep meridian, which reduced the astigmatism to 7.00 D. Lucciola of Terrin, Italy, was the first surgeon to report using nonperforating corneal incisions to correct astigmatism.4 In 1894, Bates,5 of New York City, described six patients who developed flattening of the cornea in the meridian that intersected a surgical or traumatic scar. He postulated that incisions of the cornea, made at right angles to the steeper meridian, might be used to correct astigmatism.
A Dutch ophthalmologist, Lans,6 performed one of the first systematic studies of refractive surgery while at the University of Leiden in 1896. His doctoral thesis, titled “Experimental Studies of the Treatment of Astigmatism with Nonperforating Corneal Incisions,” described carefully planned experimentation in rabbits to evaluate patterns of keratotomy, keratectomy, and thermokeratoplasty. These studies also defined some basic principles of astigmatic keratotomy. Lans showed that flattening in the meridian perpendicular to a transverse incision was associated with steepening in the opposite meridian and that deeper and longer incisions had a greater effect.
In 1939, Sato7,8,9,10,11,12,13 of Tokyo observed that spontaneous breaks in the Descemet membrane in patients with keratoconus could flatten the cornea and reduce their myopia. He performed both laboratory and clinical experiments on both posterior and anterior radial and astigmatic keratotomy incisions. Additionally, Sato discussed the concept of coupling, in which transverse incisions might be expected to flatten the steep meridian while simultaneously steepening the flatter meridian.
In the 1970s, several surgeons in the Soviet Union studied myopic and astigmatic incisions. In the early 1970s, Fyodorov et al.14,15,16 varied Sato’s technique and introduced the concept of radial incisions performed only in the anterior peripheral cornea and sclera. These investigators came up with the idea of varying the diameter of the central clear zone according to the degree of myopia being corrected. Fyodorov and Durnev17 also devised a multifactorial formula using patient and surgical variables in an attempt to improve predictability of the procedure. They investigated the effects of 32, 16, and 8 radial incisions in reducing myopia and decided that 16 was the optimal number of incisions for most cases. Fyodorov18 also discussed using several nonperforating anterior keratotomy patterns to correct myopic astigmatism.
The first RK procedure in the United States was performed by Bores et al. in 1978.19 Subsequently, there has been substantial laboratory and clinical research, including technologic advances in ultrasonic pachymeters and diamond micrometer knives that have made the procedure more predictable. In 1980, the National Eye Institute funded the Prospective Evaluation of Radial Keratotomy (PERK), which helped to define the safety and efficacy of RK.20 Four-, 5-, and 10-year results have demonstrated the problems of predictability, refractive instability, and poor visual quality inherent to the procedure.21,22,23,24 These problems, which could not be overcome by improved techniques and refined nomograms–as well as advances in the excimer laser–led to the rapid increase in excimer-based techniques with the concurrent decrease of RK in the mid and late 1990s.25
PRINCIPLES OF INCISIONAL KERATOTOMY
Many investigators have contributed to our understanding of astigmatic and radial keratotomy. The cadaver eye model has played a major role in predicting qualitative and quantitative results achieved with incisional refractive surgery.26,27,28,29,30,31,32 Corneal incisions increase the radius of curvature in a direction perpendicular to the incision, as if tissue were being added. Arcuate or transverse incisions therefore flatten the cornea in the meridian perpendicular to their location (with compensatory steepening of the orthogonal meridian). Radial incisions increase the midperipheral corneal circumference while maintaining the peripheral corneal and limbal circumference. This results in a flattening of the central cornea.
Astigmatic Keratotomy
Several basic incisional patterns have been investigated, including nonperforating, straight transverse, and arcuate keratotomy incisions, for the reduction of astigmatism. The following principles of astigmatic keratotomy33 apply to all types of astigmatism:
Astigmatic keratotomy incisions are placed in the steep corneal meridian. This is the meridian that is parallel to the plus-cylinder refraction axis and has the greatest power on central keratometry (Fig. 1).
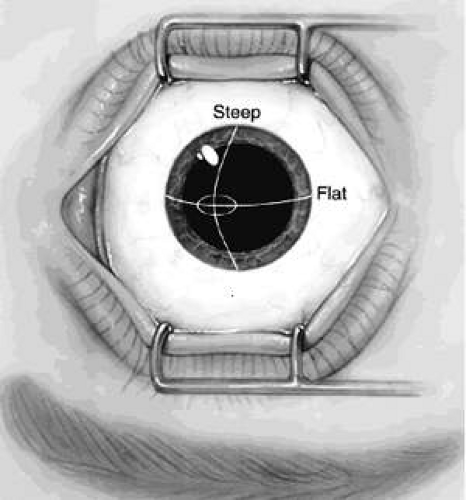
Fig. 1. With-the-rule astigmatism. Graphical depiction of keratometric measurement of corneal astigmatism. The steep and flat axes are shown.
Coupling refers to the ratio of corneal flattening along the incised meridian relative to the steepening along the unincised orthogonal meridian 90° away. Most arcuate incisions near the limbus are considered to have a coupling ratio of 1, and therefore there is no change in the spherical equivalent. The exact coupling ratio depends on the length, location, and depth of the incision. Relatively short transverse incisions measuring 1 to 1.5 mm or arcuate incisions approximating 20° tend to flatten the incised meridian more than they steepen the unincised meridian 90° away, thereby creating a hyperopic shift in the spherical equivalent (coupling ratio >1). Transverse incisions measuring 2 to 5 mm in length or arcuate incisions of 30° to 90° create a coupling ratio that approximates 1. Longer transverse incisions measuring 5 to 6 mm or arcuate incisions of 90° to 120° tend to induce more steepening in the orthogonal meridian than flattening in the incised meridian, thereby creating a myopic shift in the spherical equivalent (coupling ratio <1).
The astigmatic change per unit length of arcuate keratotomy incision varies inversely with the optical zone size. Therefore, transverse incisions at a 5-mm optical zone produce greater astigmatic correction than incisions placed near the limbus (limbal relaxing incisions). However, since the amount of induced irregular astigmatism and glare also varies inversely with the optical zone size, incisions at an optical zone less than 7 mm are rarely used.
Most of the effect of arcuate incisions is achieved with the first symmetric pair of keratotomy incisions; this accounts for about two thirds of the effect. Placement of an additional pair of incisions will increase efficacy 25% to 33%, but this is now rarely used because of an increase in irregular astigmatism.
Transverse or arcuate incisions should not cross radial or semiradial incisions. Previous clinical studies have shown that when two incisions intersect, the point of intersection undergoes poor wound healing, which often leads to epithelial inclusion cysts, exaggerated scar formation,34,35 and early and late wound dehiscence.
Radial Keratotomy
Although no longer routinely performed in the United States,36 basic principles are described for conceptual purposes of understanding corneal biomechanical properties. There are four surgical variables that can be adjusted to achieve the desired result.37,38,39,40,41
The degree of central corneal flattening varies inversely with the diameter of the central clear zone. A smaller diameter central clear zone has a greater net effect. RK incisions with an optical zone of 6 mm or greater have virtually no effect on the refractive error.42
The degree of central corneal flattening varies directly (but nonlinearly) with the number of incisions. Four radial incisions achieve greater than 70% of the effect of eight incisions.
The degree of central corneal flattening varies directly with the depth of the incisions. A double-pass technique offers a deeper incision centrally with less risk of inadvertently entering the clear optical zone (Fig. 2).43,44,45
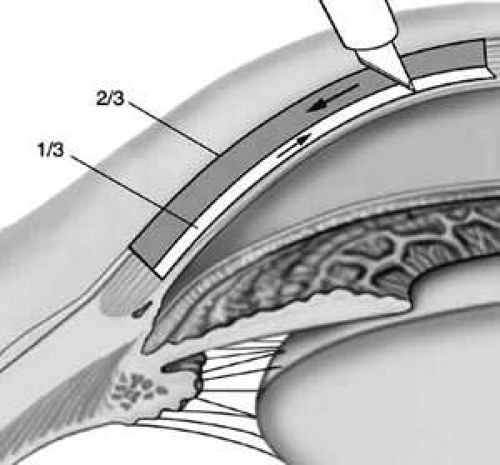
Fig. 2. The double-pass technique offers the benefits of both the Russian and American techniques. The initial incision is centrifugal and can be expected to create a beveled incision profile at the central optical zone. The blade is then pushed centrally from the peripheral 8-mm optical zone mark, deepening the initial incision until it can no longer be extended centrally. The two-step diamond blade is sharpened only on the bottom 250 μm of the vertical facet. Note the slight undercutting of the central optical zone.
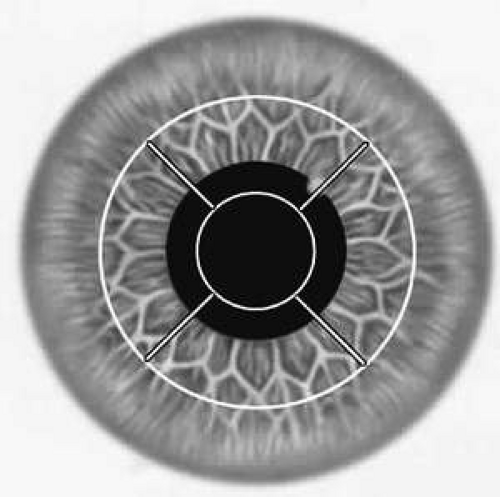 Fig. 3. In mini-RK, radial incisions are placed from a clear central optical zone to an 8-mm optical zone. The incision should extend from the inside of the central optical zone mark to the outside of the 8-mm mark. |
The two patient variables that clearly affect the outcome of RK39,40,41,47 are the degree of myopia and the patient’s age. Patients older than 30 years have an increased effect of 1.5% to 2% per year over age 30, and patients younger than 30 years have a lesser effect of 1.5% to 2% per year under age 30. There may be other patient characteristics that affect the results of surgery, but these are difficult to measure consistently. These variables include corneal curvature, preoperative intraocular pressure, gender, corneal thickness, corneal diameter, axial length of the globe, and ocular rigidity. Most studies show that male patients, high intraocular pressure, larger corneal diameter, a thicker cornea, a flatter cornea, and a higher ocular rigidity tend to result in a greater effect.
PATIENT SELECTION
Because of its inherent unpredictability, instability, and poor visual quality, RK has largely been abandoned for more modern techniques.36,48 Astigmatic keratotomy is less commonly performed as a primary procedure for the correction of refractive error but remains a useful adjunct at the time of cataract surgery.49,50,51
Up to 95% of eyes may have some clinically detectable astigmatism in their refractive error, and the incidence of clinically significant astigmatism in the general population has been reported to be in the 7.5% to 75% range, depending on the study and the definition of astigmatic error.1,2 Astigmatism greater than 0.50 D is seen in 44.4% of the population; 8.44% of the total population has astigmatism of 1.50 D or greater.1 Generally, about 10% of the population can be expected to have astigmatism greater than 1.00 D. At this level, the quality of uncorrected visual acuity might be considered unsatisfactory. An astigmatic refractive error in the range of 1.00 to 2.00 D might be expected to reduce uncorrected visual acuity to the 20/30 to 20/50 range, and 2.00 to 3.00 D should reduce uncorrected visual acuity to the 20/70 to 20/100 range.52
Visually significant astigmatism is also quite common after surgery. After extracapsular cataract extraction, astigmatism greater than 1.00 D is extremely common,53 with astigmatism greater than 3.00 D present in as many as 20% of cases. High astigmatism after penetrating keratoplasty is even more common, with astigmatism greater than 1.00 D basically being the norm.54 Troutman and Swinger55 estimated that nearly 10% of all clear penetrating keratoplasties are complicated by high postoperative astigmatism. Several surgeons have reported on the use of intraincisional relaxing incisions to correct this common postoperative problem.55,56,57,58,59,60,61 The surgical correction of naturally occurring astigmatism is considerably more predictable than the surgical correction of postkeratoplasty or postcataract astigmatism, in which individual wound healing may affect the outcome.
Patients considering astigmatic refractive keratotomy should have stable refractions. This must be confirmed by careful preoperative refractions. Keratometry is often a better measure of the true corneal astigmatism than is refraction. Corneal topography can help ascertain which patients might be poor surgical candidates because of preclinical keratoconus, irregular astigmatism, or some other corneal abnormality. Topography maps are helpful in preoperative assessment, surgical planning, and postoperative monitoring of patients undergoing incisional keratotomy.
Patients must understand that although nomograms for astigmatic keratotomy are based on averages for large numbers of procedures, the outcome of surgery cannot be precisely predicted for an individual eye. Additional refractive procedures may be needed to achieve the desired result, and spectacles or contact lenses may still be required for best visual acuity, even after surgery.
TECHNIQUE
Careful manifest refraction is performed preoperatively. In most cases, the keratometric and refractive cylinder power and axis will be compatible. Corneal topography will also verify the keratometric power and axis. In cases of significant disparity, remeasurement is warranted; but lenticular astigmatism may account for a difference in refractive and keratometric cylinder. Primary astigmatic keratotomy for naturally occurring astigmatism is based on the refractive cylinder and axis. At the time of cataract surgery and for postkeratoplasty astigmatism, keratometric values are generally used in conjunction with the refractive cylinder and axis.
Arcuate keratotomies are placed coincident with an optical zone, typically 7 mm or larger. Transverse incisions are easier to make, yet, may induce more irregular astigmatism than arcuate keratotomies, especially when placed coincident with a 5-mm optical zone, where they achieve the maximal effect. Incisions placed more central than a 5-mm optical zone are to be avoided because they are less effective, induce more glare secondary to irregular astigmatism, and carry a greater risk of inadvertently violating the visual axis. Arcuate keratotomy corrections are shown in Figure 4 and the appendix.
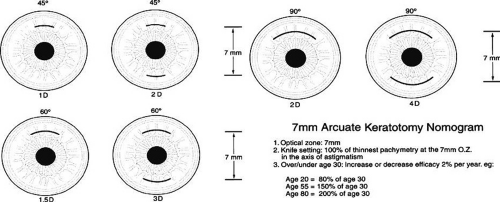 Fig. 4. Seven-millimeter arcuate keratotomy nomogram. Optical zone is 7 mm. Knife setting is 100% of thinnest pachymetry at the 7-mm optical zone in the axis of astigmatism. If the patient is older than or younger than 30 years of age, efficacy is increased or decreased 2% per year: age 20 = 80% of age 30; age 55 = 150% of age 30; age 80 = 200% of age 30. |
When using these nomograms, it is assumed that the transverse incisions flatten the steeper meridian the same amount as they steepen the flatter meridian (a coupling ratio of 1); so the net effect is no change in the spherical equivalent. This applies to paired arcuate incisions between 30° and 90°, similar to a 3-mm-long paired transverse incisions. Arcuate incisions less than 20° have a coupling ratio greater than 1, and arcuate incisions greater than 100° have a coupling ratio less than 1.
Younger patients tend to achieve a lesser effect than older patients; therefore, the nomogram is adjusted according to the patient’s age. The expected result should be decreased by 2% per year for patients younger than age 30 and increased by 2% per year for patients older than age 30.
The recommended equipment includes an operating microscope, arcuate keratotomy markers, a high-quality diamond micrometer knife, and an ultrasonic pachymeter.
The patient is centered under the operating microscope and the eye is positioned perpendicular to the microscope. The eye is anesthetized with 0.5% proparacaine hydrochloride. The patient fixates on the operating microscope light, which is turned to a low level, or a red fixation light mounted at the center of the microscope. The optical zone is then marked with a 7- to 10-mm optical zone marker, depending on the amount of astigmatism to be corrected. The steeper meridian is marked with a skin-marking pen using preoperative landmarks and an axis marker.
Special arcuate keratotomy markers are available that imprint both the desired optical zone and a graduated scale (Fig. 5). Arcuate incisions greater than 90° are not recommended because the coupling ratio diverges from 1, and late wound dehiscence is more common. The marker blades can be coated with a skin-marking pen or an ink pad for better visualization of the radial lines.
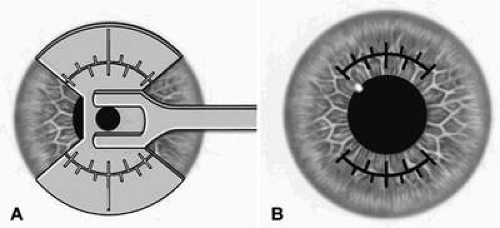 Fig. 5. A special arcuate keratotomy marker (A) delineates the desired optical zone as well as a graduated scale (B). |
The corneal thickness coincident with the intended optical zone in the steepest meridian is measured on both sides of the cornea intraoperatively with ultrasonic pachymetry (Fig. 6). A high-quality diamond knife is calibrated with a microscope capable of calibration to the micrometer level. The blade is set at 50 μm deeper than the thinnest paracentral pachymetry measurement or at 100% of the thinnest pachymetry reading at the desired optical zone. For 9- or 10-mm optical zone incisions, many surgeons set the blade at a fixed 600-μm setting.
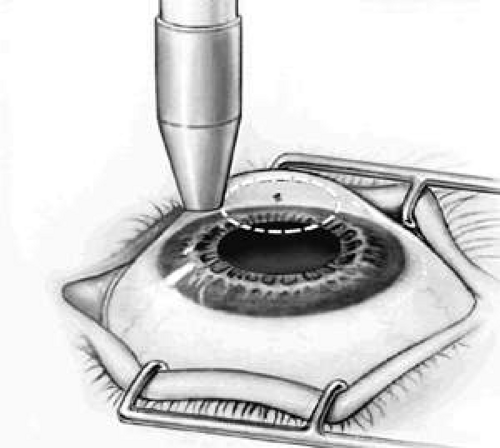 Fig. 6. Pachymetry is performed either adjacent to the central optical zone mark or directly over the area to be incised. |
The patient is asked to fixate on the operating microscope light or the fixation light. The knife is set into the cornea and allowed to seat for a full second. This is followed by a slow, steady guidance of the knife through the incisions (Fig. 7). A front-cutting knife allows the surgeon good visibility while pushing through the length of the keratotomy incision, thus improving accuracy. A square blade may provide better tracking.
 Fig. 7. Making the incision. |
The patient is generally seen 1 day and 1 month postoperatively. Topical antibiotics are continued until the corneal epithelium is re-epithelialized. The 1-month result correlates well statistically with the 1-year result, but additional astigmatic enhancement should not be considered until the refraction and keratometry measurements are stable.
Incisions with Concurrent Cataract Surgery
The principles of incisional keratotomy can be a useful adjunct in refining refractive outcomes at the time of small-incision cataract surgery.49,50,51 The cataract wound itself is an incision that can alter the astigmatism of the eye. Variation of the incision parameters such as length, width, and location can be useful but require rotation around the operating table and adjustments of the hand position and technique. Additionally, with increasing awareness of wound placement and construction for the prevention of bacterial endophthalmitis after cataract surgery,62 altering wound anatomy for astigmatism control may compromise the self-sealing quality of the incision. Some authors have suggested the creation of an opposite clear corneal incisions during cataract surgery to augment the astigmatic effect of the cataract wound.63 While this approach may be advantageous without requiring the acquisition of additional skills or equipment, creation of a second full-thickness incision may increase the risk of postoperative infectious complications.64
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


