20 Imaging of the Ear • Describe areas of high or low attenuation • Uses conventional X-rays (ionizing radiation) with computer processing of digital information obtained from layer or spiral tomographs • For imaging of the temporal bone use high-resolution algorithm, bone windows, thin slices (0.5–1 mm); spiral scanning allows for multiplanar reformatting • Problems of partial volume averaging can apply to thin bony divisions, especially when slice thickness is higher • Describes areas as high or low signal intensity • Uses the magnetic properties of biological materials and generates images without the use of ionizing radiation • Tissues contain protons; apply strong magnetic field and these align, then impart energy (radio wave) to excite photons, which resonate; turn offradio wave and protons relax and in doing so give offa radio wave that is detected as the MR signal • Excellent for contrasting soft tissues: • Congenital atresia of EAC: CT scan can help with surgical planning • Osteomyelitis (malignant otitis externa): • ME effusion will often be an incidental finding on MRIs of brain; especially common in intubated patients; normally hyperintense on T2, hypointense on T1, non-enhancing with contrast • Routine assessment of COM best with CT, but intracranial complications (dural venous sinus thrombosis, abscesses, meningitis) best evaluated by MRI • Sigmoid sinus thrombosis: contrast-enhanced CT, acute thrombus hyperdense with contrast enhancing dura around thrombus (but not thrombus)—when chronic it revascularizes so enhances; hypo/isointense with flow voids on T1 and T2 MRI • Petrositis: CT—opacified cells and lysis of septations; MRI—meningeal enhancement where dura affected with hyperintensity on T2 (not T1) • Cholesterol granuloma: expansile cyst within pneumatized apex, so smooth expansion of cortical margins on CT; high signal on both T1 and T2 MRI (because high on T1, probably due to methemoglobin, distinguished from simple fluid, apicitis, cholesteatoma); can have hypointensity patches on both T1 and T2 • Cholesteatoma: • Neoplasia: CT shows irregular bony erosion for meningioma, glomus, chordoma, chondrosarcoma; smooth erosion for schwannoma, chondroma; metastases vary • To assess cochlear anomalies associated with SNHL, both CT and MRI help • Superior Scc dehiscence: both CT and T2 MRI can be reconstructed in plane and at right angles to plane of superior Scc to demonstrate defect • Precochlear implantation need to confirm a patent cochlea—both CRT and MRI helpful; MRI also provides information on the presence of VIII n • Halo sign may be seen around otic capsule in otosclerosis, with CT • CT for trauma • CT also best for bony dysplasias, e.g., fibrous dysplasia with ground glass appearance yet sparing of the otic capsule • Glomus tumours: CT and MRI helpful; CT gives bony anatomy and extent of bony erosion; rapid flow in intratumoural vessels may appear as black flow voids resulting in a “salt and pepper” appearance; hypo/isointense on T1, hyperintense on T2, enhances dramatically on postcontrast T1 (because of high vascularity) • Pulsatile tinnitus may prompt imaging to identify vascular anomalies; in addition to MRI, MR angiography may help define anomalous vasculature, and MR venography may identify venous thrombosis; objective tinnitus should prompt catheter angiography when suspicion is high for a vascular lesion such as dural arteriovenous fistulas • MRI is the gold standard for evaluating the IAC and CPA • Vestibular schwannoma: usually isointense to hypointense to brain, hyperintense to CSF on T1 and isointense to slightly hyperintense on T2; best shown with T1 contrast (Gd); enhanced T1 images usually show a homogeneously enhancing mass centred near the porus acousticus with IAC extension; both high-resolution T2 and contrast-enhanced T1 can detect extremely small lesions (2 mm); both cystic and haemorrhagic areas may be seen associated with larger tumours, but calcification is rare; when MRI contraindicated, >90% will enhance homogeneously with CT with contrast; CT may also show dilation of IAC
20.1 Imaging Modalities
20.1.1 Computed Tomography (CT)
20.1.2 Magnetic Resonance Imaging (MRI)
 T1: good for anatomy; fluid (water, CSF, vitreous, mucus) black; fat white; hyperintense structures most likely fat, protein, methemoglobin, or contrast
T1: good for anatomy; fluid (water, CSF, vitreous, mucus) black; fat white; hyperintense structures most likely fat, protein, methemoglobin, or contrast
 T2: good for pathology; fluid (water, vitreous, CSF) white; pathological tissue usually bright; fat, muscle intermediate; blood variable; air, bone, rapid vascular flow black
T2: good for pathology; fluid (water, vitreous, CSF) white; pathological tissue usually bright; fat, muscle intermediate; blood variable; air, bone, rapid vascular flow black
 STIR: (short tau inversion recovery) suppresses fat to help show tumour; applied to T2 images; water white, fat black
STIR: (short tau inversion recovery) suppresses fat to help show tumour; applied to T2 images; water white, fat black
 Can fat suppress either T1 or T2; latter fat-suppressed virtually indistinguishable from T2 STIR sequence
Can fat suppress either T1 or T2; latter fat-suppressed virtually indistinguishable from T2 STIR sequence
 Gadolinium can be used as contrast
Gadolinium can be used as contrast
 Various other sequences can help manipulate image, e.g., FIESTA (fast imaging employing steady-state acquisition), which allows fast acquisition of thin slice information that is good for spatial resolution at expense of contrast resolution
Various other sequences can help manipulate image, e.g., FIESTA (fast imaging employing steady-state acquisition), which allows fast acquisition of thin slice information that is good for spatial resolution at expense of contrast resolution
 DWI (diffusion-weighted imaging): looks at how water moves through cells; “dead” cells (e.g., post-CVA) trap water (so restrict diffusion) showing up as high intensity, as does keratin, so useful for epidermoid cysts and cholesteatoma; echo-planar (EPI) and non-echo-planar imaging types
DWI (diffusion-weighted imaging): looks at how water moves through cells; “dead” cells (e.g., post-CVA) trap water (so restrict diffusion) showing up as high intensity, as does keratin, so useful for epidermoid cysts and cholesteatoma; echo-planar (EPI) and non-echo-planar imaging types
20.2 Imaging of Ear Pathology
20.2.1 External Ear
 CT with contrast yields bony detail; coronal CT may show effacement of the tympanic ring
CT with contrast yields bony detail; coronal CT may show effacement of the tympanic ring
 MRI (± gadolinium) can define medial extent of soft tissue disease at the skull base, dural enhancement and cerebral involvement
MRI (± gadolinium) can define medial extent of soft tissue disease at the skull base, dural enhancement and cerebral involvement
 Technetium-99 m bone scanning and gallium-67 scanning helpful; their sensitivity for the presence of infection is far greater than their specificity for the cause
Technetium-99 m bone scanning and gallium-67 scanning helpful; their sensitivity for the presence of infection is far greater than their specificity for the cause
 Tc-99 m gives excellent information about bone function (but poor for bone structure); +ve scan thought to represent osteoblastic activity as little as 10% above normal; +ve in acute and chronic osteomyelitis and in areas of active bone repair without infection (e.g., trauma); increases in Tc-99 m uptake between 4 and 24 h post-injection is the most sensitive indicator of temporal bone osteomyelitis
Tc-99 m gives excellent information about bone function (but poor for bone structure); +ve scan thought to represent osteoblastic activity as little as 10% above normal; +ve in acute and chronic osteomyelitis and in areas of active bone repair without infection (e.g., trauma); increases in Tc-99 m uptake between 4 and 24 h post-injection is the most sensitive indicator of temporal bone osteomyelitis
 Ga-67 will highlight an acute infective focus but not the full extent of an osteomyelitic process; as treatment progresses the scan will revert to normal (Tc-99 m will lag behind for months)
Ga-67 will highlight an acute infective focus but not the full extent of an osteomyelitic process; as treatment progresses the scan will revert to normal (Tc-99 m will lag behind for months)
 Baseline studies of both thus considered, and sequential imaging is used to monitor the response to therapy
Baseline studies of both thus considered, and sequential imaging is used to monitor the response to therapy
 Indium-111 labeled leucocyte planar scintigraphy can yield even better results for detection of osteomyelitis and may replace above
Indium-111 labeled leucocyte planar scintigraphy can yield even better results for detection of osteomyelitis and may replace above
20.2.2 Middle Ear/Mastoid, Petrous Apex
 CT most helpful to see pattern of bony destruction, but cannot differentiate cholesteatoma from other soft tissue; key features: scutum, lateral Scc, ossicular chain (e.g., long process of incus) erosion
CT most helpful to see pattern of bony destruction, but cannot differentiate cholesteatoma from other soft tissue; key features: scutum, lateral Scc, ossicular chain (e.g., long process of incus) erosion
 May be helpful in surgical planning, e.g., a small mastoid or low tegmen might mean canal wall up surgery is difficult and atticoantrostomy is better indicated
May be helpful in surgical planning, e.g., a small mastoid or low tegmen might mean canal wall up surgery is difficult and atticoantrostomy is better indicated
 MRI late T1 Gd get rim enhancement with non-enhancing cholesteatoma (keratin)—inflammatory tissue, granulation enhances; sequence takes 45 min but can show lesions down to 3 mm
MRI late T1 Gd get rim enhancement with non-enhancing cholesteatoma (keratin)—inflammatory tissue, granulation enhances; sequence takes 45 min but can show lesions down to 3 mm
 T2 moderately hyperintense and can differentiate cholesteatoma from brain herniation if dehiscent tegmen
T2 moderately hyperintense and can differentiate cholesteatoma from brain herniation if dehiscent tegmen
 DWI EPI: detects lesions ≥5 mm, high signal; but temporal lobe artifact
DWI EPI: detects lesions ≥5 mm, high signal; but temporal lobe artifact
 DWI non-EPI: lesions 2 mm+, less artefact, poor bony anatomy; may be suitable to screen before 2nd-look canal wall up surgery
DWI non-EPI: lesions 2 mm+, less artefact, poor bony anatomy; may be suitable to screen before 2nd-look canal wall up surgery
20.2.3 Inner Ear
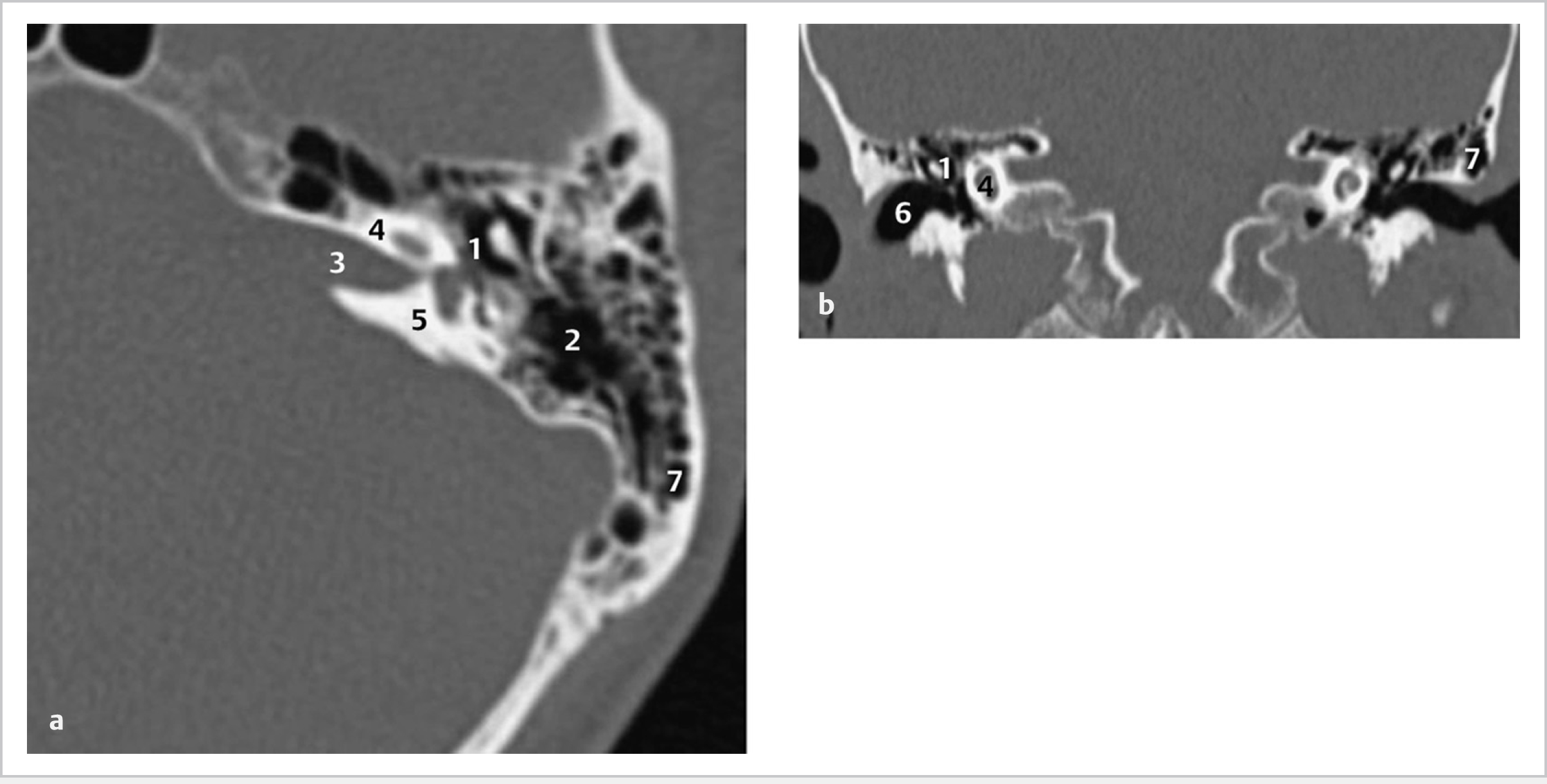
20.2.4 Temporal Bone (Fig. 20.1)
20.2.5 Internal Auditory Canal, Skull Base
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


