4 J. Daniel Nelson Historically, the tests used to diagnosis dry eye assumed that a dry eye was dry, that there was insufficient tear production. Thus, tests of tear secretion, Schirmer’s 1 and 2 tests, basal tear secretion, cotton thread test, fluorescein dilution, tear film osmolarity, tear turnover, and tear clearance were used and were important in the diagnosis of the dry eye. It was also recognized that ocular surface disease often accompanied the dry eye. Fluorescein, rose bengal, and lissamine green dyes and impression cytology were used to assess the degree and severity of conjunctival and corneal involvement. Unfortunately, there seemed to be minimal if any correlation between symptoms and any of these clinical tests. In fact, there was generally no correlation between any of the tests.1–3 At present, however, these or similar tests are the only tests that are readily available to the practicing clinician. Although clinical tests are helpful, they do no supplant nor should they be the sole basis for diagnosing dry eye disease. A careful patient history and external examination of the eye is still necessary and required to form a complete differential diagnosis. One of the first things that the clinician should do when he or she enters the examination room is to look at the patient (Table 4-1). Often we focus so much on the “trees,” we forget the “forest.” Look at the patient’s hands for evidence of joint deformity characteristic of inflammatory arthritis. Observe the facial characteristics, lid position, and eyelid blinking. Does the patient have the facial characteristics of rosacea? Is the eyelid skin normal or is it erythematous, thickened, or leathery in appearance as seen in contact dermatitis and atopy? Are the eyelids in their proper position? Observe the lid position, blink rate, and completeness of eyelid closure with each blink. Is dermatochalasis, pseudoptosis, lagophthalmos, ectropion or entropion, or eyelid or brow ptosis present? An increased blink rate, involuntary lid closure, or spasm may be indicative of blepharospasm. Are there spasms of the lower face characteristic of hemifacial spasm? Blepharospasm with involuntary movements of the lower face suggests Meige’s syndrome. Individuals with dermatochalasis with pseudoptosis or blepharospasm often have dry eye symptoms. In these disorders, however, patients have more difficulty in describing their symptoms, often describing their eyes as feeling dry or moist or tired, with blurring of their vision. Foreign body sensation (like sand or gravel) and burning (like from soap or shampoo) are typical symptoms in patients with ocular surface involvement. Failure to elicit these symptoms should raise suspicion that the patient has another source for the symptoms than ocular surface disease due to keratoconjunctivitis sicca (KCS) or blepharitis.
In-Office Diagnostic Tests for Dry Eye Disease
Key Points
♦ History of Diagnostic Tests for Dry Eye Disease
♦ Clinical Examination and Evaluation
Observing the Patient
| What to Look at | What to Look for |
| Hands | Joint deformities characteristic of rheumatoid arthritis; eczema; psoriasis |
| Facial skin | Rosacea, butterfly rash of lupus erythematosus |
| Eyelid skin | Contact or atopic dermatitis |
| Eyelid position | Ptosis, ectropion, entropion, dermatochalasis, pseudo ptosis, brow ptosis; retraction, inferior scleral show’ proptosis |
| Eyelid blinks | Frequency, spasms, completeness of closure, lagophthalmos |
It is also important to estimate the blink rate. If time between eyelid blinks is longer than the tear breakup time (BUT), the patient is likely to have symptoms. Next, examine the palpebral portion of the lacrimal glands. Have the patient look down and out while you retract the upper lid. Observe the size of the lacrimal gland and its color. It is normally about the size of the fingernail on the little finger and fleshy pink in color. In Sjögren’s syndrome, the gland may be reduced in size, fibrotic, or even absent. In dacryoadenitis, it may be inflamed accompanied by a purulent discharge from the lacrimal duct orifices in cases of bacterial infection.
Determining Visual Acuity and Refraction
Visual acuity is determined and a best-corrected acuity is obtained at distance and near. Individuals, especially in the 40- to 60-year-old age group, with latent or undercorrected hyperopia or overcorrected myopia can also have complaints that can be confused with dry eye symptoms. Their complaints are of fatigue, tiredness, and blurring and not foreign body or burning sensations. It is common for patients with more severe dry eye with corneal involvement to complain of visual disturbances such as blurred and fluctuating vision.4
Examining the Patient
Slit lamp examination allows one to focus in on specific areas of the eyelids and ocular surface with a stereoscopic, magnified view. Here one can confirm initial observations and obtain a more detailed examination of what abnormalities may be present (Table 4-2). Position the patient at the slit lamp and before turning on the lamp and without illumination (to avoid reflex tearing), observe the height of the inferior tear meniscus. The normal height of the tear meniscus is 0.1 to 0.3 mm.5 A higher height may suggest a restriction or blockage in tear egress, whereas a lower level may suggest decreased lacrimal gland secretion. At this time, also observe the blink pattern as to the completeness of eyelid closure and the frequency of blinking. The eyelids normally touch each other on eyelid closure. A lax or floppy upper eyelid may override the lower lid, especially with forced eyelid closure. The normal blink rate is 10 to 12 blinks per minute.6 Now turn on illumination and observe tear film for mucin, debris, and “foam” along the eyelid margins. The presence of mucin and debris suggests inflammation. The presence of foam suggests blepharitis due to meibomian gland disease.
| What to Look at | What to Look for |
| Inferior tear meniscus | Height, mucus debris |
| Eye blink pattern | Completeness of lid closure |
| Eyelid skin | Contact or atopic dermatitis |
| Eyelashes | Misdirected, broken or missing lashes; collarettes |
| Eyelid margin | Abnormal lid position, irregularity; ulcerations; scurf, debris, and foam; punctum position and patency |
| Meibomian glands | Ease of expression of meibum, orifice patency, glandular dropout |
| Bulbar conjunctiva | Injection, conjunctivochalasis, irregularities (e.g., pterygia and pingueculae) |
| Palpebral conjunctiva | Papillae, follicles, subepithelial fibrosis |
| Cornea | Location and appearance of opacities, punctate epithelial keratopathy, punctate erosions, vascularity, filaments, mucin plaques |
At the slit lamp, “get a feel” for the eyelid skin by gently touching it with your finger. Is it smooth or is it the thickened, rough, and leathery skin that occurs in contact dermatitis or atopic eye disease? Normal skin folds run horizontal near the lid margins. Vertical skin folds running toward the lid margin suggest atopic or contact dermatitis.
Next, examine the eyelashes. Are they normal in number, appearance, and position? Are lashes missing (madarosis) or broken? Are there lashes growing aberrantly out of the meibomian gland orifices as are seen in severe blepharitis and ocular surface disease? Are the lashes rubbing on the cornea or conjunctiva? Is this due to abnormal lid position or trichiasis? A common cause of corneal epithelial defects is an aberrant lash or lashes rubbing on the cornea. The position of the eyelashes also provides a clue to the presence of meibomian gland inflammation. With meibomian gland inflammation, the lashes tend to rotate or “roll” downward (lash ptosis).
Eyelid movement is critical to the secretion of the meibomian glands, for spreading the tear film across the conjunctiva and cornea, and for removing ocular surface debris. During eyelid closure, the lower lid meets the lower eyelid and comes into contact with the marginal tear strip. As the upper eyelid ascends, it “pulls” the marginal tear strip superiorly, causing mixing and “resurfacing” of ocular surface by the tear film.7,8 Lower lid laxity or ectropion reduces efficient mixing and spreading of the tear film during eyelid opening and can result in a decrease or loss of the marginal tear strip. Normally, the upper lid should rest at the superior corneal limbus and the lower eyelid at the inferior corneal limbus. Widening of the interpalpebral fissure, seen in thyroid eye disease (lid retraction) or lower lid ectropion may result in poor or incomplete blinking, leading to exposure keratopathy. Poor blinking can reduce effective meibomian gland secretion. Eyelid closure, by rubbing across the cornea and conjunctiva, removes desquamated epithelial cells and adherent debris. Filaments occur in areas where there is ocular surface inflammation and a lack of lid movement across the conjunctiva and cornea (Fig. 4-1 ).9 For example, filaments are seen on superior cornea only in patients with superior limbic keratoconjunctivitis (SLK) of Theodore who also have upper eyelid ptosis, and in the interpalpebral fissure in patients with KCS who also have incomplete eyelid blinking. In patients with excessive, redundant upper eyelid skin (dermatochalasis or pseudoptosis), dry eye-like symptoms arise from the fatigue of having to elevate the upper eyelid to see. In severe cases this leads to decreased blinking and to poor tear film mixing and resurfacing, impaired meibomian gland secretion, and, when inflammation is present, corneal filaments.
Lid closure is also necessary to protect the ocular surface during sleep. Nocturnal lagophthalmos and lagophthalmos due to upper lid retraction from scarring may lead to exposure keratopathy. Ask the patient to blink normally and watch for complete eyelid closure. Then have the patient close the eyelids as though she or he were sleeping and then with a forcible closure. Failure to obtain normal closure may explain punctuate staining or epithelial defects in the interpalpebral fissure. During normal and forced eyelid closure also look for overriding of the upper lid over the lower lid. This occurs when both the upper and lower lids are lax, and it can result in chronic irritation of the palpebral conjunctiva.10
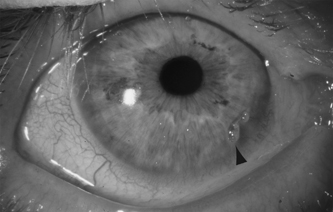
Figure 4-1 A corneal filament (arrowhead) in a patient with keratoconjunctivitis sicca and Sjögren’s syndrome.

Figure 4-2 Accessory punctum (arrowheads) in a patient with dry eye symptoms.
Compression of the nasolacrimal sac during eyelid closure creates a negative intraductal pressure, causing tears and surface debris to be pumped from the ocular surface tear film.11 Poor or incomplete blinking may result in accumulation of tear film debris, inflammatory cells, and inflammatory mediators. It is important to note the position, location, and patency of the puncta in the upper and lower eyelids of each eye. The inferior punctum is normally located medially, just lateral to the caruncle and pointing at and touching the globe, sitting in the tear meniscus. The superior punctum is similarly located and positioned along the upper eyelid. Although there are usually one punctum in each eyelid, extra or accessory functioning puncta do occur (Fig. 4-2). Canalicular fistulae also occur. Puncta may be congenitally absent or closed because of previous punctal occlusion. Abnormal punctum location, position, or patency can result in poor tear drainage and resultant epiphora. It is important to note the size of the punctal orifice as too small a punctum can result in clinical symptoms of epiphora. Too large a punctum may lead to increased loss of tears and symptoms of dryness. It is amazing at times to find that a seemingly very small punctal opening, which could not possibly contribute significantly to tear drainage, when occluded results in improvement of patient symptoms and clinical findings. It is equally amazing to find that narrowing of a large punctum or closure of an aberrant or extra punctum results in symptomatic and clinical improvement. In patients who have punctal plugs present, there may be signs of irritation where the head of the plug comes in contract with and rubs on the conjunctiva. Punctal plugs in the superior puncta tend to be more irritating than those in the lower puncta because of upper eyelid movement during the blink.
Next, examine eyelid margins. Along the anterior eyelid margin, the key clinical findings occur around the base of the eyelashes. Position and orientation of the lashes should be noted. Misdirected individual lashes suggest chronic inflammation involving the lash follicle or glands of Zeis located near the lash follicle. With inflammation involving the skin around the eyelash, ulceration occurs. As this heals, a crust forms (collarettes) that is carried upward, away from the skin, as the eyelash grows. Flake-like debris, or “scurf,” that occurs along the anterior lid margin due to skin desquamation can be confused with collarettes. Scurf, however, does not encase individual lashes nor is ulceration present. Collarettes are usually seen with bacterial infections of the eyelashes, whereas scurf is seen in seborrheic blepharitis. Crusting on the eyelashes is also often seen with the use of more viscous artificial tears.
The most important part of the external examination is the posterior eyelid margin. This is where most dry eye problems start (or perhaps end). The meibomian gland is the major participant in many, if not most, dry eye problems. Its normal lipid secretions are necessary for stabilizing the tear film at the air-tear film interface. The glands can be visualized from the palpebral conjunctival surface by transillumination though the eyelid. The normal meibomian gland orifices, located along the posterior eyelid margin, look like a tiny doughnut, with a small opening surrounded by a ring of slightly darker tissue. Manifestations of meibomian gland disease revolve around the characteristics of the gland’s secretion (meibum). Applying gentle pressure to the lower eyelid margin to express gland secretions allows assessment of the character of the meibum. The presence of drops of oil or lipid around the gland orifices is characteristic of meibomian gland hypersecretion that is seen in meibomian gland seborrhea. As meibomian gland disease progresses the meibum becomes cloudy, thicker, and paste-like. Plugging of the gland orifices and obstruction results. Instead of the normal, relatively clear orifice, the orifice appears as a whitish opacity due to the thickened meibum (metaplasia). Acute plugging of the glands can lead to inflammation and chalazia formation. Chronic plugging can lead to stasis, obstruction, meibomian gland degeneration, and dropout. Posterior eyelid margin irregularity, notching, or dimpling is a clue to chronic meibomian gland disease. Numerous systems have been developed in an attempt to standardize both a classification of blepharitis as well as that of meibomian gland dysfunction (MGD).12–14 Practically, from a clinical standpoint, classification of blepharitis as anterior or posterior is a useful first step. Anterior blepharitis tends to be more acute in nature and often infectious. Posterior margin blepharitis is defined by the status of the meibomian glands. Clinically, the most common form of meibomian gland disease is due to MGD. MGD can be classified as hypersecretory due to meibomian seborrhea or as obstructive (Fig. 4-3). Obstructive causes include primary focal or diffuse MGD and secondary MGD due to local or systemic disease. Skin conditions such as acne rosacea, atopic dermatitis, and psoriasis are the most common systemic conditions associated with MGD. The characteristics of the meibum, the presence of inflammation, and evidence of chronicity are most helpful in assessing MGD. The purpose of all such systems is twofold: to aid in the diagnosis and access severity and to allow pretreatment or baseline comparisons following therapeutic intervention. As with all grading systems, accuracy and consistency in observation and recording are important to determine whether a patient’s clinical picture is improving or worsening.
Examination of the conjunctiva is most helpful in determining the underlying cause of patient symptoms, in particular, in determining whether inflammation is present. The term ocular surface is commonly used. It is important to remember that the ocular surface includes not only the cornea and bulbar conjunctiva but also the lid margin and palpebral conjunctiva. It is critical to examine the palpebral conjunctiva of a patient suspected of having dry eye disease. This involves the routine eversion of the upper eyelid and inspection of the superior palpebral conjunctiva for follicles, papillae, subepithelial fibrosis, and foreign bodies. With lax upper eyelids and in floppy eyelid syndrome, the upper eyelids are everted almost too easily. The inferior palpebral conjunctiva should be similarly inspected. The presence of follicles is uncommon in the patient with dry eye. They are most commonly seen in topical drug toxicity or viral and chlamydial infections. Papillae are common in patients with dry eye disease due to conditions associated with inflammation, such as Sjögren’s syndrome. The presence of papillae suggests inflammation (Table 4-3). With KCS, the papillae usually are small in nature and more prominent on the inferior palpebral conjunctiva. In allergic conditions, the papillae are larger and often more prominent on the superior palpebral conjunctiva. The presence of subepithelial fibrosis suggests chronic inflammatory disease. Subepithelial fibrosis involving the inferior palpebral conjunctiva is seen in conditions such as ocular cicatricial pemphigoid, Stevens-Johnson syndrome, atopic eye disease, and severe chemical burns. Trachoma, in addition to all of these conditions, can also involve the superior palpebral conjunctiva.
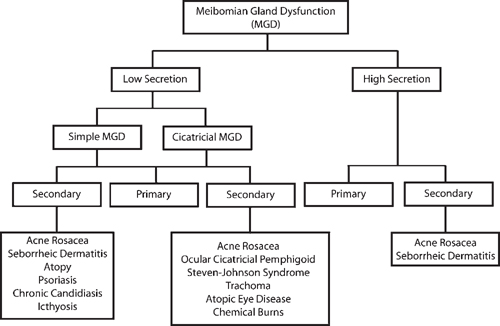
Figure 4-3 Classification of meibomian gland dysfunction.
|
Examination of the bulbar conjunctiva is straightforward. The most useful clinical findings are injection and the finding of surface irregularities. The presence of injection suggests that inflammation is present. Conjunctival injection must be distinguished from ciliary, episcleral, and scleral injection. Diffuse conjunctival injection is seen in inflammatory and infectious disorders of the cornea and ocular surface. Sectoral or localized injection is seen in association with a pinguecula or pterygium. The discomfort associated with conjunctival injection is usually a foreign body or burning sensation. Ciliary injection (ciliary flush) is perilimbal in location, a deeper red, and accompanied by deeper pain (ciliary spasm). Episcleritis and scleritis are not uncommon in primary Sjögren’s and secondary Sjögren’s syndrome due to rheumatoid arthritis. Episcleral injection may be sectoral or diffuse in nature, accompanied at times with a nodular elevation, and, usually but not always, painless. Scleral injection may be sectoral or diffuse, and like episcleritis, can be associated with a nodule (nodular scleritis). Scleritis, however, is characterized by a deeper red color due to scleral blood vessel dilation and engorgement and can be quite painful. Conjunctival and episcleral injection diminish in intensity with the application of topical 10% phenylephrine hydrochloride (Neo-Synephrine®, Bayer, Morristown, NJ), whereas scleral injection does not.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


