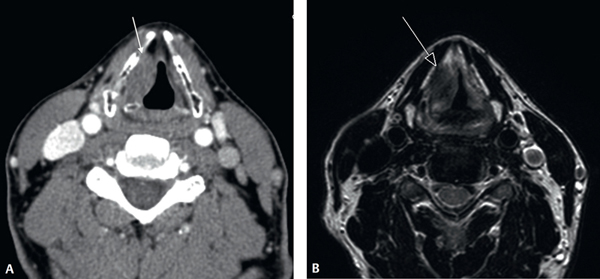
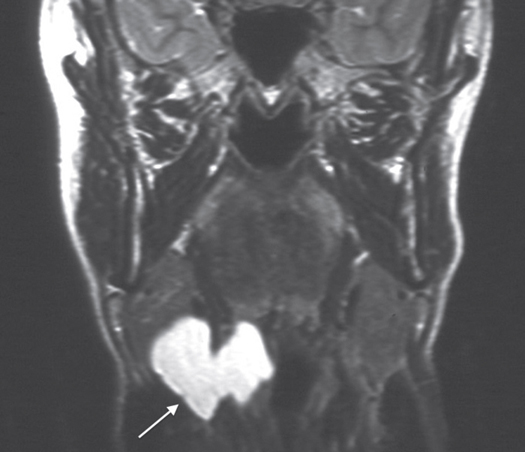
12 Imaging of the Larynx The evolution of modern imaging techniques, particularly over the past decade, has significantly improved the ability of the radiologist to visualize and assess laryngeal anatomy and disease. While the laryngologist is able to use modern endoscopy to evaluate mucosal surfaces, it is the radiologist’s role to elucidate the depth of submucosal disease extension through imaging as well as characterize the imaging appearances of such lesions. What is paramount, however, is that the findings of both clinical and radiological examinations are discussed and correlated together in an interdisciplinary setting to optimize benefit to the patient; it is also imperative that the radiologist has a good working knowledge of the descriptive anatomy used by the laryngologist. Historically, imaging techniques such as plain film tomography, laryngography, and barium swallow were the methods used for radiological depiction of laryngeal anatomy and disease. The majority of these techniques have fallen out of use, largely because of the development of computed tomography (CT) and magnetic resonance imaging (MRI). This was the first technique used to image the larynx. Soft-tissue lateral projections of the neck are still used in current modern-day practice as an overview to look for ingested, penetrated, or aspirated radiopaque foreign bodies (but usually as an adjunct to flexible nasendoscopy) and to assess gross airway patency. Conventional tomography was in routine use until toward the end of the 1980s but is now obsolete, superseded by CT and MRI. Cross-sectional imaging, either CT or MRI, has become essential for optimal pretreatment assessment of laryngeal disease, in particular neoplastic laryngeal pathology. Clinical evaluation allows the mucosal layer of the larynx to be defined; however, the deep extent of potentially infiltrating lesions can be assessed indirectly by clinical evaluation alone. Objective assessment of submucosal disease extension, disease volume, and involvement of the laryngeal cartilaginous skeleton can be achieved with CT and MRI cross-sectional imaging in cases of neoplastic and inflammatory disease.1–3 In acute traumatic and posttraumatic pathology, cross-sectional imaging, in particular CT, is useful in the evaluation of the laryngeal cartilaginous framework and soft tissues4–6; laryngeal and tracheal stenoses can be objectively documented with a view to planning of appropriate reconstructive surgery.7–11 Modern CT involves, in simplistic terms, the simultaneous translatory movement of a patient through a rotating X-ray source. If the CT scanner consists of multiple small X-ray sources with multiple detectors for the X-ray sources, this is termed multidetector helical CT. This multidetector helical technology is the current CT imaging technology of choice. Multidetector technology allows acquisition of faster scans of higher resolution. Probably the key consideration in CT is the fact that this imaging technology uses radiation. The patient undergoing CT assessment is exposed to a radiation dose (so are the radiation-sensitive tissues such as the thyroid gland)—this should always be borne in mind when request for CT assessment of the neck is made. To justify the radiation exposure to the patient, the benefit of the information yielded by the CT assessment must always outweigh the risks posed by the inherent radiation exposure. This is particularly the case if imaging assessment of the larynx is required in the pediatric population. There are several advantages of CT (relative to MRI) in imaging assessment of the larynx. CT is a faster technique—the imaging acquisition of the entire neck is of much shorter duration than MRI assessment of the larynx (the CT acquisition takes less than 30 seconds compared with 20 to 30 minutes for comprehensive MRI assessment of the soft tissues of the neck and larynx). Because the CT acquisition is a shorter scan time, the resultant images are less affected by motion degradation caused by swallowing or respiration, particularly in those patients who may already have labored breathing because of laryngeal airway pathology. CT is a relatively cheaper technology compared with MRI and, as such, is a more widely available imaging modality. Multidetector CT allows postprocessing generation of high-resolution multiplanar (coronal and sagittal) image reconstructions. Modern-day (multidetector helical) CT not only provides good soft-tissue contrast but also offers excellent depiction of osseous and calcific structures, which is particularly useful for demonstration of the ossified laryngeal cartilaginous skeleton. For many of the reasons outlined, CT is the first-line imaging modality of choice for assessing laryngeal pathology. An important nonsequitur to this is imaging assessment of the larynx in the nonsequitur pediatric population, where MRI may be an appropriate alternative for first-line imaging to avoid radiation exposure. Such considerations are best taken by the specialist radiologist. The majority of CT assessments of the larynx are best performed with the administration of intravenous contrast material (in those patients where renal function permits and there is no past history of allergic reaction to iodinated contrast material). Intravenous contrast medium increases the conspicuity of lesions of the larynx as well as allows better differentiation between lymph nodes and vessels in the extralaryngeal soft tissues of the neck. Multidetector CT images can be reconstructed to high quality along any plane, including a true axial orientation through the true and false vocal cords (Fig. 12.1). Although CT acquisitions can be obtained during specific dynamic maneuvers to enhance visualization of particular anatomical subsites (e.g., scan acquisition during a modified Valsalva maneuver distends the hypopharynx including the pyriform fossae and postcricoid region), acquisitions should generally be performed during quiet respiration by the patient to avoid adduction and approximation of the true vocal cords that hinders identification and delineation of superficial mucosal abnormalities. The basic principle of MRI employs the application of pulses of radiofrequency energy within a magnetic field. The nuclei of hydrogen atoms in water and fat (the predominant constituents of the human body) absorb and re-emit the radiofrequency energy. It is the re-emitted radiofrequency energy that is eventually translated into a contrast image of each particular tissue component. By varying the nature of the radiofrequency pulses applied, different sequences that highlight different tissue contrast characteristics can be obtained (Fig. 12.1). As an imaging modality, as with CT, there are several relatively advantageous and disadvantageous features of MRI. MRI scanners as well as the requisite hardware and software (in addition to the long-term maintenance) are expensive, far more so than CT. MRI is also a slower technique with comprehensive scan times of particular body regions lasting anything from 20 minutes to 45 minutes or more. As such, the quality of MR images is particularly prone to patient movement degradation and artifact. For anatomical regions where motion artifact may be an issue, this can be problematic. The laryngopharynx can be one such region. Inherent in the MRI technique is susceptibility to significant image artifact created by ferromagnetic material, which can have a major deleterious effect on image quality. Because of the nature of the strong magnetic fields related to MRI scanners (at present, 1.5 T and 3 T are routinely used clinically), there exist relative and absolute contraindications to MRI of particular patients; for example, patients with cardiac pacemakers cannot undergo an MRI (although the first generation of MR-“compatible” cardiac pacemakers may soon be available) and patients with ferromagnetic (typically steel) intraorbital foreign bodies, such as might occur as a frequent occupational hazard in metal workers, cannot undergo MR scan as such foreign bodies may be subject to movement in the strong magnetic field of the scanner. For those patients who have never had to endure an MRI scan of the head or neck region, the bore of the majority of current standard 1.5 T and 3 T MRI scanners is relatively small to maximize image quality. This can pose a very claustrophobic environment for even the most stoic individuals (let alone those prone to claustrophobia) required to lie in such a position for scan times of 30 minutes or more and, therefore, should not be underestimated; not infrequently, patients are unable to endure such scans even with oral sedation administered an hour before the MRI examination. One of the most salient advantages of MRI is that the technique does not involve the use of ionizing radiation, a particular advantage in the pediatric population. Other relative advantages of MRI include the relatively superior soft-tissue contrast detail of MRI over CT (although the detail of ossified structures such as bone and ossified cartilage is relatively less well served by MRI); the inherent orthogonal multiplanar capability of MRI (axial, sagittal, and coronal planes) is also advantageous. Figure 12.1 (A) Axial contrast-enhanced computed tomography image through the larynx of a 60-year-old man with hoarseness. There is a submucosal lesion in the right true and false cords (arrow) but no laryngeal cartilage destruction. The radiological features are not entirely typical of a neoplastic carcinoma. (B) Axial T2-weighted magnetic resonance (MR) sequence through the larynx of the same patient as in (A). The submucosal lesion in the right false and true cords (arrow) demonstrates MR signal characteristics and appearances consistent with amyloidosis. Microlaryngoscopy and biopsy confirmed amyloidosis. Swallowing and respiratory movement artifacts may seriously degrade the MRI study. The patient is therefore instructed to breathe quietly, in particular, without moving the neck. Patients are encouraged to use “abdominal” instead of “thoracic” respiration and to swallow as seldom as possible during individual scan sequence acquisitions. Axial and coronal planes are used in MRI of the larynx (Fig. 12.2). The axial planes should be angled in a plane parallel to the true vocal cords (equivalent to a plane parallel to the C4/5 and C5/6 cervical spine intervertebral disks). Where midline pathology is a consideration, sagittal plane MRI sequences should also be performed. The choice of sequences can be variable and will not be discussed in detail because it is beyond the scope of this discourse but will routinely incorporate the use of contrast-enhanced sequences where intravenous paramagnetic contrast material (gadolinium) is administered. In cases of malignant neoplastic pathology, this can increase the conspicuity of primary tumors as well as prove essential for the evaluation of cervical lymph nodes. Gadolinium is very rarely associated with allergic reaction and this is therefore rarely a consideration in contradistinction to iodinated contrast material used in CT. However, intravenous gadolinium contrast material is contraindicated in patients with renal impairment (because of the risk of nephrogenic systemic fibrosis).12–16 Figure 12.2 Coronal T2-weighted magnetic resonance sequence through the larynx in a 33-year-old female professional orchestral trumpet player demonstrates typical appearances of a right internal– external laryngocele (arrow).
Imaging Techniques
Historical Perspectives
Plain Film Radiography
Cross-Sectional Imaging
Computed Tomography
Technique
Magnetic Resonance Imaging
Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


