3

Imaging of the Paranasal Sinuses
Imaging of the paranasal sinuses has continued to evolve as treatment strategies and imaging technology have progressed. Cross-sectional imaging has proven to be a valuable tool for preoperative planning and has provided insight into the natural history of inflammatory sinus disease.1 Although plain films once occupied a central role in the diagnosis and follow-up of sinus disease, they probably have no role at this point.2 Uncomplicated sinusitis is a clinical diagnosis, and initial assessment of response to therapy is likewise clinical. A meta-analysis by Low et al3 suggests that initial imaging is not helpful when the suspicion is high or low, but it is beneficial when the diagnosis remains in doubt. Advanced imaging modalities primarily assist in assessing complications of sinusitis, failure of response to therapy, surgical planning for functional endoscopic sinus surgery (FESS), and in some institutions provide data utilized for intraoperative surgical guidance.
 Imaging Modalities
Imaging Modalities
Computed Tomography
Computed comography (CT) has become the primary imaging modality for assessing inflammatory sinus disease. Preoperative scanning is performed in the coronal plane, when possible, as this approximates the working plane during FESS and optimally displays the ostiomeatal unit (OMU) (Fig. 3–1). A cadaveric study by Melhem et al4 demonstrated that a slice thickness of 3 mm and a scan plane within 10 degrees of perpendicular to the hard palate best display the OMU. CT provides excellent bony anatomical detail and, with the evolution of helical scanning, can rapidly acquire thin-slice axial data suitable for three-dimensional or multiplanar reformatting in sagittal, coronal, or oblique planes5 (Fig. 3–2). Patients who cannot tolerate the neck hyperextension necessary for prone or supine coronal scanning (Fig. 3–3) and patients with extensive dental restorations (Fig. 3–4) are good candidates for thin-slice helical scanning with reformatting.6 Helical scanning defines a combination of continuous rotational tube head motion about the patient, along with continuous feed of the patient through the scanner. This results in significantly shorter scan times, less motion artifact, and minimization of volume averaging artifact. Data for intraoperative guidance are always acquired as a thin section helical dataset to permit real-time multiplanar display in the operating room. Newer multidetector CT scanners allow acquisition of 4 to 32 slices with each scanner rotation. 64 slice units are in development. This degree of coverage dramatically reduces motion artifact, and in conjunction with 0.5 mm to 0.75 mm beam collimation permits very high-resolution multiplanar reformatted images.
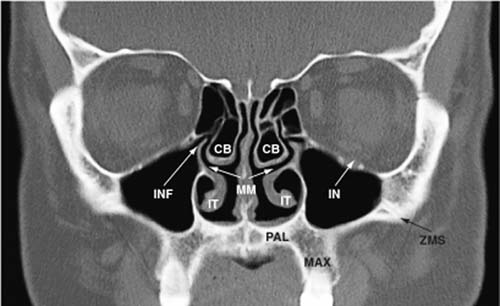
FIGURE 3–1 Direct coronal scan through the osteomeatal unit showing relevant anatomy. cb, concha bullosa of middle turbinate; IN, infraorbital nerve and canal; INF, infundibulum; IT, inferior turbinate; MAX, maxillary dentoalveolus (tooth-bearing area); MM, middle meatus (text label overlies the nasal septum); PAL, hard palate; ZMS, zygomaticomaxillary suture.
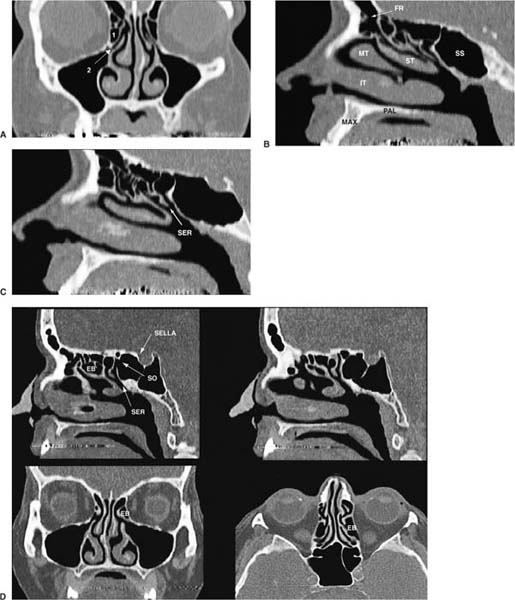
FIGURE 3–2 (A) Coronal reformat of axial CT data at approximately the same point as Figure 3–1. This permits a more direct coronal plane and avoids significant dental restoration artifact in the region of interest. (B) Sagittal reformat from the same axial dataset. The frontal recess is prominantly displayed, and is clearly an hourglass-shaped structure, not a duct. FR, frontal recess; IT, inferior turbinate; MAX, maxillary dentoal veolus; PAL, hard palate; MT, middle turbinate; SS, sphenoid sinus; ST, superior turbinate. (C) Sagittal reformat showing the sphenoethmoid recess (SER), as well as drainage pathways from posterior ethmoid air cells. (D) Direct axial and reformatted coronal and sagittal images showing the ethmoid bulla (EB), sphenoid ostium (SO), and SER.
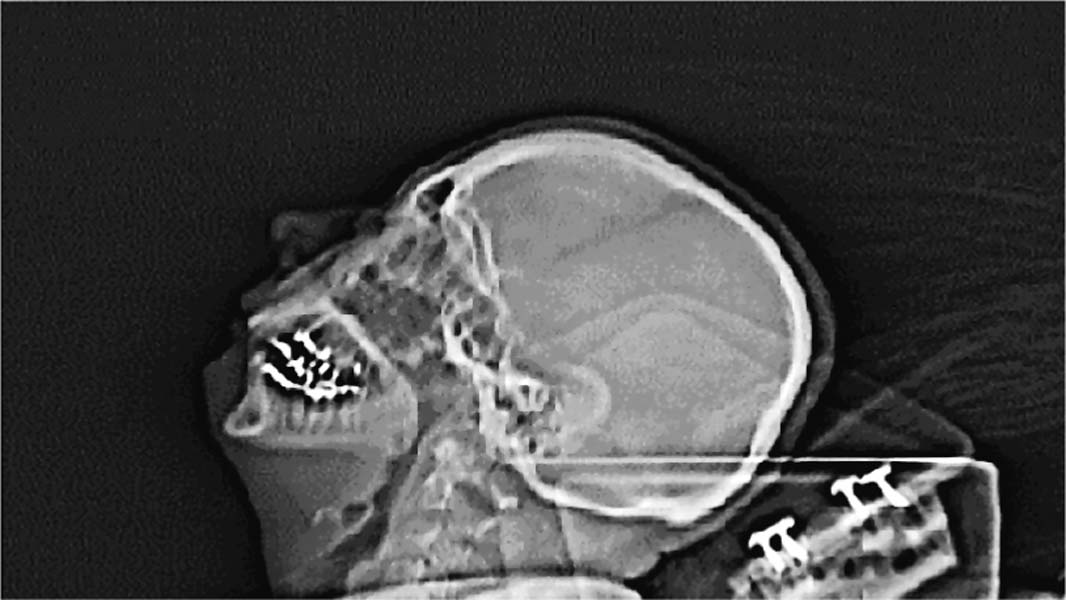
FIGURE 3–3 Topogram of patient in supine hyperextended position.
The Hounsfield number or unit (HU) describes tissue density in CT (Table 3–1). Because the subcutaneous and intraorbital tissues contain substantial fat, there is usually sufficient contrast to recognize extension of disease to these areas from the sinuses. Diagnosis of subtle intracranial complications from sinus disease is more problematic with CT.7 Iodinated intravenous (IV) contrast is not necessary in most routine or preoperative cases; however, it is very useful to demonstrate abnormal enhancement at the margin of an area of inflammation or abscess. This enhancement may be the only finding in a situation such as an early subperiosteal postseptal abscess. Though relatively safe, use of IV contrast is not trivial, and a few simple points should be considered. Prior reaction to contrast should prompt brief questioning regarding its nature and whether the patient is aware if “ionic” (high osmolar) or “nonionic” (low osmolar) contrast was used. One or two hives with no therapy necessary should be noted but will probably not require a change in protocol for the scan. More significant reactions such as laryngeal or oropharyngeal edema and respiratory compromise will generally require rethinking the necessity for contrast, considering magnetic resonance imaging (MRI), or utilizing a steroid prep combined with low osmolar IV contrast. When considering contrast-enhanced CT, the radiologist at your institution should be contacted when confronted with a history of significant prior contrast reaction.
Substance | Hounsfield Units |
Air | −1000 |
Fat | −100 |
Infiltrated fat | −30 to + 20 (approx.) |
Water | 0 |
Simple fluid | 0 to + 20 |
Proteinaceous fluid | +20 to +50 |
Soft tissue | +30 to +50 |
Acute blood (normal hematocrit) | ~ +80 |
Bone | +500 to +1000 |
Metal | > +1000 |
Normal hematocrit is approximately 80 HU. Hounsfield number decreases with decreasing hematocrit.
Renal dysfunction is a relative contraindication to iodinated contrast administration. At our institution, a baseline creatinine is not required for patients younger than 60 years with no history of renal compromise. We generally will not administer any iodinated contrast to patients with a creatinine greater than 2.0 mg/dL, unless they are undergoing regular dialysis. A diabetic with a creatinine of 1.4 to 2.0 mg/dL, where contrast-enhanced CT is essential, will be hydrated and receive low osmolar contrast. Again, if any questions arise regarding contrast administration for a patient at risk, discussion with the responsible radiologist is best prior to scheduling the scan.
Finally, a general discussion of CT would not be complete without addressing the issue of limited sinus CT as a substitute for plain films in the early workup of sinus disease. Often it seems these exams are done in an attempt to convince patients that their complaint is being investigated, while trying to limit the cost of the exam. The evaluation of an initial episode of acute sinusitis and the response to therapy is a clinical exercise. Subjective complaints by the patient correlate poorly with CT findings, as demonstrated by Bhattacharyya et al.8 If the patient demonstrates persistent disease following therapy or complicated sinusitis or is deemed a candidate for surgical intervention, then complete coronal evaluation becomes the preferred option. Limited axial or coronal sinus CT probably adds little to patient management (Fig. 3–5). One exception to this may be patients about to undergo bone marrow transplantation. Oberholzer et al9 studied 80 patients prior to bone marrow transplantation, revealing disease requiring therapy in 17 (21%). Patients with leukemia and non-Hodgkin’s lymphoma were the most frequently affected. Given the profound immunosuppression these patients are subjected to, limited study to exclude significant sinus disease without complete evaluation of the OMU may be reasonable.

FIGURE 3–4 Severe dental artifact. When extensive restorations are present, thin section axial scanning with reformatting may be preferable.

FIGURE 3–5 (A,B) Axial images pretreatment for acute sinusitis (simple CT protocol: thick sections, axial, five to nine images). (C) Coronal scan posttherapy.
Magnetic Resonance Imaging
Magnetic resonance imaging also provides cross-sectional data and has been preferred over CT when coronal or sagittal imaging is desired. Helical CT with multiplanar reformatting has lessened the importance of this distinction. MRI utilizes the magnetic properties of protons in a strong magnetic field to generate weak radiofrequency signals that yield the diagnostic image. Unfortunately, from the perspective of sinus imaging, bony detail is more difficult to appreciate, as cortical bone has essentially no signal.10 Additionally, the examinations are long compared with CT, and sedation may be required. MRI is probably superior to CT in most instances to assess potential intracranial complications of sinusitis or operative intervention.10 One important point regarding MRI is that signal strength from the tissues, and hence image quality, is directly related to the strength of the scanner magnetic field. Most open MRI units operate at 0.3 to 0.5 Tesla (1 T = 10,000 × earth’s gravitational field strength). High-field scanners operate at 1.5 Tesla. Subtle abnormalities may be missed in a low-field scanner. If medical conditions permit, claustrophobic patients will receive a higher quality study sedated in a high-field scanner rather than giving in to their request to be imaged in an open system.
Ultrasound
Ultrasound has been used recently for diagnosis of acute sinusitis in intensive care unit (ICU) patients11 and has been investigated as a primary care screening tool,12 but it has essentially no utility in presurgical imaging.
Nuclear Medicine
Nuclear imaging will generally be utilized for diagnosis of osteomyelitis in cases of complicated sinusitis. Intrathecal injection of tracer may be useful as a screening exam prior to CT cisternography when trying to identify cerebrospinal fluid (CSF) leaks.
 Anatomy
Anatomy
Surgical anatomy has been covered previously. This discussion will focus on the radiologic appearance of normal and variant anatomy.
Normal Anatomy
A key concept underpinning functional endoscopic sinus surgery is that inflammatory sinus disease primarily results from impaired sinus drainage through the ostiomeatal channels. The goal of FESS is to restore physiologic drainage patterns. Radiologic examinations should be customized to optimally display the ostiomeatal channels that provide ventilation to and mucociliary clearance from the frontal, maxillary, ethmoid, and sphenoid sinuses. The term ostiomeatal unit defines air passages communicating between the frontal, anterior ethmoid, and maxillary sinuses, and is usually the main focus of FESS. Two other key areas to evaluate and describe are the frontal recess (FR) and the sphenoethmoid recess (SER).
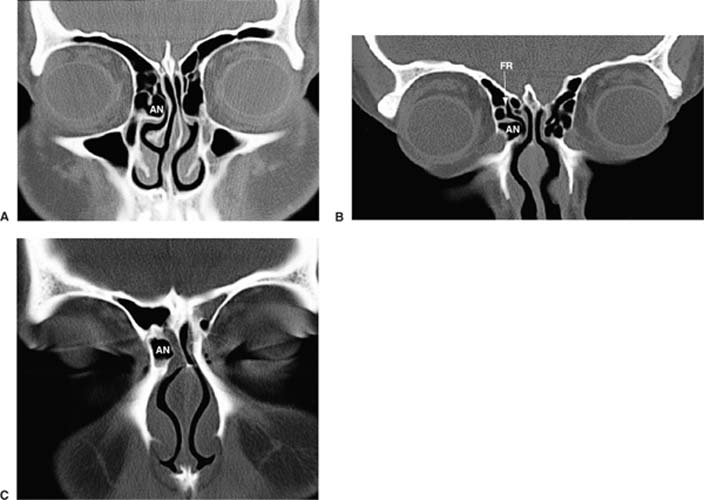
FIGURE 3–6 Agger nasi cells are distinguished from the ethmoid bulla by their more anterior location. They may impair drainage via the frontal recess. The term anterior ethmoid air cell may help avoid confusion. Images A–C show the appearance as one moves anteriorly. Note that the air cell is still visible with soft tissues of the eyelids and globes barely within the plane of imaging. AN, aggar nasi cells; FR, frontal recess.
Initial coronal CT images display the frontal sinuses. The FR is an hourglass-like narrowing between the frontal sinus and the anterior middle meatus. Sagittal images clearly demonstrate it is not a tubular structure, and therefore the term frontal recess is preferred over nasofrontal duct (Fig. 3–2B). Anterior, lateral, and inferior to the FR are the most anterior ethmoid air cells, usually referred to as agger nasi cells. (The nomenclature for these structures is undergoing modification to more directly reflect anatomical location, and so the term anterior ethmoid air cell is increasingly used.) They are usually immediately subjacent to the FR, and thus their size may directly influence drainage via the FR and the anterior middle meatus (Fig. 3–6) The frontal recesses are in actuality residual spaces remaining following pneumatization of the agger nasi cells and the ethmoid bulla more posteriorly. They are often fairly narrow and are common sites for inflammation and impaired mucociliary clearance.
The ethmoid infundibulum extends between the uncinate process and the inferomedial border of the orbit and is the primary drainage pathway from the maxillary sinus. The uncinate process of the ethmoid bone is a superomedial extension of the lateral nasal wall. Anteriorly, the uncinate process joins the medial wall of the agger nasi cells and the posteromedial wall of the nasolacrimal duct. The free edge of the uncinate process extends posterosuperiorly, and the lateral margin defines the superomedial aspect of the infundibulum. The ethmoid bulla is posterolateral to the free edge of the uncinate, usually the largest of the anterior ethmoid cells, and enclosed laterally by the lamina papyracea (Fig. 3–7). The ethmoid bulla represents a key surgical landmark, presenting a characteristic bulge in the superolateral nasal wall visible through the surgical endoscope. For this reason, it is considered separately from the other components of the ethmoid labyrinth, and it is referred to as though it is a single structure even though it often contains more than one air cell. The hiatus semilunaris is defined as the gap between the ethmoid bulla and the free edge of the uncinate process, and it medially communicates with the middle meatus. Laterally and inferiorly, the hiatus semilunaris borders the infundibulum.
The lateral nasal wall is the origin of the superior, middle, and inferior turbinates. The turbinates divide the nasal cavity into the superior, middle, and inferior meati. The superior meatus drains the posterior ethmoid air cells, as well as the sphenoid sinus via the sphenoethmoid recess. The middle meatus drains the frontal sinus via the frontal recess, the maxillary sinus via the maxillary ostium leading into the ethmoidal infundibulum, and anterior ethmoid air cells via the ethmoid cell ostia. The inferior meatus receives drainage from the nasolacrimal duct, usually visible on three to four adjacent coronal sections through the anterior midface.
The middle turbinate attaches anteriorly to the medial wall of the agger nasi (anterior ethmoid) cells and the superior edge of the uncinate process. Superiorly, the middle turbinate adheres to the cribriform plate. Posteriorly, the middle turbinate connects to the skull base via the basal or ground lamella (Fig. 3–8) that fuses with the lamina papyracea just posterior to the ethmoid bulla. In most patients, the posterior wall of the ethmoid bulla is intact, and an air space is usually found between the ground lamella and the ethmoid bulla. This air space, the sinus lateralis, may extend superior to the ethmoid bulla, communicating with the FR. Dehiscence or absence of the posterior wall of the ethmoid bulla is not unusual and may permit communication between these two usually separated air spaces. The posterior ethmoid sinus consists of air cells between the basal lamella and the sphenoid sinus. The number, shape, and size of these air cells vary.
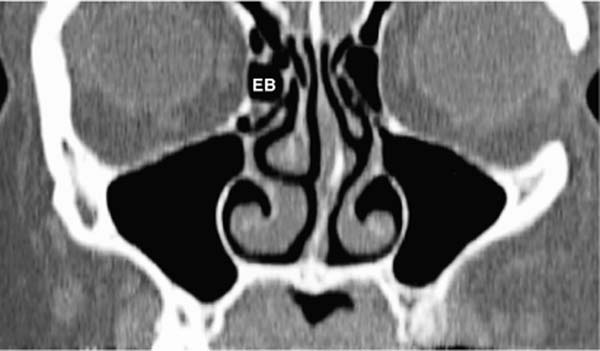
FIGURE 3–7 Reformatted axial scan showing the ethmoid bulla (EB). Note that it is more posterior, in the region of the uncinate and infundibulum.
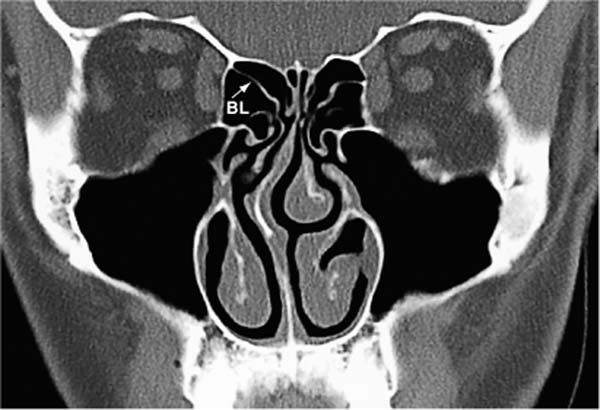
FIGURE 3–8 Basal lamella (BL) connecting the middle turbinate to the lamina papyracea. Damage may occur in this region from excessive traction during middle turbinectomy. Note the septal deviation and hypoplasia of the right middle turbinate (also the lack of any demonstrable sinus mucosal disease).
The sphenoid sinus is most posterior, contained within the clivus, lying anteroinferior to the sella turcica. Its ostium is usually in the superomedial portion of the anterior sinus wall and drains via the SER into the posterior aspect of the superior meatus. The SER is just lateral to the nasal septum and is best seen with axial or sagittal images (Fig. 3–2C,D).
The sphenoid sinus and posterior ethmoid air cells change in relation to one another as one moves from the midline laterally. Near the midline, the sphenoid sinus is the most superior aerated cavity, and laterally, the posterior ethmoid air cells become the most posterior and superior extent of the paranasal sinuses.
Anatomical Variations
The relation of a particular variation to inflammatory disease is related to its ability to narrow or obstruct the air passages of the FR, OMU, or SER. From a presurgical standpoint, important variants influence the risk to adjacent structures during specific operative maneuvers. Special note is made of encephalocele, which is a contraindication to all but the most limited endoscopic manipulation.
Septal Variants
Septal bowing may compress the middle turbinate laterally, narrowing the middle meatus. Bony spurs are often associated with septal deviation and may compromise the OMU (Fig. 3–9).
Middle Turbinate Variants
Concha bullosa defines a middle turbinate that is aerated, enlarges, and may obstruct the middle meatus or infundibulum (Fig. 3–10). Middle turbinate concha bullosa may be unilateral or bilateral, superior turbinate involvement is less frequent, and inferior turbinate involvenent is rare. The mucous membrane lining the concha bullosa is no different from the rest of the sinuses and may display inflammatory change, including development of air-fluid levels. In most people the major curvature of the middle turbinate is projected toward the septum. A paradoxical middle turbinate curves laterally (reverse scrolling) and may narrow the middle meatus (Fig. 3–11). A study by Lam et al13 shows no specific relationship between concha bullosa and chronic sinusitis.

FIGURE 3–9 Septal deviation with spur. Again, note hypoplasia of the right middle turbinate.
Uncinate Variants
The free edge of the uncinate process has a variable course. Lateral deviation narrows the infundibulum. Medial deviation may narrow or obstruct the middle meatus. Occasionally, the free edge of the uncinate is fused to the orbital floor or lamina papyrcea, described as an atelectatic uncinate process. Inflammation or hypoplasia of the ipsilateral maxillary sinus may be present related to partial or complete obstruction of the infundibulum. Occasionally, the uncinate may be aerated (Fig. 3–12).
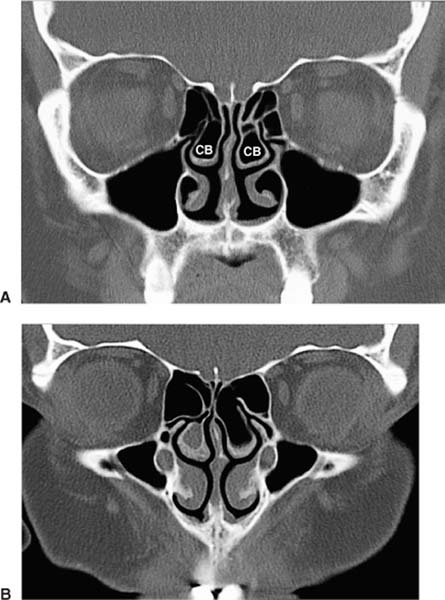
FIGURE 3–10 (A) Bilateral concha bullosa. (B) Bilateral concha bullosa with retained secretions versus mucosal thickening.

FIGURE 3–11 Paradoxical left middle turbinate curves laterally and may obstruct the middle meatus.
Ethmoid Variants
Haller’s cells are ethmoid air cells that extend along the roof of the maxillary sinus and may contribute to narrowing of the infundibulum (Fig. 3–13). Again, nomenclature is shifting to more accurately describe anatomy, and so the term orbital air cell is frequently used. The ethmoid bulla may enlarge to narrow or obstruct the middle meatus and infundibulum. Large agger nasi cells can obstruct the frontal recess. Onodi cells are rare lateral and posterior extensions of the posterior ethmoid air cells, extending in close proximity to the optic nerves as they exit the orbits. Failure to recognize this variant may place the optic nerves at risk. Dehiscence of the lamina papyracea, either congenital or post-traumatic, may increase the risk of orbital entry. An aerated crista galli may communicate with the frontal recess (Fig. 3–14). Obstruction of this ostium can lead to chronic sinusitis and mucocele formation. Although usually small, the presence of this variant may increase the risk of entry into the anterior cranial fossa.
Sphenoid Variants
Pneumatization of the sphenoid sinus can extend into the anterior clinoids or present as very large lateral recesses (Fig. 3–15). The former may place the optic nerves at risk; the latter may increase the risk of inadvertent perforation of the carotid artery. The septations of the sphenoid sinus are variable and may be incorporated in the bony wall covering the internal carotid artery. The margin of the carotid canal or optic canal adjacent to the sphenoid sinus may be dehiscent.
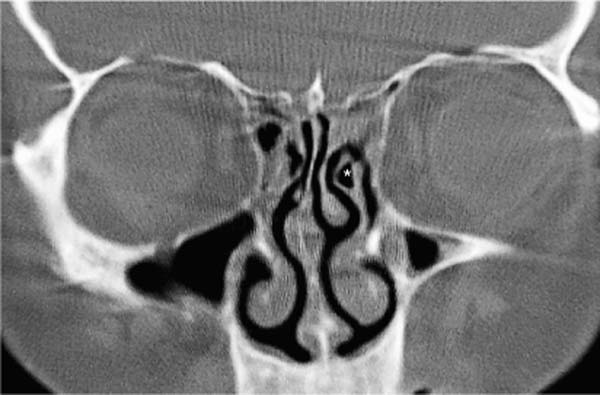
FIGURE 3–12 Aerated uncinate (*) is uncommon but may obstruct the infundibulum.
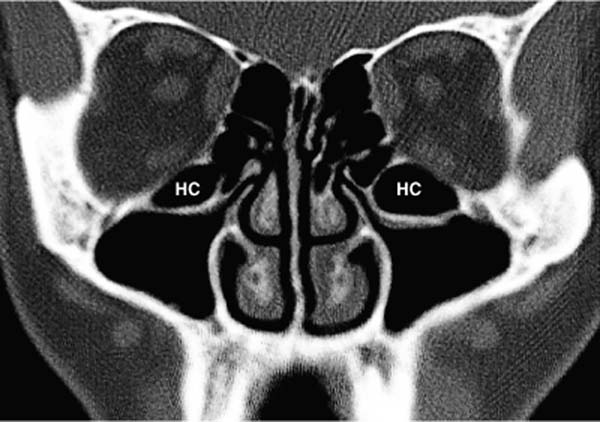
FIGURE 3–13 Large bilateral Haller’s cells (HC). Again, nomenclature is shifting to more descriptive terminology, so the term inferior ethmoid air cell is increasingly used.

FIGURE 3–14 Aerated crista galli (CG).
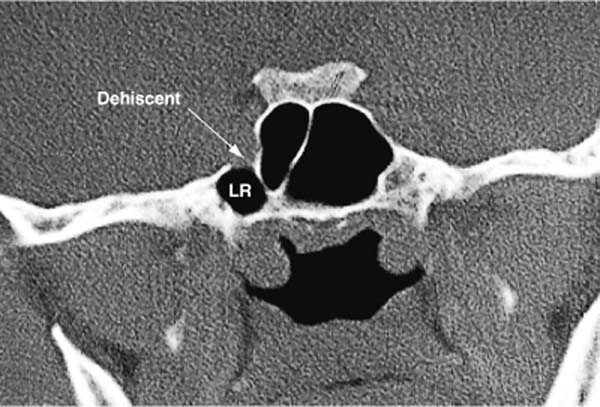
FIGURE 3–15 Large lateral recess (LR) of sphenoid. The presence of a dehiscence increases the risk of inadvertent carotid entry.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


